Subgaleal hemorrhage
| Subgaleal hemorrhage | |
|---|---|
 | |
| Newborn Scalp bleeds | |
| Classification and external resources | |
| Specialty | pediatrics |
| ICD-10 | P12, S00.0 (when not due to a birth injury) |
| ICD-9-CM | 767.1 |
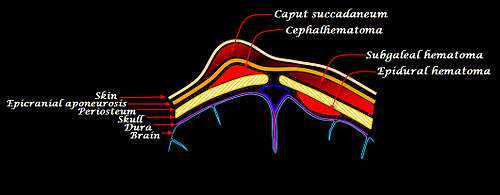
Subgaleal hemorrhage or hematoma is bleeding in the potential space between the skull periosteum and the scalp galea aponeurosis.
Causes
The majority (90%) result from applying a vacuum to the head at delivery (Ventouse assisted delivery). The vacuum assist ruptures the emissary veins (connections between dural sinus and scalp veins) leading to accumulation of blood under the aponeurosis of the scalp muscle and superficial to the periosteum.[1] Subgaleal hematoma has a high frequency of occurrence of associated head trauma (40%), such as intracranial hemorrhage or skull fracture. The occurrence of these features does not correlate significantly with the severity of subgaleal hemorrhage.
Symptoms
The diagnosis is generally a clinical one, with a fluctuant boggy mass developing over the scalp (especially over the occiput) with superficial skin bruising. The swelling develops gradually 12–72 hours after delivery, although it may be noted immediately after delivery in severe cases. The hematoma spreads across the whole calvaria as its growth is insidious and may not be recognized for hours. If enough blood accumulates a visible fluid wave may be seen. Patients can develop raccoon eyes.
Patients with subgaleal hematoma may present with hemorrhagic shock.[2] The swelling may obscure the fontanel and cross suture lines (distinguishing it from cephalohematoma). Watch for significant hyperbilirubinemia. The long-term prognosis is generally good. Laboratory studies consist of a hematocrit evaluation.
Management
Management consists of vigilant observation over days to detect progression. The subgaleal space is capable of holding up to 50% of a newborn baby's blood and can therefore result in acute shock and death. Fluid bolus may be required if blood loss is significant and patient becomes tachycardic. Transfusion and phototherapy may be necessary. Investigation for coagulopathy may be indicated.
See also
References
- ↑ AAP Textbook of Pediatrics
- ↑ Ronald S. Gibbs; David N. Danforth; Beth Y Karlan; Arthur F Haney (2008). Danforth's obstetrics and gynecology. Lippincott Williams & Wilkins. p. 470. ISBN 978-0-7817-6937-2. Retrieved 12 April 2010.