Methylphenidate
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Ritalin, Concerta, Aptensio, Biphentin, Daytrana, Equasym, Medikinet, Metadate, Methylin, QuilliChew, Quillivant |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a682188 |
| License data |
|
| Pregnancy category | |
| Dependence liability |
Physical: None Psychological: Moderate |
| Addiction liability | Moderate |
| Routes of administration | Oral, insufflation, intravenous, transdermal |
| ATC code | N06BA04 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | ~30% (range: 11–52%) |
| Protein binding | 10–33% |
| Metabolism | Liver (80%) mostly CES1A1-meditated |
| Biological half-life | 2–3 hours[1] |
| Excretion | Urine (90%) |
| Identifiers | |
| |
| CAS Number |
113-45-1 |
| PubChem (CID) | 4158 |
| IUPHAR/BPS | 7236 |
| DrugBank |
DB00422 |
| ChemSpider |
4015 |
| UNII |
207ZZ9QZ49 |
| KEGG |
D04999 |
| ChEBI |
CHEBI:6887 |
| ChEMBL |
CHEMBL796 |
| Chemical and physical data | |
| Formula | C14H19NO2 |
| Molar mass | 233.31 g/mol |
| 3D model (Jmol) | Interactive image |
| Melting point | 74 °C (165 °F) [2] |
| Boiling point | 136 °C (277 °F) [2] |
| |
| |
| (verify) | |
Methylphenidate, sold under various trade names, Ritalin being one of the most commonly known, is a central nervous system (CNS) stimulant of the phenethylamine[3] and piperidine classes that is used in the treatment of attention deficit hyperactivity disorder (ADHD) and narcolepsy. The original patent was owned by CIBA, now Novartis Corporation. It was first licensed by the US Food and Drug Administration (FDA) in 1955 for treating what was then known as hyperactivity.
Medical use began in 1960; the drug has become increasingly prescribed since the 1990s, when the diagnosis of ADHD became more widely accepted.[4][5] Between 2007 and 2012 methylphenidate prescriptions increased by 50% in the United Kingdom and in 2013 global methylphenidate consumption increased to 2.4 billion doses, a 66% increase from the year before. The United States continues to account for more than 80% of global consumption.[6][7]
ADHD and other similar conditions are believed to be linked to sub-performance of the dopamine and norepinephrine functions in the brain, primarily in the prefrontal cortex, responsible for executive function (e.g., reasoning, inhibiting behaviors, organizing, problem solving, planning, etc.).[8][9] Methylphenidate's mechanism of action involves the inhibition of catecholamine reuptake, primarily as a dopamine reuptake inhibitor. Methylphenidate acts by blocking the dopamine transporter and norepinephrine transporter, leading to increased concentrations of dopamine and norepinephrine within the synaptic cleft. This effect in turn leads to increased neurotransmission of dopamine and norepinephrine.[10] Methylphenidate is also a weak 5HT1A receptor agonist.[11]
Uses
Medical
Methylphenidate is a commonly prescribed psychostimulant and works by increasing the activity of the central nervous system.[12] It produces such effects as increasing or maintaining alertness, combating fatigue, and improving attention.[13] The short-term benefits and cost effectiveness of methylphenidate are well established.[14][15] Methylphenidate is not approved for children under six years of age.[16][17] Methylphenidate may also be prescribed for off-label use in treatment-resistant cases of bipolar disorder and major depressive disorder.[18]
Meta-analyses and systematic reviews of magnetic resonance imaging studies suggest that long-term treatment with ADHD stimulants (specifically, amphetamine and methylphenidate) decreases abnormalities in brain structure and function found in subjects with ADHD.[19][20][21] Moreover, reviews of clinical stimulant research have established the safety and effectiveness of the long-term use of ADHD stimulants for individuals with ADHD.[22][23] In particular, the continuous treatment effectiveness and safety of both amphetamine and methylphenidate have been demonstrated in controlled drug trials with durations of several years;[23][24] however, the precise magnitude of improvements in ADHD symptoms and quality of life that are produced by methylphenidate treatment remains uncertain as of November 2015.[25]
Attention deficit hyperactivity disorder
Methylphenidate is approved by the US Food and Drug Administration (FDA) for the treatment of attention deficit hyperactivity disorder.[26] The addition of behavioural modification therapy (e.g. cognitive behavioral therapy (CBT)) can have additional benefits on treatment outcome.[27][28] The dosage used can vary quite significantly among individuals; consequently, dosage must be titrated precisely.[29]
Current models of ADHD suggest that it is associated with functional impairments in some of the brain's neurotransmitter systems,[note 1] particularly those involving dopamine and norepinephrine.[30] Psychostimulants like methylphenidate and amphetamine may be effective in treating ADHD because they increase neurotransmitter activity in these systems.[30] Approximately 70% of those who use these stimulants see improvements in ADHD symptoms.[31][32] Children with ADHD who use stimulant medications generally have better relationships with peers and family members,[22][31] generally perform better in school, are less distractible and impulsive, and have longer attention spans.[22][31] People with ADHD have an increased risk of substance use disorders, and stimulant medications reduce this risk.[33][34]
Narcolepsy
Narcolepsy, a chronic sleep disorder characterized by overwhelming daytime drowsiness and sudden need for sleep, is treated primarily with stimulants. Methylphenidate is considered effective in increasing wakefulness, vigilance, and performance.[35] Methylphenidate improves measures of somnolence on standardized tests, such as the Multiple Sleep Latency Test, but performance does not improve to levels comparable to healthy controls.[36]
Other
Methylphenidate may be used in addition to an antidepressant for refractory major depressive disorder. It can also improve depression in several groups including stroke, cancer, and HIV-positive patients.[37] However, the use of stimulants such as methylphenidate in cases of treatment-resistant depression is controversial.[38] Stimulants may have fewer side-effects than tricyclic antidepressants in the elderly and medically ill.[39] In individuals with terminal cancer, methylphenidate can be used to counteract opioid-induced somnolence, to increase the analgesic effects of opioids, to treat depression, and to improve cognitive function.[40]
Enhancing performance
In 2015, a systematic review and a meta-analysis of high quality clinical trials found that therapeutic doses of amphetamine and methylphenidate result in modest yet unambiguous improvements in cognition, including working memory, episodic memory, and inhibitory control, in normal healthy adults;[41][42] the cognition-enhancing effects of these drugs are known to occur through the indirect activation of both dopamine receptor D1 and adrenoceptor α2 in the prefrontal cortex.[41] Methylphenidate and other ADHD stimulants also improve task saliency and increase arousal.[43][44] Stimulants such as amphetamine and methylphenidate can improve performance on difficult and boring tasks,[43][44] and are used by some students as a study and test-taking aid.[45] Based upon studies of self-reported illicit stimulant use, performance-enhancing use, rather than use as a recreational drug, is the primary reason that students use stimulants.[46] Excessive doses of methylphenidate, above the therapeutic range, can interfere with working memory and cognitive control.[43][44] Like amphetamine and bupropion, methylphenidate increases stamina and endurance in humans primarily through reuptake inhibition of dopamine in the central nervous system.[47] Similar to the loss of cognitive enhancement when using large amounts, large doses of methylphenidate can induce side effects that impair athletic performance, such as rhabdomyolysis and hyperthermia.[48]
Ethics of use for performance enhancement
Methylphenidate is sometimes used by students to enhance their mental abilities, improving their concentration and helping them to study.
John Harris, an expert in bioethics, has said that it would be unethical to stop healthy people taking the drug. He pointed out the logical non sequitur which would result if people were to draw a parallel between the claims of a university that they could "set out deliberately to improve the mental capacities of its students; suppose its stated aims were to ensure that students left the university more intelligent and learned than when they arrived. Suppose they further claimed that not only could they achieve this but that their students would be more intelligent and mentally alert than any students in history." He then asked the rhetorical question of whether, "if the claims could be sustained, should we be pleased?" He argues that it would be "not rational" and against human enhancement to not use the drug to improve people's cognitive abilities.[49]
Barbara Sahakian has argued that the use of Ritalin in this way may give students an unfair advantage in examinations and that as a result universities may want to discuss making students give urine samples to be tested for the drug.[50]
Contraindications
Methylphenidate is contraindicated for individuals using monoamine oxidase inhibitors (e.g., phenelzine and tranylcypromine), or individuals with agitation, tics, or glaucoma, or a hypersensitivity to any ingredients contained in methylphenidate pharmaceuticals.[51]
The US FDA gives methylphenidate a pregnancy category of C, and women are advised to only use the drug if the benefits outweigh the potential risks.[52] Not enough animal and human studies have been conducted to conclusively demonstrate an effect of methylphenidate on fetal development. In 2007, empirical literature included 63 cases of prenatal exposure to methylphenidate across three empirical studies.[53]
Adverse effects
Methylphenidate is generally well tolerated.[55][56] The most commonly observed adverse effects with a frequency greater than placebo include appetite loss, dry mouth, anxiety/nervousness, nausea, and insomnia. Gastrointestinal adverse effects may include abdominal pain and weight loss. Nervous system adverse effects may include akathisia (agitation/restlessness), irritability, dyskinesia (tics), lethargy (drowsiness/fatigue), and dizziness. Cardiac adverse effects may include palpitations, changes in blood pressure and heart rate (typically mild), and tachycardia (rapid resting heart rate). Ophthalmologic adverse effects may include blurred vision and dry eyes, with less frequent reports of diplopia and mydriasis.[57] Other adverse effects may include depression, emotional lability, confusion, and bruxism. Hyperhidrosis (increased sweating) is common. Chest pain is rarely observed.[58]
There is some evidence of mild reductions in growth rate with prolonged treatment in children, but no causal relationship has been established and reductions do not appear to persist long-term.[59] Hypersensitivity (including skin rash, urticaria, and fever) is sometimes reported. The Daytrana patch has a much higher rate of dermal reactions than oral methylphenidate.[60]
Methylphenidate can worsen psychosis in psychotic patients, and in very rare cases it has been associated with the emergence of new psychotic symptoms.[61] It should be used with extreme caution in patients with bipolar disorder due to the potential induction of mania or hypomania.[62] There have been very rare reports of suicidal ideation, but evidence does not support a link.[59] Logorrhea is occasionally reported. Libido disorders, disorientation, and hallucinations are very rarely reported. Priapism is a very rare adverse event that can be potentially serious.[63]
USFDA-commissioned studies from 2011 indicate that in children, young adults, and adults there is no association between serious adverse cardiovascular events (sudden death, heart attack, and stroke) and the medical use of methylphenidate or other ADHD stimulants.[64]
Because some adverse effects may only emerge during chronic use of methylphenidate, a constant watch for adverse effects is recommended.[65]
Overdose
The symptoms of a moderate acute overdose on methylphenidate primarily arise from central nervous system overstimulation; these symptoms include: vomiting, agitation, tremors, hyperreflexia, muscle twitching, euphoria, confusion, hallucinations, delirium, hyperthermia, sweating, flushing, headache, tachycardia, heart palpitations, cardiac arrhythmias, hypertension, mydriasis, and dryness of mucous membranes.[48][66] A severe overdose may involve symptoms such as hyperpyrexia, sympathomimetic toxidrome, convulsions, paranoia, stereotypy (a repetitive movement disorder), rapid muscle breakdown, coma, and circulatory collapse.[48][66][67] A methylphenidate overdose is rarely fatal with appropriate care.[67] Severe toxic reactions involving abscess and necrosis have been reported following injection of methylphenidate tablets into an artery.[68]
Treatment of a methylphenidate overdose typically involves the application of benzodiazepines, with antipsychotics, α-adrenoceptor agonists, and propofol serving as second-line therapies.[67]
Addiction and dependence
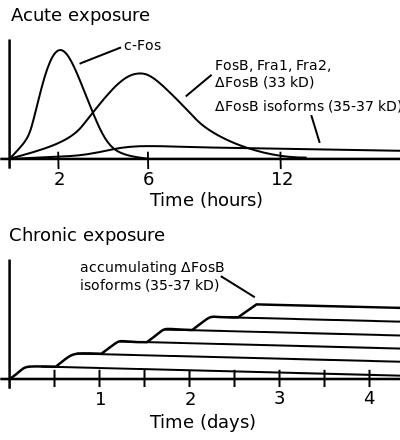
Bottom: this diagram illustrates increasing ΔFosB expression from repeated twice daily drug binges, where these phosphorylated (35–37 kD) ΔFosB isoforms persist in the D1-type medium spiny neurons of the nucleus accumbens for up to 2 months following drug exposure.[69][70]
Pharmacological texts describe methylphenidate as a stimulant with effects, addiction liability, and dependence liability similar to the amphetamine, a compound with moderate liability among addictive drugs;[71][72] accordingly, addiction and psychological dependence are possible and likely when methylphenidate is used at high doses as a recreational drug.[72][73] When used above the medical dose range, stimulants are associated with the development of stimulant psychosis.[74] As with all addictive drugs, the overexpression of ΔFosB in D1-type medium spiny neurons in the nucleus accumbens is implicated in methylphenidate addiction.[73][75]
Methylphenidate has shown some benefits as a replacement therapy for individuals who are addicted to and dependent upon methamphetamine.[76] Methylphenidate and amphetamine have been investigated as a chemical replacement for the treatment of cocaine addiction[77][78][79][80] in the same way that methadone is used as a replacement drug for physical dependence upon heroin. Its effectiveness in treatment of cocaine or psychostimulant addiction or psychological dependence has not been proven and further research is needed.[81]
Biomolecular mechanisms
Methylphenidate has the potential to induce euphoria due to its pharmacodynamic effect (i.e., dopamine reuptake inhibition) in the brain's reward system.[75] At therapeutic doses, ADHD stimulants do not sufficiently activate the reward system, or the reward pathway in particular, to induce persistent ΔFosB gene expression in the D1-type medium spiny neurons of the nucleus accumbens;[72][75][82] consequently, when used medically and as directed, methylphenidate use has no capacity to cause an addiction.[72][75][82] However, when methylphenidate is used at sufficiently high recreational doses through a bioavailable route of administration (e.g., insufflation or intravenous administration), particularly for use of the drug as a euphoriant, ΔFosB accumulates in the nucleus accumbens.[72][75] Hence, like any other addictive drug, regular recreational use of methylphenidate at high doses eventually gives rise to ΔFosB overexpression in D1-type neurons which subsequently triggers a series of gene transcription-mediated signaling cascades that induce an addiction.[75][82][83][84][85]
Interactions
Methylphenidate may inhibit the metabolism of coumarin anticoagulants, certain anticonvulsants, and some antidepressants (tricyclic antidepressants and selective serotonin reuptake inhibitors). Concomitant administration may require dose adjustments, possibly assisted by monitoring of plasma drug concentrations.[56] There are several case reports of methylphenidate inducing serotonin syndrome with concomitant administration of antidepressants.[86][87][88][89]
When methylphenidate is coingested with ethanol, a metabolite called ethylphenidate is formed via hepatic transesterification,[90][91] not unlike the hepatic formation of cocaethylene from cocaine and alcohol. The reduced potency of ethylyphenidate and its minor formation means it does not contribute to the pharmacological profile at therapeutic doses and even in overdose cases ethylphenidate concentrations remain negligible.[12][92]
Coingestion of alcohol (ethanol) also increases the blood plasma levels of d-methylphenidate by up to 40%.[93]
Liver toxicity from methylphenidate is extremely rare, but limited evidence suggests that intake of β-adrenergic agonists with methylphenidate may increase the risk of liver toxicity.[94]
Pharmacology
Pharmacodynamics
| Receptor | Ki (nM) dl-MPH | Ki (nM) d-MPH | Ki (nM) l-MPH |
|---|---|---|---|
| DAT | 121 | 161 | 2250 |
| NET | 788 | 206 | >10,000 |
| SERT | >10,000 | >10,000 | >6700 |
| 5-HT1A | 5000 | 3400 | >10,000 |
| 5-HT2B | >10,000 | 4700 | >10,000 |
Methylphenidate primarily acts as a norepinephrine–dopamine reuptake inhibitor (NDRI). It is a benzylpiperidine and phenethylamine derivative which also shares part of its basic structure with catecholamines.
Methylphenidate is most active at modulating levels of dopamine and to a lesser extent norepinephrine.[98] Methylphenidate binds to and blocks dopamine transporters and norepinephrine transporters.[99]
Both amphetamine and methylphenidate are predominantly dopaminergic drugs, yet their methods of action are distinct. Methylphenidate acts as a norepinephrine–dopamine reuptake inhibitor while amphetamine is both a releasing agent and reuptake inhibitor of dopamine and norepinephrine. Methylphenidate's mechanism of action in the release of dopamine and norepinephrine is fundamentally different from most other phenethylamine derivatives, as methylphenidate is thought to increase general firing rate,[100][101][102][103] whereas amphetamine reduces firing rate and reverses the flow of the monoamines via TAAR1 activation.[104]
Methylphenidate has both dopamine transporter and norepinephrine transporter binding affinity, with the dextromethylphenidate enantiomers displaying a prominent affinity for the norepinephrine transporter. Both the dextrorotary and levorotary enantiomers displayed receptor affinity for the serotonergic 5HT1A and 5HT2B subtypes, though direct binding to the serotonin transporter was not observed.[97] A later study confirmed the d-threo- enantiomer binding to the 5HT1A receptor, but no significant activity on the 5HT2B receptor was found.[105]
Methylphenidate may protect neurons from the neurotoxic effects of Parkinson's disease and methamphetamine abuse.[106]
The dextrorotary enantiomers are significantly more potent than the levorotary enantiomers, and some medications therefore only contain dexmethylphenidate.[98]
Methylphenidate has been identified as a sigma-1 receptor agonist.[107]
Pharmacokinetics
Methylphenidate taken orally has a bioavailability of 11–52% with a duration of peak action around 2–4 hours for instant release (i.e. Ritalin), 3–8 hours for sustained release (i.e. Ritalin SR), and 8–12 hours for extended release (i.e. Concerta). The half-life of methylphenidate is 2–3 hours, depending on the individual. The peak plasma time is achieved at about 2 hours.[1]
Dextromethylphenidate is much more bioavailable than levomethylphenidate when administered orally, and is primarily responsible for the psychoactivity of racemic methylphenidate.[1]
Contrary to the expectation, taking methylphenidate with a meal speeds absorption.[108]
Methylphenidate is metabolized into ritalinic acid by CES1A1. Dextromethylphenidate is selectively metabolized at a slower rate than levomethylphenidate.[109]
Chemistry
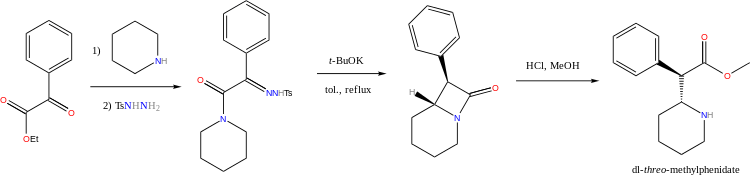
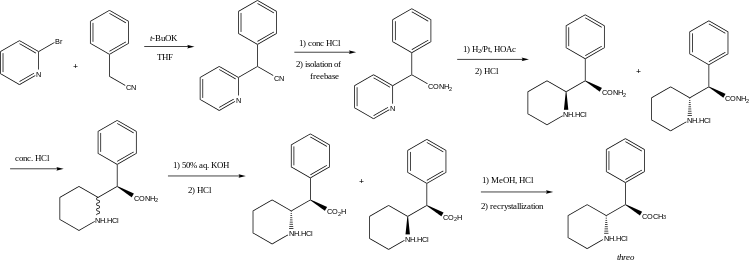
Four isomers of methylphenidate are possible, since the molecule has two chiral centers. One pair of threo isomers and one pair of erythro are distinguished, from which only d-threo-methylphenidate exhibits the pharmacologically usually desired effects.[98][110] When the drug was first introduced it was sold as a 3:1 mixture of erythro:threo diastereomers. The erythro diastereomers are also pressor amines. "TMP" is referring only to the threo product that does not contain any erythro diastereomers. Since the threo isomers are energetically favored, it is easy to epimerize out any of the undesired erythro isomers. The drug that contains only dextrorotary methylphenidate is called d-TMP. A review on the synthesis of enantiomerically pure (2R,2'R)-(+)-threo-methylphenidate hydrochloride has been published.[111]
Detection in biological fluids
The concentration of methylphenidate or ritalinic acid, its major metabolite, may be quantified in plasma, serum or whole blood in order to monitor compliance in those receiving the drug therapeutically, to confirm the diagnosis in potential poisoning victims or to assist in the forensic investigation in a case of fatal overdosage.[114]
Pharmaceutical products
Names

Methylphenidate is produced in the United States, Mexico, Spain, Sweden, Pakistan, and India. It is also sold in Canada, Australia, the United Kingdom, Spain, Germany, Belgium, Brazil, Portugal, Argentina, Thailand, and several other European countries (although in much lower volumes than in the United States). Brand names for methylphenidate include Ritalin, Concerta, Aptensio, Biphentin, Daytrana, Equasym, Medikinet, Metadate, Methylin, and Quillivant. Generic forms are produced by numerous pharmaceutical companies throughout the world. In Belgium the product is sold under the name Rilatine and in Brazil, Portugal and Argentina as Ritalina. In Thailand, it is found under the name Hynidate. In India, it is found under the names Addwize and Inspiral SR.
The dextrorotary enantiomer of methylphenidate, known as dexmethylphenidate, is sold as a generic and under the brand names Focalin and Attenade.
Available forms

Methylphenidate is available in numerous forms, a doctor will prescribe the appropriate method based on patient feedback and product availability. Current available forms are tablet, capsule, adhesive-based matrix transdermal system (patch), and oral suspension (liquid syrup).
Immediate-release

Methylphenidate was originally available as an immediate-release racemic mixture formulation under the Novartis trademark name Ritalin, although a variety of generics are now available, some under other brand names. Generic brand names include Ritalina, Rilatine, Attenta, Medikinet, Metadate, Methylin, Penid, Tranquilyn, and Rubifen.
Extended-release
Extended-release methylphenidate products include:
| Brand name(s) | Generic name(s)[115][116][117][118] | Duration | Product format |
|---|---|---|---|
| Aptensio XR (US); Biphentin (CA) |
12 hours[119][120] | Pill (capsule) | |
| Concerta (US/CA); Concerta XL (UK) |
Actavis Methylphenidate ER (US); Teva-Methylphenidate ER‑C (CA); pms-Methylphenidate ER (CA) |
12 hours[121] | Pill (OROS tablet) |
| Quillivant XR | 12 hours[121] | Oral suspension | |
| Daytrana | 11 hours[122] | Transdermal patch | |
| Metadate CD (US); Equasym XL (UK) |
Corepharma methylphenidate ER (US); Mallinckrodt methylphenidate ER (US); Teva methylphenidate ER (US) |
8–10 hours[121] | Pill (capsule) |
| QuilliChew ER (US) | 8 hours | Tablet (chewable) | |
| Ritalin LA (US); Medikinet XL (UK) |
Barr methylphenidate ER (US); Mayne methylphenidate ER (US) |
8 hours[121] | Pill (capsule) |
| Ritalin SR (US/CA/UK); Rubifen SR (NZ) |
Metadate ER (US); Methylin ER (US); methylphenidate SR (US/CA) |
5–8 hours[121] | Pill (CR tablet) |
Concerta tablets are marked with the letters "ALZA" and followed by: "18", "27", "36", or "54", relating to the mg dosage strength. Approximately 22% of the dose is immediate release,[123] and the remaining 78% of the dose is released over 10–12 hours post ingestion, with an initial increase over the first 6 to 7 hours, and subsequent decline in released drug.[124]
Ritalin LA capsules are marked with the letters "NVR" (abbrev.: Novartis) and followed by: "R20", "R30", or "R40", depending on the (mg) dosage strength. Ritalin LA[125] provides two standard doses – half the total dose being released immediately and the other half released four hours later. In total, each capsule is effective for about eight hours.
Metadate CD capsules contain two types of beads; 30% are immediate release, and the other 70% are evenly sustained release.[126]
Quillivant XR is an extended-release oral suspension (after reconstitution with water): 25 mg per 5 mL (5 mg per mL). It was designed and is patented and made by Pfizer. The medication comes in various sizes from 60ml to 180ml (after reconstitution). Each bottle is shipped with the medication in powder form containing roughly 20% instant-release and 80% extended-release methylphenidate, to which water must be added by the pharmacist in an amount corresponding with the total intended volume of the bottle. The bottle must be shaken vigorously for ten seconds prior to administration via included oral syringe to ensure proper ratio.[127]
Cost
Generic immediate-release methylphenidate is relatively inexpensive. The average wholesale cost is about US$0.15 per defined daily dose (retail pharmacies normally charge more).[128] However, the priciest brand-name extended-release tablets may retail for as much as $12.40 per defined daily dose.[129]
There are two main reasons for this price difference:
- Generic formulations are cheaper than brand-name formulations.
- Immediate-release tablets are cheaper than 8-hour extended-release tablets, which in turn are much cheaper than 12-hour extended-release tablets.
History, society, and culture
Methylphenidate was first synthesized in 1944,[130] and was identified as a stimulant in 1954.[131]
Methylphenidate was synthesized by Ciba (now Novartis) chemist Leandro Panizzon. His wife, Marguerite, had low blood pressure and would take the drug as a stimulant before playing tennis. He named the substance Ritaline, after his wife's nickname, Rita.[132]
Originally it was marketed as a mixture of two racemates, 80% (±)-erythro and 20% (±)-threo. Subsequent studies of the racemates showed that the central stimulant activity is associated with the threo racemate and were focused on the separation and interconversion of the erythro isomer into the more active threo isomer.[133][134][135]
Methylphenidate was first used to allay barbiturate-induced coma, narcolepsy and depression.[132] It was later used to treat memory deficits in the elderly.[136] Beginning in the 1960s, it was used to treat children with ADHD or ADD, known at the time as hyperactivity or minimal brain dysfunction (MBD) based on earlier work starting with the studies by American psychiatrist Charles Bradley[137] on the use of psychostimulant drugs, such as benzedrine, with then called "maladjusted children".[138] Production and prescription of methylphenidate rose significantly in the 1990s, especially in the United States, as the ADHD diagnosis came to be better understood and more generally accepted within the medical and mental health communities.[139]
In 2000 ALZA Corporation received US Food and Drug Administration (FDA) approval to market "Concerta", an extended-release form of methylphenidate.[140] See the "Extended-release" section of this article, above, for more information about Concerta.
Legal status

- Internationally, methylphenidate is a Schedule II drug under the Convention on Psychotropic Substances.[141]
- In the United States, methylphenidate is classified as a Schedule II controlled substance, the designation used for substances that have a recognized medical value but present a high potential for abuse.
- In the United Kingdom, methylphenidate is a controlled 'Class B' substance. Possession without prescription carries with a sentence up to 5 years and/or an unlimited fine, and supplying it is 14 years and/or an unlimited fine.[142]
- In Canada, methylphenidate is listed in Schedule III of the Controlled Drugs and Substances Act (along with LSD, psychedelic mushrooms, and mescaline, among others), and is illegal to possess without a prescription, pursuant to Part G (section G.01.002) of the Food and Drug Regulations under the Food and Drugs Act.
- In New Zealand, methylphenidate is a 'class B2 controlled substance'. Unlawful possession is punishable by six-month prison sentence and distribution of it is punishable by a 14-year sentence.
- In Australia, methylphenidate is a 'Schedule 8' controlled substance.[143] Such drugs must be kept in a lockable safe before being handed out and possession without prescription carries hefty fines and even imprisonment.
- In Sweden, methylphenidate is a List II controlled substance with recognized medical value. Possession without a prescription is punishable by up to three years in prison.[144]
- In France, methylphenidate is covered by the "narcotics" schedule, prescription and distribution conditions are restricted with hospital-only prescription for the initial treatment and yearly consultations.[145]
- In India, methylphenidate is a schedule X drug and is controlled by the Drugs and Cosmetics Rule, 1945. It is given only under a prescription from a neurologist or a psychiatrist [146]
Controversy
Methylphenidate has been the subject of controversy in relation to its use in the treatment of ADHD. The prescription of psychostimulant medication to children to reduce ADHD symptoms has been a major point of criticism.[147] The contention that methylphenidate acts as a gateway drug has been discredited by multiple sources,[148] according to which abuse is statistically very low and "stimulant therapy in childhood does not increase the risk for subsequent drug and alcohol abuse disorders later in life".[149] A study found that ADHD medication was not associated with increased risk of cigarette use, and in fact stimulant treatments such as Ritalin seemed to lower this risk.[150]
Treatment of ADHD by way of methylphenidate has led to legal actions including malpractice suits regarding informed consent, inadequate information on side effects, misdiagnosis, and coercive use of medications by school systems.[151] In the US and the UK, it is approved for use in children and adolescents. In the US, the Food and Drug Administration approved the use of methylphenidate in 2008 for use in treating adult ADHD.[152] In the UK, while not licensed for use in Adult ADHD, NICE guidelines suggest it be prescribed off-license for the condition.[153] Methylphenidate has been approved for adult use in the treatment of narcolepsy.[154] One of the highest use of Methylphenidate medication is in Iceland and research shows that the drug was the most commonly abused substance among intravenous substance abusers in Iceland.[155] The study involved 108 IV substance abusers and 88% of them had injected methylphenidate within the last 30 days and for 63% of them, methylfenidate was the most preferred substance.
See also
- 3,4-Dichloromethylphenidate
- 4-Methylmethylphenidate
- Dexmethylphenidate
- Ethylphenidate
- HDMP-28
- Isopropylphenidate
- Propylphenidate
- Pethidine
Notes
- ↑ This involves impaired dopamine neurotransmission in the mesocortical and mesolimbic pathways and norepinephrine neurotransmission in the prefrontal cortex and locus coeruleus.[30]
References
- 1 2 3 Kimko, HC; Cross, JT; Abernethy, DR (December 1999). "Pharmacokinetics and clinical effectiveness of methylphenidate.". Clinical pharmacokinetics. 37 (6): 457–70. doi:10.2165/00003088-199937060-00002. PMID 10628897.
- 1 2 "Chemical and Physical Properties". Methylphenidate. Pubchem Compound. National Center for Biotechnology Information. Retrieved 24 June 2014.
- ↑ Markowitz JS, Straughn AB, Patrick KS (2003). "Advances in the pharmacotherapy of attention-deficit-hyperactivity disorder: focus on methylphenidate formulations". Pharmacotherapy. 23 (10): 1281–99. doi:10.1592/phco.23.12.1281.32697. PMID 14594346.
- ↑ Diller, Lawrence (1999). Running on Ritalin. ISBN 978-0553379068.
- ↑ Lange KW, Reichl S, Lange KM, Tucha L, Tucha O (2010). "The history of attention deficit hyperactivity disorder". ADHD Attention Deficit and Hyperactivity Disorders. 2 (4): 241–55. doi:10.1007/s12402-010-0045-8. PMC 3000907
 . PMID 21258430.
. PMID 21258430. - ↑ http://www.bbc.com/news/health-23674235
- ↑ http://www.pharmaceutical-journal.com/news-and-analysis/news-in-brief/narcotics-monitoring-board-reports-66-increase-in-global-consumption-of-methylphenidate/20068042.article
- ↑ "Functional Roles of Norepinephrine and Dopamine in ADHD: Dopamine in ADHD". Medscape. 2006. Retrieved 8 October 2013.
Catecholamines not only facilitate attention, they are essential to executive function. The prefrontal cortex directs behaviors, thoughts, and feelings represented in working memory. This representational knowledge is essential to fundamental cognitive abilities that compromise executive functions. These encompass the ability to (1) inhibit inappropriate behaviors and thoughts, (2) regulate our attention, (3) monitor our actions, and (4) plan and organize for the future. Difficulties with these prefrontal cortex functions are evident in neuropsychological and imaging studies of ADHD patients and account for many of the common behavioral symptoms. Measures of prefrontal cortical functioning in animals indicate that these functions are sensitive to small changes in catecholamine modulation of prefrontal cortex cells that can produce profound effects on the ability of the prefrontal cortex to guide behavior. Optimal levels of NE acting at postsynaptic alpha2A-adrenoceptors and dopamine acting at D1 receptors are essential to prefrontal cortex function. Blockade of norepinephrine alpha2-adrenoceptors in prefrontal cortex markedly impairs prefrontal cortex function and mimics most of the symptoms of ADHD, including impulsivity and locomotor hyperactivity. Conversely, stimulation of prefrontal cortical alpha2-adrenoceptors strengthens prefrontal cortex regulation of behavior and reduces distractibility. Thus, effective treatments for ADHD facilitate catecholamine transmission and apparently have their therapeutic actions by optimizing catecholamine actions in the prefrontal cortex
- ↑ Arnsten AF, Li BM (2005). "Neurobiology of Executive Functions: Catecholamine Influences on Prefrontal Cortical Functions". Biological Psychiatry. 57 (11): 1377–84. doi:10.1016/j.biopsych.2004.08.019. PMID 15950011.
- ↑ Stahl, Stephen M. Stahl's Essential Psychopharmacology: Neuroscientific Basis and Practical Applications (4th ed.). Cambridge University Press. ISBN 978-1107686465.
- ↑ "The psychostimulant d-threo-(R,R)-methylphenidate binds as an agonist to the 5HT(1A) receptor.". Pharmazie. 64: 123–5. Feb 2009. PMID 19322953.
- 1 2 Markowitz JS, Logan BK, Diamond F, Patrick KS (1999). "Detection of the novel metabolite ethylphenidate after methylphenidate overdose with alcohol coingestion". Journal of Clinical Psychopharmacology. 19 (4): 362–6. doi:10.1097/00004714-199908000-00013. PMID 10440465.
- ↑ Steele M, Weiss M, Swanson J, Wang J, Prinzo RS, Binder CE (2006). "A randomized, controlled effectiveness trial of OROS-methylphenidate compared to usual care with immediate-release methylphenidate in attention deficit-hyperactivity disorder" (PDF). Can J Clin Pharmacol. 13 (1): e50–62. PMID 16456216.
- ↑ Gilmore A, Milne R (2001). "Methylphenidate in children with hyperactivity: review and cost-utility analysis". Pharmacoepidemiol Drug Saf. 10 (2): 85–94. doi:10.1002/pds.564. PMID 11499858.
- ↑ Mott TF, Leach L, Johnson L (2004). "Clinical inquiries. Is methylphenidate useful for treating adolescents with ADHD?". The Journal of Family Practice. 53 (8): 659–61. PMID 15298843.
- ↑ Vitiello B (2001). "Psychopharmacology for young children: clinical needs and research opportunities". Pediatrics. 108 (4): 983–9. doi:10.1542/peds.108.4.983. PMID 11581454.
- ↑ Hermens DF, Rowe DL, Gordon E, Williams LM (2006). "Integrative neuroscience approach to predict ADHD stimulant response". Expert Review of Neurotherapeutics. 6 (5): 753–63. doi:10.1586/14737175.6.5.753. PMID 16734523.
- ↑ Bernardo Dell’Osso, Cristina Dobrea, Laura Cremaschi, Chiara Arici, A. Carlo Altamura (2014). "Wake-Promoting Pharmacotherapy for Psychiatric Disorders". Current Psychiatry Reports. 16 (12): 524. doi:10.1007/s11920-014-0524-2. PMID 25312027.
- ↑ Hart H, Radua J, Nakao T, Mataix-Cols D, Rubia K (February 2013). "Meta-analysis of functional magnetic resonance imaging studies of inhibition and attention in attention-deficit/hyperactivity disorder: exploring task-specific, stimulant medication, and age effects". JAMA Psychiatry. 70 (2): 185–198. doi:10.1001/jamapsychiatry.2013.277. PMID 23247506.
- ↑ Spencer TJ, Brown A, Seidman LJ, Valera EM, Makris N, Lomedico A, Faraone SV, Biederman J (September 2013). "Effect of psychostimulants on brain structure and function in ADHD: a qualitative literature review of magnetic resonance imaging-based neuroimaging studies". J. Clin. Psychiatry. 74 (9): 902–917. doi:10.4088/JCP.12r08287. PMC 3801446. PMID 24107764.
- ↑ Frodl T, Skokauskas N (February 2012). "Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects.". Acta psychiatrica Scand. 125 (2): 114–126. doi:10.1111/j.1600-0447.2011.01786.x. PMID 22118249.
Basal ganglia regions like the right globus pallidus, the right putamen, and the nucleus caudatus are structurally affected in children with ADHD. These changes and alterations in limbic regions like ACC and amygdala are more pronounced in non-treated populations and seem to diminish over time from child to adulthood. Treatment seems to have positive effects on brain structure.
- 1 2 3 Millichap, JG (2010). "Chapter 3: Medications for ADHD". In Millichap, JG. Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD (2nd ed.). New York: Springer. pp. 111–113. ISBN 9781441913968.
- 1 2 Huang YS, Tsai MH (July 2011). "Long-term outcomes with medications for attention-deficit hyperactivity disorder: current status of knowledge". CNS Drugs. 25 (7): 539–554. doi:10.2165/11589380-000000000-00000. PMID 21699268.
- ↑ Millichap, JG (2010). "Chapter 3: Medications for ADHD". In Millichap, JG. Attention Deficit Hyperactivity Disorder Handbook: A Physician's Guide to ADHD (2nd ed.). New York: Springer. pp. 121–123. ISBN 9781441913968.
- ↑ Storebø OJ, Ramstad E, Krogh HB, Nilausen TD, Skoog M, Holmskov M, Rosendal S, Groth C, Magnusson FL, Moreira-Maia CR, Gillies D, Buch Rasmussen K, Gauci D, Zwi M, Kirubakaran R, Forsbøl B, Simonsen E, Gluud C (November 2015). "Methylphenidate for children and adolescents with attention deficit hyperactivity disorder (ADHD)". Cochrane Database Syst Rev. 11: CD009885. doi:10.1002/14651858.CD009885.pub2. PMID 26599576.
- ↑ Fone KC, Nutt DJ (2005). "Stimulants: use and abuse in the treatment of ADD". Current Opinion in Pharmacology. 5 (1): 87–93. doi:10.1016/j.coph.2004.10.001. PMID 15661631.
- ↑ Capp PK, Pearl PL, Conlon C (2005). "Methylphenidate HCl: therapy for attention deficit hyperactivity disorder". Expert Rev Neurother. 5 (3): 325–31. doi:10.1586/14737175.5.3.325. PMID 15938665.
- ↑ Greenfield B, Hechman L (2005). "Treatment of attention deficit hyperactivity disorder in adults". Expert Rev Neurother. 5 (1): 107–21. doi:10.1586/14737175.5.1.107. PMID 15853481.
- ↑ Stevenson RD, Wolraich ML (1989). "Stimulant medication therapy in the treatment of children with attention deficit hyperactivity disorder". Pediatr. Clin. North Am. 36 (5): 1183–97. PMID 2677938.
- 1 2 3 Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 6: Widely Projecting Systems: Monoamines, Acetylcholine, and Orexin". In Sydor A, Brown RY. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. pp. 154–157. ISBN 9780071481274.
- 1 2 3 "Stimulants for Attention Deficit Hyperactivity Disorder". WebMD. Healthwise. 12 April 2010. Retrieved 12 November 2013.
- ↑ Greenhill LL, Pliszka S, Dulcan MK, Bernet W, Arnold V, Beitchman J, Benson RS, Bukstein O, Kinlan J, McClellan J, Rue D, Shaw JA, Stock S (February 2002). "Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults". J. Am. Acad. Child Adolesc. Psychiatry. 41 (2 Suppl): 26S–49S. doi:10.1097/00004583-200202001-00003. PMID 11833633.
- ↑ Faraone SV, Wilens TE (2007). "Effect of stimulant medications for attention-deficit/hyperactivity disorder on later substance use and the potential for stimulant misuse, abuse, and diversion". J Clin Psychiatry. 68 Suppl 11: 15–22. doi:10.4088/jcp.1107e28. PMID 18307377.
- ↑ Wilens TE, Faraone SV, Biederman J, Gunawardene S (2003). "Does Stimulant Therapy of Attention-Deficit/Hyperactivity Disorder Beget Later Substance Abuse? A Meta-analytic Review of the Literature". Pediatrics. 111 (1): 179–85. doi:10.1542/peds.111.1.179. PMID 12509574.
- ↑ Fry JM (1998). "Treatment modalities for narcolepsy". Neurology. 50 (2 Suppl 1): S43–8. doi:10.1212/WNL.50.2_Suppl_1.S43. PMID 9484423.
- ↑ Mitler MM (1994). "Evaluation of treatment with stimulants in narcolepsy". Sleep. 17 (8 Suppl): S103–6. PMID 7701190.
- ↑ Leonard BE, McCartan D, White J, King DJ (2004). "Methylphenidate: a review of its neuropharmacological, neuropsychological and adverse clinical effects". Hum Psychopharmacol. 19 (3): 151–80. doi:10.1002/hup.579. PMID 15079851.
- ↑ Kraus MF, Burch EA (1992). "Methylphenidate hydrochloride as an antidepressant: controversy, case studies, and review". South. Med. J. 85 (10): 985–91. doi:10.1097/00007611-199210000-00012. PMID 1411740.
- ↑ Satel SL, Nelson JC (1989). "Stimulants in the treatment of depression: a critical overview". J Clin Psychiatry. 50 (7): 241–9. PMID 2567730.
- ↑ Rozans M, Dreisbach A, Lertora JJ, Kahn MJ (2002). "Palliative uses of methylphenidate in patients with cancer: a review". J. Clin. Oncol. 20 (1): 335–9. doi:10.1200/JCO.20.1.335. PMID 11773187.
- 1 2 Spencer RC, Devilbiss DM, Berridge CW (June 2015). "The Cognition-Enhancing Effects of Psychostimulants Involve Direct Action in the Prefrontal Cortex". Biol. Psychiatry. 77 (11): 940–950. doi:10.1016/j.biopsych.2014.09.013. PMID 25499957.
The procognitive actions of psychostimulants are only associated with low doses. Surprisingly, despite nearly 80 years of clinical use, the neurobiology of the procognitive actions of psychostimulants has only recently been systematically investigated. Findings from this research unambiguously demonstrate that the cognition-enhancing effects of psychostimulants involve the preferential elevation of catecholamines in the PFC and the subsequent activation of norepinephrine α2 and dopamine D1 receptors. ... This differential modulation of PFC-dependent processes across dose appears to be associated with the differential involvement of noradrenergic α2 versus α1 receptors. Collectively, this evidence indicates that at low, clinically relevant doses, psychostimulants are devoid of the behavioral and neurochemical actions that define this class of drugs and instead act largely as cognitive enhancers (improving PFC-dependent function). This information has potentially important clinical implications as well as relevance for public health policy regarding the widespread clinical use of psychostimulants and for the development of novel pharmacologic treatments for attention-deficit/hyperactivity disorder and other conditions associated with PFC dysregulation.
- ↑ Ilieva IP, Hook CJ, Farah MJ (January 2015). "Prescription Stimulants' Effects on Healthy Inhibitory Control, Working Memory, and Episodic Memory: A Meta-analysis". J. Cogn. Neurosci.: 1–21. doi:10.1162/jocn_a_00776. PMID 25591060.
Specifically, in a set of experiments limited to high-quality designs, we found significant enhancement of several cognitive abilities. ... The results of this meta-analysis ... do confirm the reality of cognitive enhancing effects for normal healthy adults in general, while also indicating that these effects are modest in size.
- 1 2 3 Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 13: Higher Cognitive Function and Behavioral Control". In Sydor A, Brown RY. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 318. ISBN 9780071481274.
Therapeutic (relatively low) doses of psychostimulants, such as methylphenidate and amphetamine, improve performance on working memory tasks both in normal subjects and those with ADHD. Positron emission tomography (PET) demonstrates that methylphenidate decreases regional cerebral blood flow in the doroslateral prefrontal cortex and posterior parietal cortex while improving performance of a spatial working memory task. This suggests that cortical networks that normally process spatial working memory become more efficient in response to the drug. ... [It] is now believed that dopamine and norepinephrine, but not serotonin, produce the beneficial effects of stimulants on working memory. At abused (relatively high) doses, stimulants can interfere with working memory and cognitive control ... stimulants act not only on working memory function, but also on general levels of arousal and, within the nucleus accumbens, improve the saliency of tasks. Thus, stimulants improve performance on effortful but tedious tasks ... through indirect stimulation of dopamine and norepinephrine receptors.
- 1 2 3 Wood S, Sage JR, Shuman T, Anagnostaras SG (January 2014). "Psychostimulants and cognition: a continuum of behavioral and cognitive activation". Pharmacol. Rev. 66 (1): 193–221. doi:10.1124/pr.112.007054. PMID 24344115.
- ↑ Twohey M (26 March 2006). "Pills become an addictive study aid". JS Online. Archived from the original on 15 August 2007. Retrieved 2 December 2007.
- ↑ Teter CJ, McCabe SE, LaGrange K, Cranford JA, Boyd CJ (October 2006). "Illicit use of specific prescription stimulants among college students: prevalence, motives, and routes of administration". Pharmacotherapy. 26 (10): 1501–1510. doi:10.1592/phco.26.10.1501. PMC 1794223. PMID 16999660.
- ↑ Roelands B, de Koning J, Foster C, Hettinga F, Meeusen R (May 2013). "Neurophysiological determinants of theoretical concepts and mechanisms involved in pacing". Sports Med. 43 (5): 301–311. doi:10.1007/s40279-013-0030-4. PMID 23456493.
- 1 2 3 Noven Pharmaceuticals, Inc. (17 April 2015). "Daytrana Prescribing Information" (PDF). United States Food and Drug Administration. pp. 1–33. Retrieved 23 June 2015.
- ↑ Harris J (2009). "Is it acceptable for people to take methylphenidate to enhance performance? Yes". BMJ. 338: b1955. doi:10.1136/bmj.b1955. PMID 19541705.
- ↑ Davies, Caroline (21 February 2010). "Universities told to consider dope tests as student use of 'smart drugs' soars". The Observer. London. Retrieved 21 February 2010.
- ↑ "DAYTRANA" (PDF). United States Food and Drug Administration. Noven Pharmaceuticals, Inc. October 2013. Retrieved 13 June 2014.
- ↑ Methylphenidate Use During Pregnancy and Breastfeeding. Drugs.com. Retrieved on 30 April 2011.
- ↑ Humphreys C, Garcia-Bournissen F, Ito S, Koren G (2007). "Exposure to attention deficit hyperactivity disorder medications during pregnancy". Canadian Family Physician. 53 (7): 1153–5. PMC 1949295. PMID 17872810.
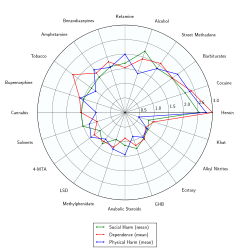
- ↑ Nutt, D; King, LA; Saulsbury, W; Blakemore, C (24 March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse.". Lancet (London, England). 369 (9566): 1047–53. doi:10.1016/S0140-6736(07)60464-4. PMID 17382831.
- ↑ Didoni, A; Sequi, M; Panei, P; Bonati, M; Lombardy ADHD Registry, Group (October 2011). "One-year prospective follow-up of pharmacological treatment in children with attention-deficit/hyperactivity disorder.". European journal of clinical pharmacology. 67 (10): 1061–7. doi:10.1007/s00228-011-1050-3. PMID 21538145.
• "Ritalin Side Effects". Retrieved 22 June 2015.
• "Biphentin product monograph" (PDF). Purdue Pharma. Retrieved 22 June 2015.
• Huss, M; Ginsberg, Y; Tvedten, T; Arngrim, T; Philipsen, A; Carter, K; Chen, CW; Kumar, V (January 2014). "Methylphenidate hydrochloride modified-release in adults with attention deficit hyperactivity disorder: a randomized double-blind placebo-controlled trial.". Advances in therapy. 31 (1): 44–65. doi:10.1007/s12325-013-0085-5. PMID 24371021. - 1 2 "Concerta product monograph" (PDF). Janssen Pharmaceuticals. Retrieved 4 December 2016.
- ↑ Jaanus SD (1992). "Ocular side-effects of selected systemic drugs". Optom Clin. 2 (4): 73–96. PMID 1363080.
- ↑ Stein; et al. (1998). "Sleep disturbances in children with Attention-Deficit/Hyperactivity Disorder a comparative study with healthy siblings". Journal of Learning Disabilities. 31 (6): 572–578.
- 1 2 Cortese, S; Holtmann, M; Banaschewski, T; Buitelaar, J; Coghill, D; Danckaerts, M; Dittmann, RW; Graham, J; Taylor, E; Sergeant, J; European ADHD Guidelines, Group (March 2013). "Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents.". Journal of child psychology and psychiatry, and allied disciplines. 54 (3): 227–46. doi:10.1111/jcpp.12036. PMID 23294014.
- ↑ Findling, RL; Dinh, S (March 2014). "Transdermal therapy for attention-deficit hyperactivity disorder with the methylphenidate patch (MTS).". CNS Drugs. 28 (3): 217–28. doi:10.1007/s40263-014-0141-y. PMID 24532028.
- ↑ Kraemer M, Uekermann J, Wiltfang J, Kis B (July 2010). "Methylphenidate-induced psychosis in adult attention-deficit/hyperactivity disorder: report of 3 new cases and review of the literature". Clin Neuropharmacol. 33 (4): 204–6. doi:10.1097/WNF.0b013e3181e29174. PMID 20571380.
- ↑ Wingo, AP; Ghaemi, SN (2008). "Frequency of stimulant treatment and of stimulant-associated mania/hypomania in bipolar disorder patients.". Psychopharmacology bulletin. 41 (4): 37–47. PMID 19015628.
- ↑ "Methylphenidate ADHD Medications: Drug Safety Communication – Risk of Long-lasting Erections". U.S. Food and Drug Administration. 17 December 2013. Retrieved 17 December 2013.
- ↑ "FDA Drug Safety Communication: Safety Review Update of Medications used to treat Attention-Deficit/Hyperactivity Disorder (ADHD) in children and young adults". United States Food and Drug Administration. 20 December 2011. Retrieved 4 November 2013.
• Cooper WO, Habel LA, Sox CM, Chan KA, Arbogast PG, Cheetham TC, Murray KT, Quinn VP, Stein CM, Callahan ST, Fireman BH, Fish FA, Kirshner HS, O'Duffy A, Connell FA, Ray WA (November 2011). "ADHD drugs and serious cardiovascular events in children and young adults". N. Engl. J. Med. 365 (20): 1896–1904. doi:10.1056/NEJMoa1110212. PMID 22043968.
• "FDA Drug Safety Communication: Safety Review Update of Medications used to treat Attention-Deficit/Hyperactivity Disorder (ADHD) in adults". United States Food and Drug Administration. 15 December 2011. Retrieved 4 November 2013.
• Habel LA, Cooper WO, Sox CM, Chan KA, Fireman BH, Arbogast PG, Cheetham TC, Quinn VP, Dublin S, Boudreau DM, Andrade SE, Pawloski PA, Raebel MA, Smith DH, Achacoso N, Uratsu C, Go AS, Sidney S, Nguyen-Huynh MN, Ray WA, Selby JV (December 2011). "ADHD medications and risk of serious cardiovascular events in young and middle-aged adults". JAMA. 306 (24): 2673–2683. doi:10.1001/jama.2011.1830. PMC 3350308. PMID 22161946. - ↑ Gordon N (1999). "Attention deficit hyperactivity disorder: possible causes and treatment". Int. J. Clin. Pract. 53 (7): 524–8. PMID 10692738.
- 1 2 Heedes G, Ailakis J. "Methylphenidate hydrochloride (PIM 344)". INCHEM. International Programme on Chemical Safety. Retrieved 23 June 2015.
- 1 2 3 Spiller HA, Hays HL, Aleguas A (June 2013). "Overdose of drugs for attention-deficit hyperactivity disorder: clinical presentation, mechanisms of toxicity, and management". CNS Drugs. 27 (7): 531–543. doi:10.1007/s40263-013-0084-8. PMID 23757186.
The management of amphetamine, dextroamphetamine, and methylphenidate overdose is largely supportive, with a focus on interruption of the sympathomimetic syndrome with judicious use of benzodiazepines. In cases where agitation, delirium, and movement disorders are unresponsive to benzodiazepines, second-line therapies include antipsychotics such as ziprasidone or haloperidol, central alpha-adrenoreceptor agonists such as dexmedetomidine, or propofol. ... However, fatalities are rare with appropriate care
- ↑ Bruggisser M, Bodmer M, Liechti ME (2011). "Severe toxicity due to injected but not oral or nasal abuse of methylphenidate tablets". Swiss Med Wkly. 141: w13267. doi:10.4414/smw.2011.13267. PMID 21984207.
- ↑ Nestler EJ, Barrot M, Self DW (September 2001). "DeltaFosB: a sustained molecular switch for addiction". Proc. Natl. Acad. Sci. U.S.A. 98 (20): 11042–11046. doi:10.1073/pnas.191352698. PMC 58680. PMID 11572966.
Although the ΔFosB signal is relatively long-lived, it is not permanent. ΔFosB degrades gradually and can no longer be detected in brain after 1–2 months of drug withdrawal ... Indeed, ΔFosB is the longest-lived adaptation known to occur in adult brain, not only in response to drugs of abuse, but to any other perturbation (that doesn't involve lesions) as well.
- ↑ Nestler EJ (December 2012). "Transcriptional mechanisms of drug addiction". Clin. Psychopharmacol. Neurosci. 10 (3): 136–143. doi:10.9758/cpn.2012.10.3.136. PMC 3569166. PMID 23430970.
The 35–37 kD ΔFosB isoforms accumulate with chronic drug exposure due to their extraordinarily long half-lives. ... As a result of its stability, the ΔFosB protein persists in neurons for at least several weeks after cessation of drug exposure. ... ΔFosB overexpression in nucleus accumbens induces NFκB
- ↑ Morton WA, Stockton GG (2000). "Methylphenidate Abuse and Psychiatric Side Effects". Prim Care Companion J Clin Psychiatry. 2 (5): 159–164. doi:10.4088/PCC.v02n0502. PMC 181133. PMID 15014637.
- 1 2 3 4 5 Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY. Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 368. ISBN 9780071481274.
Cocaine, [amphetamine], and methamphetamine are the major psychostimulants of abuse. The related drug methylphenidate is also abused, although it is far less potent. These drugs elicit similar initial subjective effects ; differences generally reflect the route of administration and other pharmacokinetic factors. Such agents also have important therapeutic uses; cocaine, for example, is used as a local anesthetic (Chapter 2), and amphetamines and methylphenidate are used in low doses to treat attention deficit hyperactivity disorder and in higher doses to treat narcolepsy (Chapter 12). Despite their clinical uses, these drugs are strongly reinforcing, and their long-term use at high doses is linked with potential addiction, especially when they are rapidly administered or when high-potency forms are given.
- 1 2 Steiner H, Van Waes V (January 2013). "Addiction-related gene regulation: risks of exposure to cognitive enhancers vs. other psychostimulants". Prog. Neurobiol. 100: 60–80. doi:10.1016/j.pneurobio.2012.10.001. PMC 3525776. PMID 23085425.
- ↑ Auger RR, Goodman SH, Silber MH, Krahn LE, Pankratz VS, Slocumb NL (2005). "Risks of high-dose stimulants in the treatment of disorders of excessive somnolence: a case-control study". Sleep. 28 (6): 667–72. PMID 16477952.
- 1 2 3 4 5 6 Kim Y, Teylan MA, Baron M, Sands A, Nairn AC, Greengard P (2009). "Methylphenidate-induced dendritic spine formation and DeltaFosB expression in nucleus accumbens". Proc. Natl. Acad. Sci. U.S.A. 106 (8): 2915–20. doi:10.1073/pnas.0813179106. PMC 2650365. PMID 19202072.
Despite decades of clinical use of methylphenidate for ADHD, concerns have been raised that long-term treatment of children with this medication may result in subsequent drug abuse and addiction. However, meta analysis of available data suggests that treatment of ADHD with stimulant drugs may have a significant protective effect, reducing the risk for addictive substance use (36, 37). Studies with juvenile rats have also indicated that repeated exposure to methylphenidate does not necessarily lead to enhanced drug-seeking behavior in adulthood (38). However, the recent increase of methylphenidate use as a cognitive enhancer by the general public has again raised concerns because of its potential for abuse and addiction (3, 6–10). Thus, although oral administration of clinical doses of methylphenidate is not associated with euphoria or with abuse problems, nontherapeutic use of high doses or i.v. administration may lead to addiction (39, 40).
- ↑ Elkashef A, Vocci F, Hanson G, White J, Wickes W, Tiihonen J (2008). "Pharmacotherapy of methamphetamine addiction: an update". Substance Abuse. 29 (3): 31–49. doi:10.1080/08897070802218554. PMC 2597382. PMID 19042205.
- ↑ Grabowski J, Roache JD, Schmitz JM, Rhoades H, Creson D, Korszun A (1997). "Replacement medication for cocaine dependence: methylphenidate". J Clin Psychopharmacol. 17 (6): 485–8. doi:10.1097/00004714-199712000-00008. PMID 9408812.
- ↑ Gorelick DA, Gardner EL, Xi ZX (2004). "Agents in development for the management of cocaine abuse". Drugs. 64 (14): 1547–73. doi:10.2165/00003495-200464140-00004. PMID 15233592.
- ↑ Karila L, Gorelick D, Weinstein A, Noble F, Benyamina A, Coscas S, Blecha L, Lowenstein W, Martinot JL, Reynaud M, Lépine JP (2008). "New treatments for cocaine dependence: a focused review". Int. J. Neuropsychopharmacol. 11 (3): 425–38. doi:10.1017/S1461145707008097. PMID 17927843.
- ↑ "NIDA InfoFacts: Understanding Drug Abuse and Addiction" (PDF). 2008.
- ↑ Shearer J (2008). "The principles of agonist pharmacotherapy for psychostimulant dependence". Drug Alcohol Rev. 27 (3): 301–8. doi:10.1080/09595230801927372. PMID 18368612.
- 1 2 3 Nestler EJ (December 2013). "Cellular basis of memory for addiction". Dialogues Clin. Neurosci. 15 (4): 431–443. PMC 3898681. PMID 24459410.
DESPITE THE IMPORTANCE OF NUMEROUS PSYCHOSOCIAL FACTORS, AT ITS CORE, DRUG ADDICTION INVOLVES A BIOLOGICAL PROCESS: the ability of repeated exposure to a drug of abuse to induce changes in a vulnerable brain that drive the compulsive seeking and taking of drugs, and loss of control over drug use, that define a state of addiction. ... A large body of literature has demonstrated that such ΔFosB induction in D1-type NAc neurons increases an animal's sensitivity to drug as well as natural rewards and promotes drug self-administration, presumably through a process of positive reinforcement ... Another ΔFosB target is cFos: as ΔFosB accumulates with repeated drug exposure it represses c-Fos and contributes to the molecular switch whereby ΔFosB is selectively induced in the chronic drug-treated state.41. ... Moreover, there is increasing evidence that, despite a range of genetic risks for addiction across the population, exposure to sufficiently high doses of a drug for long periods of time can transform someone who has relatively lower genetic loading into an addict.4
- ↑ Ruffle JK (November 2014). "Molecular neurobiology of addiction: what's all the (Δ)FosB about?". Am J Drug Alcohol Abuse. 40 (6): 428–437. doi:10.3109/00952990.2014.933840. PMID 25083822.
The strong correlation between chronic drug exposure and ΔFosB provides novel opportunities for targeted therapies in addiction (118), and suggests methods to analyze their efficacy (119). Over the past two decades, research has progressed from identifying ΔFosB induction to investigating its subsequent action (38). It is likely that ΔFosB research will now progress into a new era – the use of ΔFosB as a biomarker. ...
Conclusions
ΔFosB is an essential transcription factor implicated in the molecular and behavioral pathways of addiction following repeated drug exposure. The formation of ΔFosB in multiple brain regions, and the molecular pathway leading to the formation of AP-1 complexes is well understood. The establishment of a functional purpose for ΔFosB has allowed further determination as to some of the key aspects of its molecular cascades, involving effectors such as GluR2 (87,88), Cdk5 (93) and NFkB (100). Moreover, many of these molecular changes identified are now directly linked to the structural, physiological and behavioral changes observed following chronic drug exposure (60,95,97,102). New frontiers of research investigating the molecular roles of ΔFosB have been opened by epigenetic studies, and recent advances have illustrated the role of ΔFosB acting on DNA and histones, truly as a ‘‘molecular switch’’ (34). As a consequence of our improved understanding of ΔFosB in addiction, it is possible to evaluate the addictive potential of current medications (119), as well as use it as a biomarker for assessing the efficacy of therapeutic interventions (121,122,124). Some of these proposed interventions have limitations (125) or are in their infancy (75). However, it is hoped that some of these preliminary findings may lead to innovative treatments, which are much needed in addiction. - ↑ Biliński P, Wojtyła A, Kapka-Skrzypczak L, Chwedorowicz R, Cyranka M, Studziński T (2012). "Epigenetic regulation in drug addiction". Ann. Agric. Environ. Med. 19 (3): 491–496. PMID 23020045.
For these reasons, ΔFosB is considered a primary and causative transcription factor in creating new neural connections in the reward centre, prefrontal cortex, and other regions of the limbic system. This is reflected in the increased, stable and long-lasting level of sensitivity to cocaine and other drugs, and tendency to relapse even after long periods of abstinence. These newly constructed networks function very efficiently via new pathways as soon as drugs of abuse are further taken ... In this way, the induction of CDK5 gene expression occurs together with suppression of the G9A gene coding for dimethyltransferase acting on the histone H3. A feedback mechanism can be observed in the regulation of these 2 crucial factors that determine the adaptive epigenetic response to cocaine. This depends on ΔFosB inhibiting G9a gene expression, i.e. H3K9me2 synthesis which in turn inhibits transcription factors for ΔFosB. For this reason, the observed hyper-expression of G9a, which ensures high levels of the dimethylated form of histone H3, eliminates the neuronal structural and plasticity effects caused by cocaine by means of this feedback which blocks ΔFosB transcription
- ↑ Robison AJ, Nestler EJ (November 2011). "Transcriptional and epigenetic mechanisms of addiction". Nat. Rev. Neurosci. 12 (11): 623–637. doi:10.1038/nrn3111. PMC 3272277. PMID 21989194.
ΔFosB has been linked directly to several addiction-related behaviors ... Importantly, genetic or viral overexpression of ΔJunD, a dominant negative mutant of JunD which antagonizes ΔFosB- and other AP-1-mediated transcriptional activity, in the NAc or OFC blocks these key effects of drug exposure14,22–24. This indicates that ΔFosB is both necessary and sufficient for many of the changes wrought in the brain by chronic drug exposure. ΔFosB is also induced in D1-type NAc MSNs by chronic consumption of several natural rewards, including sucrose, high fat food, sex, wheel running, where it promotes that consumption14,26–30. This implicates ΔFosB in the regulation of natural rewards under normal conditions and perhaps during pathological addictive-like states.
- ↑ Ishii, M; Tatsuzawa, Y; Yoshino, A; Nomura, S (April 2008). "Serotonin syndrome induced by augmentation of SSRI with methylphenidate.". Psychiatry and clinical neurosciences. 62 (2): 246. doi:10.1111/j.1440-1819.2008.01767.x. PMID 18412855.
- ↑ Türkoğlu, S (2015). "Serotonin syndrome with sertraline and methylphenidate in an adolescent.". Clinical neuropharmacology. 38 (2): 65–6. doi:10.1097/WNF.0000000000000075. PMID 25768857.
- ↑ Park, YM; Jung, YK (30 May 2010). "Manic switch and serotonin syndrome induced by augmentation of paroxetine with methylphenidate in a patient with major depression.". Progress in neuro-psychopharmacology & biological psychiatry. 34 (4): 719–20. doi:10.1016/j.pnpbp.2010.03.016. PMID 20298736.
- ↑ Bodner, RA; Lynch, T; Lewis, L; Kahn, D (February 1995). "Serotonin syndrome.". Neurology. 45 (2): 219–23. doi:10.1212/wnl.45.2.219. PMID 7854515.
- ↑ Patrick KS, González MA, Straughn AB, Markowitz JS (2005). "New methylphenidate formulations for the treatment of attention-deficit/hyperactivity disorder". Expert Opinion on Drug Delivery. 2 (1): 121–43. doi:10.1517/17425247.2.1.121. PMID 16296740.
- ↑ Markowitz JS, DeVane CL, Boulton DW, Nahas Z, Risch SC, Diamond F, Patrick KS (2000). "Ethylphenidate formation in human subjects after the administration of a single dose of methylphenidate and ethanol". Drug Metabolism and Disposition. 28 (6): 620–4. PMID 10820132.
- ↑ Markowitz JS, DeVane CL, Boulton DW, Nahas Z, Risch SC, Diamond F, Patrick KS (2000). "Ethylphenidate formation in human subjects after the administration of a single dose of methylphenidate and ethanol". Drug metabolism and disposition: the biological fate of chemicals. 28 (6): 620–4. PMID 10820132.
- ↑ Patrick KS, Straughn AB, Minhinnett RR, Yeatts SD, Herrin AE, DeVane CL, Malcolm R, Janis GC, Markowitz JS (March 2007). "Influence of ethanol and gender on methylphenidate pharmacokinetics and pharmacodynamics.". Clinical pharmacology and therapeutics. 81 (3): 346–53. doi:10.1038/sj.clpt.6100082. PMC 3188424. PMID 17339864.
- ↑ Roberts SM, DeMott RP, James RC (1997). "Adrenergic modulation of hepatotoxicity". Drug Metab. Rev. 29 (1–2): 329–53. doi:10.3109/03602539709037587. PMID 9187524.
- ↑ Markowitz, JS; Patrick, KS (June 2008). "Differential pharmacokinetics and pharmacodynamics of methylphenidate enantiomers: does chirality matter?". Journal of Clinical Psychopharmacology. 28 (3 Suppl 2): S54–61. doi:10.1097/JCP.0b013e3181733560. PMID 18480678.
- ↑ Williard, RL; Middaugh, LD; Zhu, HJ; Patrick, KS (February 2007). "Methylphenidate and its ethanol transesterification metabolite ethylphenidate: brain disposition, monoamine transporters and motor activity.". Behavioural Pharmacology. 18 (1): 39–51. doi:10.1097/fbp.0b013e3280143226. PMID 17218796.
- 1 2 Markowitz, JS; DeVane, CL; Pestreich, LK; Patrick, KS; Muniz, R (December 2006). "A comprehensive in vitro screening of d-, l-, and dl-threo-methylphenidate: an exploratory study.". Journal of child and adolescent psychopharmacology. 16 (6): 687–98. doi:10.1089/cap.2006.16.687. PMID 17201613.
- 1 2 3 Heal DJ, Pierce DM (2006). "Methylphenidate and its isomers: their role in the treatment of attention-deficit hyperactivity disorder using a transdermal delivery system". CNS Drugs. 20 (9): 713–38. doi:10.2165/00023210-200620090-00002. PMID 16953648.
- ↑ Iversen L (2006). "Neurotransmitter transporters and their impact on the development of psychopharmacology". British Journal of Pharmacology. 147 (Suppl 1): S82–8. doi:10.1038/sj.bjp.0706428. PMC 1760736. PMID 16402124.
- ↑ Viggiano D, Vallone D, Sadile A (2004). "Dysfunctions in dopamine systems and ADHD: evidence from animals and modeling". Neural Plasticity. 11 (1–2): 102, 106–107. doi:10.1155/NP.2004.97. PMC 2565441. PMID 15303308.Full-text
- ↑ Novartis:Focalin XR Overview
- ↑ Focalin XR – Full Prescribing Information. Novartis.
- ↑ Concerta XL 18 mg – 36 mg prolonged release tablets last updated on the eMC: 5 November 2010
- ↑ Miller GM (January 2011). "The emerging role of trace amine-associated receptor 1 in the functional regulation of monoamine transporters and dopaminergic activity". J. Neurochem. 116 (2): 164–76. doi:10.1111/j.1471-4159.2010.07109.x. PMC 3005101. PMID 21073468.
- ↑ Markowitz, J. S., DeVane, C. L., Ramamoorthy, S., & Zhu, H. J. (2009). The psychostimulant d-threo-(R, R)-methylphenidate binds as an agonist to the 5HT1A receptor. Die Pharmazie-An International Journal of Pharmaceutical Sciences, 64(2), 123–125. http://www.ingentaconnect.com/content/govi/pharmaz/2009/00000064/00000002/art00012
- ↑ Volz TJ (2008). "Neuropharmacological Mechanisms Underlying the Neuroprotective Effects of Methylphenidate". Current Neuropharmacology. 6 (4): 379–385. doi:10.2174/157015908787386041. PMC 2701286. PMID 19587858.
- ↑ Zhang CL, Feng ZJ, Liu Y, Ji XH, Peng JY, Zhang XH, Zhen XC, Li BM (2012). "Methylphenidate enhances NMDA-receptor response in medial prefrontal cortex via sigma-1 receptor: a novel mechanism for methylphenidate action". PLoS ONE. 7 (12): e51910. doi:10.1371/journal.pone.0051910. PMC 3527396. PMID 23284812.
- ↑ Chan YP, Swanson JM, Soldin SS, Thiessen JJ, Macleod SM, Logan W (1983). "Methylphenidate hydrochloride given with or before breakfast: II. Effects on plasma concentration of methylphenidate and ritalinic acid". Pediatrics. 72 (1): 56–59. PMID 6866592.
- ↑ Sun, Z; Murry, DJ; Sanghani, SP; Davis, WI; Kedishvili, NY; Zou, Q; Hurley, TD; Bosron, WF (August 2004). "Methylphenidate is stereoselectively hydrolyzed by human carboxylesterase CES1A1". The Journal of Pharmacology and Experimental Therapeutics. 310 (2): 469–76. doi:10.1124/jpet.104.067116. PMID 15082749.
- ↑ Froimowitz M, Patrick KS, Cody V (1995). "Conformational analysis of methylphenidate and its structural relationship to other dopamine reuptake blockers such as CFT". Pharmaceutical Research. 12 (10): 1430–4. doi:10.1023/A:1016262815984. PMID 8584475.
- ↑ Prashad M (2001). "Approaches to the Preparation of Enantiomerically Pure (2R,2′R)-(+)-threo-Methylphenidate Hydrochloride" (PDF). Adv. Synth. Catal. 343 (5): 379–92. doi:10.1002/1615-4169(200107)343:5<379::AID-ADSC379>3.0.CO;2-4.
- ↑ Axten JM, Krim L, Kung HF, Winkler JD (1998). "A Stereoselective Synthesis ofdl-threo-Methylphenidate: Preparation and Biological Evaluation of Novel Analogues". The Journal of Organic Chemistry. 63 (26): 9628–9629. doi:10.1021/jo982214t.
- ↑ Singh S (2000). "Chemistry, Design, and Structure-Activity Relationship of Cocaine Antagonists" (PDF). Chem. Rev. 100 (3): 925–1024 (1008). doi:10.1021/cr9700538. PMID 11749256.
- ↑ R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 9th edition, Biomedical Publications, Seal Beach, CA, 2011, pp. 1091–93.
- ↑ "Education/Training » Clinical Resources". Illinois DocAssist website. University of Illinois at Chicago. Retrieved 26 July 2012.
Ritalin‑SR, methylphenidate SR, Methylin ER, and Metadate ER are the same formulation and have the same drug delivery system
- ↑ "Apo‑Methylphenidate SR product monograph" (PDF). Apotex Inc. 31 March 2005. "Comparative Bioavailability" section. Retrieved 26 July 2012. If the monograph link doesn't work, visit Health Canada's Drug Product Database query form one time, then click the monograph link again.
- ↑ "New product: Sandoz Methylphenidate SR 20 mg" (PDF). Sandoz Canada Inc. 5 May 2009. Retrieved 26 July 2012.
An alternative to Ritalin‑SR from Novartis
- ↑ "Drugs@FDA: FDA Approved Drug Products". Drugs@FDA: FDA Approved Drug Products. US Food and Drug Administration. Retrieved 1 October 2016.
- ↑ Hosenbocus, S; Chahal, R (November 2009). "A review of long-acting medications for ADHD in Canada.". Journal of the Canadian Academy of Child and Adolescent Psychiatry / Journal de l'Academie canadienne de psychiatrie de l'enfant et de l'adolescent. 18 (4): 331–9. PMC 2765387. PMID 19881943.
- ↑ (PDF) http://www.aptensioxr.com/resources/full-prescribing-information.pdf. Missing or empty
|title=(help) - 1 2 3 4 5 Moses, Scott (26 July 2009). "Methylphenidate". Family Practice Notebook. Retrieved 7 August 2012.
- ↑ "Daytrana transdermal". WebMD. Retrieved 11 June 2015.
- ↑ Concerta for Kids with ADHD. Pediatrics.about.com (1 April 2003). Retrieved on 30 April 2011.
- ↑ Concerta (Methylphenidate Extended-Release Tablets) Drug Information: User Reviews, Side Effects, Drug Interactions and Dosage at RxList. Rxlist.com. Retrieved on 30 April 2011.
- ↑ Ritalin LA® (methylphenidate hydrochloride) extended-release capsules, Novartis
- ↑ Metadate CD. Adhd.emedtv.com. Retrieved on 30 April 2011.
- ↑ Quillivant PI Sheet. Retrieved 13 October 2014.
- ↑ Based on: "Methylphenidate Hydrochloride". International Drug Price Indicator Guide. Retrieved 9 May 2016.
- ↑ The Ontario Drug Benefit online formulary indicates that, in Ontario, Canada, the local most-expensive methylphenidate product is probably Concerta. Drug prices in the US are often higher than in Canada. The GoodRx website correctly points out that short-term refills (e.g. 30 tablets) often cost more per tablet than longer-term refills (e.g. 90 tablets). For 30 tablets of brand-name Concerta 27 mg, the relevant GoodRx webpage offers coupons. However, if a patient ignores the coupons, and if the patient does not shop around, the website indicates that it is possible to pay more than twelve US dollars per defined daily dose. Data retrieved 17 May 2016.
- ↑ Panizzon L (1944). "La preparazione di piridile piperidil-arilacetonitrili e di alcuni prodotti di trasformazione (Parte Ia)". Helvetica Chimica Acta. 27: 1748–56. doi:10.1002/hlca.194402701222.
- ↑ Meier R, Gross F, Tripod J (1954). "Ritalin, a new synthetic compound with specific analeptic components". Klinische Wochenschrift. 32 (19–20): 445–50. doi:10.1007/BF01466968. PMID 13164273.
- 1 2 Myers, Richard L (August 2007). The 100 most important chemical compounds: a reference guide By Richard L. Myers. ISBN 978-0-313-33758-1. Retrieved 10 September 2010.
- ↑ Leandro Panizzon et al Pyridine and piperdjine compounds U.S. Patent 2,507,631 Issue date: 16 May 1950
- ↑ Rudolf Rouietscji et al Process for the conversion of U.S. Patent 2,838,519 Issue date: 10 June 1958
- ↑ Rudolf Rouietscji et alProcess for the conversion of U.S. Patent 2,957,880 Issue date: 25 October 1960
- ↑ Stolerman, Ian (2010). Encyclopedia of psychopharmacology. Berlin London: Springer. p. 763. ISBN 3540686983.
- ↑ Ritalin and Attention Deficit Disorder: History of its Use, Effects and Side Effects. Susan McCrossin, 1995; http://www.crossinology.com/pdf/RITALINus.pdf
- ↑ Bradley, Charles. Benzedrine® and Dexedrine® in the Treatment of Children's Behavior Disorders. Pediatrics 1950; 5:1 24–37
- ↑ Terrance Woodworth (16 May 2000). "DEA Congressional Testimony". Retrieved 2 November 2007.
- ↑ Approved Drug Therapies (637) Concerta, Alza. CenterWatch. Retrieved on 30 April 2011.
- ↑ "Green List: Annex to the annual statistical report on psychotropic substances (form P)" (PDF). (1.63 MB) 23rd edition. August 2003. International Narcotics Board, Vienna International Centre. Retrieved 2 March 2006.
- ↑ "Misuse of Drugs Act 1971 (c. 38): SCHEDULE 2: Controlled Drugs". Office of Public Sector Information. Retrieved 15 June 2009.
- ↑ "Poisons Standard 2012 as amended made under paragraph 52D(2)(a) of the Therapeutic Goods Act 1989.". Therapeutic Goods Administration. 27 November 2014. Retrieved 28 June 2015.
- ↑ "Narkotikastrafflag (1968:64)". Ministry of Justice. Retrieved 15 January 2014.
- ↑ Frances C, Hoizey G, Millart H, Trenque (2004). "Paediatric methylphenidate (Ritalin) restrictive conditions of prescription in France". British Journal of Clinical Pharmacology. 57 (1): 115–6. doi:10.1046/j.1365-2125.2003.01943.x. PMC 1884413. PMID 14678352.
- ↑ http://www.mohfw.nic.in/WriteReadData/l892s/43503435431421382269.pdf
- ↑ Lakhan SE, Hagger-Johnson GE (2007). "The impact of prescribed psychotropics on youth". Clin Pract Epidemol Ment Health. 3 (1): 21. doi:10.1186/1745-0179-3-21. PMC 2100041. PMID 17949504.
- ↑ New Research Helps Explain Ritalin's Low Abuse Potential When Taken As Prescribed – 09/29/1998. Nih.gov. Retrieved on 30 April 2011.
- ↑ Stimulant ADHD Medications: Methylphenidate and Amphetamines – InfoFacts – NIDA. Drugabuse.gov. Retrieved on 30 April 2011.
- ↑ Schoenfelder, EN; Faraone, SV; Kollins, SH (June 2014). "Stimulant treatment of ADHD and cigarette smoking: a meta-analysis.". Pediatrics. 133 (6): 1070–80. doi:10.1542/peds.2014-0179. PMID 24819571.
- ↑ Ouellette EM (1991). "Legal issues in the treatment of children with attention deficit hyperactivity disorder". Journal of Child Neurology. 6 Suppl: S68–75. doi:10.1177/0883073891006001081 (inactive 2016-10-01). PMID 2002217.
- ↑ FDA OKs Concerta for Adult ADHD, webmd.com
- ↑ NICE – Can methylphenidate be used for adults with attention deficit hyperactivity disorder (ADHD)? evidence.nhs.uk (4 July 2013). Retrieved on 5 December 2013.
- ↑ Ritalin for Adults. Adhd.emedtv.com (6 March 2007). Retrieved on 30 April 2011.
- ↑ Bjarnadottir, Gudrun D.; Haraldsson, Haraldur M.; Rafnar, Bjarni O.; Sigurdsson, Engilbert; Steingrimsson, Steinn; Johannsson, Magnus; Bragadottir, Helena; Magnusson, Andres (2016-11-29). "Prevalent Intravenous Abuse of Methylphenidate Among Treatment-Seeking Patients With Substance Abuse Disorders: A Descriptive Population-Based Study". Journal of Addiction Medicine. 9 (3): 188–194. doi:10.1097/ADM.0000000000000115. ISSN 1932-0620. PMC 4450903. PMID 25748561.
External links
| Wikimedia Commons has media related to Methylphenidate. |