Vision restoration therapy
Vision Restoration Therapy (VRT) is a noninvasive, nonsurgical form of Vision therapy.[1] This therapy was developed by Bernhard Sabel, Ph.D. The phenomenon underlying the therapy is visual neuroplasticity.[2]
Description of therapy
Vision Restoration Therapy (VRT) is a computer-based treatment designed to help patients with visual field defects regain visual functions through repetitive light stimulation. [1,2] The therapy is cleared by the U.S. Food and Drug Administration (FDA) for “…the diagnosis and improvement of visual functions in patients with impaired vision that may result from trauma, stroke, inflammation, surgical removal of brain tumors or brain surgery, and may also be used to improve visual function in patients with amblyopia”. Patterns of visual field loss depend on the injury, but the most common are hemianopia, loss of an entire hemisphere of vision; quadrantanopia, loss of a quadrant of vision; and scotoma, loss of an irregular section of vision.[4] The main characteristics of these visual field losses is that they persist in both eyes, and therefore, one eye cannot compensate for the deficit in the other eye.
Before the development of VRT, there was no therapy available to improve the range or sensitivity of the patient’s affected field of vision – patients were often told they “had to live with” their deficits. However, similar to recovery from motor deficits after brain injury, where repetitive stimulation has proven effective in recovery of patient functions such as movements of lower limbs, systematic repetitive visual training can also lead to increased visual sensitivity and recovery of function. To date the concept of improving vision in patients with repeated stimulation has been confirmed by a number of independent laboratories, and extended to a range of techniques. These include using moving stimuli (Krystal Huxlin, University of Rochester); flickering dots stimuli at sighted/blind field borders (Laura Julkunen, University of Turku; And D P Bergsma, Utrecht), and flashing large patterns deep in the blind field (Arash Sahraie, University of Aberdeen). In addition, VRT has been shown effective in more than 20 clinical studies where the repeated stimulation of the blind and transition areas has led to improved visual sensitivity.
Science behind the therapy
Neuroplasticity
There exist two approaches for visual neurolasticity:
- The first approach involves rescuing, regenerating, or transplanting visual neurons by biological/pharmacological methods. One example of this approach is the discovery of the regeneration of axons of retinal ganglion cells (RGCs) by introducing several proteins into the chemical environment of these cells. Some of these known proteins that induce axon growth of RGCs include laminin, Gap-43 protein, fatty acid binding protein, calmodulin, Alpha crystallin, IFN-gamma, cyclin-dependent kinase inhibitor protein, beta-hemoglobin, 60s-ribosomal protein, GAP-DH, and ADP-ribosylation factor.
- The second approach involves improving visual functions by stimulating the associated neurons in either the blind region of the visual field through different pathways or by stimulating damaged areas of the border region.[3]
Biology of visual neuroplasticity

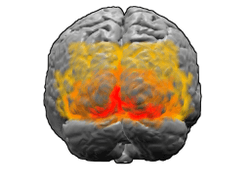
With visual neuroplasticity, reorganization of the physical structure of the brain occurs concurrently with reorganization of the visual system by new connections made by stimulated neurons. Using the imaging technique of fMRI, it was found that brain activity was altered after Vision Restoration Therapy. This associates cerebral reorganization with VRT treatment.[2][4]
The cerebrum is involved with higher brain function, and one component of the cerebrum is the primary visual cortex. The primary visual cortex is a region in the occipital lobe that can be altered by neuroplasticity to create new neuronal pathways around damaged areas to help regain lost visual functions. Sensory visual information is sent from the retina of the eye to the Lateral geniculate nucleus (LGN) in the Thalamus, which relays the visual information to the primary visual cortex by the fibers of the optic radiation. Lesions or damage to parts of the brain that cause visual field defects usually occur posterior to the optic chiasm.[5] Although the exact mechanisms that underlie regaining visual field functions through visual neuroplasticity and VRT are not yet fully known, the reorganization of the primary visual cortex is thought to make new connections and pathways in the optic radiation to the LGN to help regain visual field functions. The stimulation of existing neurons near a damaged site in the brain can form new synapses with other functional neurons to help take on and compensate for the function lost due to the damaged neurons. This is what is theorized to occur during VRT treatment.[2][3][5]
Vision Restoration Therapy stimulates the retina of the eye using repetitive points of light that flash on a computer screen. These flashing lights are aimed to stimulate the border of the blind area of a patient’s visual field. The repetitive stimulation is used to help promote visual neuroplasticity and ultimately make new neuronal connections to regain and expand the visual field.[3]
Process of therapy
VRT is a prescription therapy provided in the US by NovaVision Inc. headquartered in Boca Raton, Florida, USA, and in Europe through its operations based in Germany and the UK.
VRT is designed to identify a patient’s visual field deficit and provide customized therapy to improve vision using light-based stimuli programs. Patients undergo therapy in the comforts of their home due to it being a software-based therapy delivered to the patient’s computer over the internet. Before the actual therapy, a diagnostic algorithm in the VRT program first maps the visual field and defines the areas of visual impairment. Based upon the results of the diagnostic process, a customized, specific therapy program is then created for each patient.
This first month of this customized therapy regimen is then delivered to the patient’s computer over the Internet and the patient can begin home therapy. A typical therapy schedule comprises two daily sessions of 20-30 minutes each. Session results are recorded and monitored. The therapy is monthly adjusted to the individual’s therapy development.
With VRT therapy, the patient first focuses on a fixation point on a display screen. Then, a series of light stimuli are presented along the border of the patient’s area of visual field loss. These programmed light sequences stimulate the border zone between the “seeing” and “blind” visual fields, repetitively challenging neuronal structures responsible for processing visual information from this border zone with thousands of stimuli over the course of time.
VRT is typically performed over a six-month period twice a day for about 20-30 minutes per session, six days a week. The course of visual improvement differs from person to person: for example, some patients notice improvement already within their first month of VRT, while others only experience material benefits after the third month of treatment. The long-term twice-daily exposure to the intense and repetitive stimulation is considered to be one of the key contributors to the success of the therapy.
Skepticism
The effectiveness of VRT has been a controversial topic. Beneficial results have been researched and documented by testing small groups of patients. This has led to skepticism by some of the scientific community.[6] Even though VRT has been available for a few years now, optometrists, ophthalmologists, and other eye specialists do not regularly recommend VRT for their patients. The primary cause of this is that eye specialists rarely recommend this therapy to other eye specialists. The skepticism of VRT may be the source of the lack of recommendation.[7]
When VRT was first introduced, the primary skepticism involved the data collection methods that the VRT researchers used to quantify the effective results of using the therapy. The main argument was that the HRP data from the VRT device that was used to measure the progress of the patients was the same data used to show the effectiveness of VRT. These data would not be as reliable as data gathered using some other Perimetry technique.[8] Skeptics turned to studies that assessed VRT effectiveness using Tubinger Automatic Perimetry and Scanning laser ophthalmoscopy (SLO), which showed that no beneficial results in improving the visual field were associated with VRT use.[8] Skepticism also arose about the quality of life questionnaire surveys that patients took after VRT treatment. The possibility of the placebo effect could be present in the answering of these questionnaires.[8] Patients could have stated that their qualities of life did improve just because they had finished the therapy, even if no improvements actually occurred. Others questioned the neuroplastic mechanism behind VRT, stating that no salvageable tissue remains in the occipital lobe with vision deficits such as hemianopia. Neuroplasticity cannot make new connections according to this claim, which debunks VRT in its entirety.[8][9] It was proclaimed that eye movements were the cause of visual rehabilitation instead of self regeneration of the brain and visual neuroplasticity.[8]
Pilot studies
Pilot studies have looked into the effects of Vision Restoration Therapy in treating visual field defects that have resulted from anterior ischemic optic neuropathy and glaucoma. Although these are pilot studies and require more data, it seems promising that VRT can help restore some visual functions of patients with anterior ischemic optic neuropathy.[10]
References
- ↑ Caplan, L. R., Firlik, A., Newman, N. J., Pless, M., Romano, J. G., & Schatz, N. (2005). Vision restoration therapy. [Letter]. British Journal of Ophthalmology, 89(9), 1229-1229. doi:10.1136/bjo.2005.069773
- 1 2 3 Frequently Asked Questions: Vision Restoration Therapy: Vision Rehab after Stroke or TBI. (2007). Retrieved November 12, 2010 from NovaVision, www.novavision.com: http://www.novavision.com
- 1 2 3 Sabel, B. A. (2008). Plasticity and restoration of vision after visual system damage: An update. [Article]. Restorative Neurology and Neuroscience, 26(4-5), 243-247.
- ↑ Vision Restoration Therapy Shown To Improve Brain Activity In Brain Injured Patients. (2007). Retrieved September 11, 2010 from ScienceDaily, http://www.sciencedaily.com/releases/2007/08/070814082950.htm
- 1 2 Farah, M. J. (2000). The Cognitive Neuroscience of Vision. Malden, Massachusetts: Blackwell Publishers Inc.
- ↑ Mueller, I., Mast, H., & Sabel, B. A. (2007). Recovery of visual field defects: A large clinical observational study using vision restoration therapy. [Article]. Restorative Neurology and Neuroscience, 25(5-6), 563-572.
- ↑ Dr. Mona Patel, Doctor of Optometry at the Ochsner Clinic LLC in Marrero,LA. Interview date October 25, 2010.
- 1 2 3 4 5 Horton, J. C. (2005). Disappointing results from Nova Vision's visual restoration therapy. [Editorial Material]. British Journal of Ophthalmology, 89(1), 1-2. doi:10.1136/bjo.2004.058214
- ↑ Disappointing results from Nova Vision’s visual restoration therapy
- ↑ Jung, C. S., Bruce, B., Newman, N. J., & Biousse, V. (2008). Visual function in anterior ischemic optic neuropathy: Effect of Vision Restoration Therapy - A pilot study. [Article]. Journal of the Neurological Sciences, 268(1-2), 145-149. doi:10.1016/j.jns.2007.12.001
1. Kasten E, Wuest S, Behrens-Baumann W, Sabel BA (1998). Computer-based training for the treatment of partial blindness. Nature Medicine; 4 (9): 1083-1087
2. Marshall RS, Ferrera JJ, Barnes A, Zhang X, O’Brien KA, Chmayssani M, Hirsch J, Lazar RM (2007). Brain activity associated with stimulation therapy of the visual border- zone in hemianopic stroke patients. Neurorehabilitation and Neural Repair; 22(2): 136-144
3. Plow EB, Obretenova SN, Fregni F, Pascual-Leone A, Merabet LB (2012). Comparison of Visual Field Training for Hemianopia With Active Versus Sham Transcranial Direct Cortical Stimulation. Neurorehabilitation and Neural Repair; 20 (10): 1–11
4. Farah, M. J. (2000). The Cognitive Neuroscience of Vision. Malden, Massachusetts: Blackwell Publishers Inc.
5. Huxlin KR, Martin T, Kelly K, Riley M, Friedman DI, Burgin WS, Hayhoe M (2009). Perceptual relearning of complex visual motion after V1 damage in humans. The Journal of neuroscience : the official journal of the Society for Neuroscience; 29(13): 3981-91.
6. Das A, Tadin D, Huxlin KR (2014). Beyond blindsight: properties of visual relearning in cortically blind fields. The Journal of neuroscience : the official journal of the Society for Neuroscience; 34(35): 11652-64.
7. Julkunen L, Tenovuo O, Vorobyev V, et al. (2006). Functional brain imaging, clinical and neurophysiological outcome of visual rehabilitation in a chronic stroke patient. Restor Neurol Neurosci.; 24: 123-132.
8. Julkunen L, Tenovuo O, Jääskeläinen S, Hämäläinen H (2003). Rehabilitation of chronic post-stroke visual field defect with computer-assisted training. Restor Neurol Neurosci.; 21: 19-28.
9. Bergsma DP, van der Wildt G (2010). Visual Training of Cerebral Blindness patients gradually enlarges the visual field. Br J Ophthalmol; 94:88-96.
10. Raemaekers M, Bergsma DP, van Wezel RJ, van der Wildt GJ, et al. (2011). Effects of vision restoration training on early visual cortex in patients with cerebral blindness investigated with functional magnetic resonance imaging. Journal of Neurophysiology; 105(2):872-82.
11. Trevethan CT, Urquhart J, Ward R, Gentleman D, Sahraie A (2012). Evidence for perceptual learning with repeated stimulation after partial and total cortical blindness. Advances in Cognitive Psychology; 8 (1): 29-37.
12. Sahraie, A (2010). Improved detection following Neuro-Eye Therapy in patients with post-geniculate brain damage. Experimental Brain Research; 206 (1): 25-34.
13. Romano JG, Schulz P, Kenkel S, Todd DP (2008). Visual field changes after a rehabilitation intervention: Vision restoration therapy. Journal of the Neurological Sciences; 273(1-2): 70-74.
14. Mueller I, Mast H, Sabel BA (2007). Recovery of visual field defects: A large clinical observational study using vision restoration therapy. Restor Neurol Neurosci.; 25(5-6): 563-572.
15. See website: www.novavision.com
16. See website: www.neuroeyecoach.com
17. Reinhard J, Schreiber A, Schiefer U, et al. (2005). Does visual restitution training change absolute homonymous visual field defects? A fundus controlled study. Br J Ophthalmol.; 89:30-35.
18. Horton JC (2005). Disappointing results from Nova Vision's visual restoration therapy. Br J Ophthalmol.; 89(1): 1-2.
19. Sabel BA (2006). Vision restoration therapy and raising red flags too early. Br. J. Ophthalmol.; 90: 659-660.
20. Mueller I, Poggel DA, Kenkel S, et al. (2003). Vision Restoration Therapy after brain damage: subjective improvements of activities of daily life and their relationship to visual field enlargements. Visual Impairment Research; 5: 157-178.
21. Gall C et al. (2008). Vision- and health-related quality of life before and after vision restoration training in cerebrally damaged patients. Restor Neurol Neurosci ; (26): 341-353.