Persistent Müllerian duct syndrome
| Persistent Müllerian duct syndrome | |
|---|---|
| Classification and external resources | |
| Specialty | medical genetics |
| ICD-10 | Q55.8 |
| OMIM | 261550 |
| DiseasesDB | 33868 |
| MeSH | C536665 |
Persistent Müllerian duct syndrome (PMDS) is the presence of Müllerian duct derivatives (fallopian tubes, uterus, and/or the upper part of the vagina)[1] in what would be considered a genetically male animal by typical human based standards. In humans, PMDS typically is due to an autosomal recessive[2] congenital disorder and is considered by some to be a form of pseudohermaphroditism due to the presence of Müllerian derivatives.[1][3]
Typical features include undescended testes (cryptorchidism) and the presence of a small, underdeveloped uterus in an XY infant or adult. This condition is usually caused by deficiency of fetal anti-Müllerian hormone (AMH) effect due to mutations of the gene for AMH or the anti-Müllerian hormone receptor, but may also be as a result of insensitivity to AMH of the target organ.[1]
Background
AMH (Anti Müllerian Hormone) is produced by the primitive Sertoli cells as one of the earliest Sertoli cell products and induces regression of the Müllerian ducts. Fetal Müllerian ducts are only sensitive to AMH action around the 7th or 8th week of gestation,[4] and Müllerian regression is completed by the end of the 9th week. The AMH induced regression of the Müllerian duct occurs in cranio-caudal direction via apoptosis. The AMH receptors are on the Müllerian duct mesenchyme and transfer the apoptotic signal to the Müllerian epithelial cell, presumably via paracrine actors. The Wolffian ducts differentiate into epididymides, vasa deferentia and seminal vesicles under the influence of testosterone, produced by the fetal Leydig cells[5]
Presentation
Because both the Wolffian ducts and Müllerian ducts begin to develop, the tissues are often intertwined, resulting in obstruction or nonpatency of the vas deferens or other parts of the reproductive excretory ducts. This can result in infertility, the most serious potential problem caused by this condition. Sometimes, transverse testicular ectopia is evident.[4]
Cryptorchidism in AMH deficiency suggests that AMH may play a role in transabdominal testicular descent, perhaps by facilitating contraction of the gubernaculum.
Other Müllerian derivatives which may be present in at least a rudimentary form are the cervix, upper part of the vagina, and fallopian tubes.[6]
The condition can come to attention because of a bulge in the inguinal canal of an XY infant due to herniation of the uterus. The presence of a uterus may be noticed if an ultrasound or MRI of the pelvis is performed to locate the testes or for other reasons. Occasionally the uterus is discovered during abdominal surgery for some other purpose in later childhood or adult life.
Although persistent Müllerian duct syndrome is classified as an intersex condition, it does not involve ambiguity or malformation of the external genitalia, which appear typical (apart from cryptorchidism if present). Sometimes the uterus enters a hernia.[1] Sometimes the Müllerian structures get entangled with the spermatic ducts and interfere with the descent of the testes.
Apart from humans, this syndrome has been reported in dogs.[7]
Treatment
Surgery (orchiopexy) to retrieve the testes and position them in the scrotum is the primary treatment. Occasionally they are unsalvageable if located high in the retroperitoneum. During this surgery, the uterus is usually removed and attempts made to dissect away Müllerian tissue from the vas deferens and epididymis to improve the chance of fertility. If the person has male gender identity himself and the testes cannot be retrieved, testosterone replacement will be usually necessary at puberty should the affected individual choose to pursue medical attention. Lately, laparoscopic hysterectomy is offered to patients as a solution to both improve the chances of fertility and to prevent the occurrences of neoplastic tissue formation.[3]
Molecular genetics and inheritance
PMDS type I results from mutations of the gene (AMH) for AMH on chromosome 19p3.3.[8]
PMDS type II results from mutations of the gene (AMH-RII) for the AMH receptor on 12q13.[9]
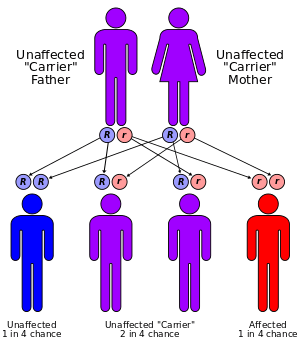
Both types of disorders are inherited as autosomal recessive conditions with expression usually limited to XY offspring.
References
- 1 2 3 4 Renu, Divya; Rao, GaneshB; Ranganath, K; Namitha (2010). "Persistent mullerian duct syndrome". Indian Journal of Radiology and Imaging. 20 (1): 72–4. doi:10.4103/0971-3026.59761. PMID 20352001.
- ↑ Imbeaud, S; Belville, C; Messika-Zeitoun, L; Rey, R; Di, Clemente, N; Josso, N; Picard, Jy (September 1996). "A 27 base-pair deletion of the anti-müllerian type II receptor gene is the most common cause of the persistent müllerian duct syndrome" (Free full text). Human Molecular Genetics. 5 (9): 1269–77. doi:10.1093/hmg/5.9.1269. PMID 8872466.
- 1 2 Colacurci, N.; A.Cardone; P.De Franciscis; E.Landolfi; T.Venditto; A.A.Sinisi (1997-12-02). "Laparoscopic hysterectomy in a case of male pseudohermaphroditism with persistent Müllerian duct derivatives" (PDF). European Society of Human Reproduction and Embryology. Oxford University Press. 12 (2): 272–274. doi:10.1093/humrep/12.2.272. ISSN 1460-2350. Retrieved 2009-05-17.
- 1 2 Shamim, Muhammad (August 2007). "Persistent Mullerian duct syndrome with transverse testicular ectopia presenting in an irreducible recurrent inguinal hernia.". The Journal of the Pakistan Medical Association. 57 (8): 421–3. PMID 17902529. Retrieved 9 February 2015.
- ↑ Rey, Rodolfo (2005-02-01). "Anti-Müllerian hormone in disorders of sex determination and differentiation". Arq. Bras. Endocrinol. Metabol. 49 (1): 26–36. doi:10.1590/s0004-27302005000100005. PMID 16544032.
- ↑ Grzegorz Kudela; Mirosław Mikosiński; Wojciech Utrata; Elżbieta Kuleta-Bosak; Barbara Kalina-Faska; Tomasz Koszutski (2008). "Persistent Müllerian Duct Syndrome – Familiar Occurrence". J. Urologia Polska. 61 (3). ISSN 0500-7208.
- ↑ Vegter AR, Kooistra HS, van Sluijs FJ, van Bruggen LW, Ijzer J, Zijlstra C, Okkens AC (October 2008). "Persistent Müllerian Duct Syndrome in a Miniature Schnauzer Dog with Signs of Feminization and a Sertoli Cell Tumour". Reprod. Domest. Anim. 45 (3): 447–52. doi:10.1111/j.1439-0531.2008.01223.x. PMID 18954385.
- ↑ Online Mendelian Inheritance in Man (OMIM) 600957
- ↑ Online Mendelian Inheritance in Man (OMIM) 600956