Tracheal tube
| Tracheal tube | |
|---|---|
| Intervention | |
 | |
| ICD-9-CM | 96.04 |
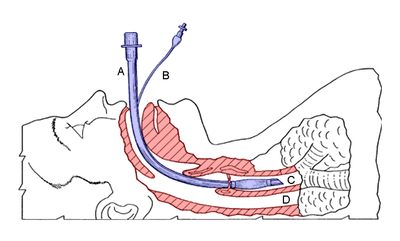
A tracheal tube is a catheter that is inserted into the trachea for the primary purpose of establishing and maintaining a patent airway and to ensure the adequate exchange of oxygen and carbon dioxide.
Many different types of tracheal tubes are available, suited for different specific applications:
- An endotracheal tube is a specific type of tracheal tube that is nearly always inserted through the mouth (orotracheal) or nose (nasotracheal).
- A tracheostomy tube is another type of tracheal tube; this 2–3-inch-long (51–76 mm) curved metal or plastic tube may be inserted into a tracheostomy stoma (following a tracheotomy) to maintain a patent lumen.
- A tracheal button is a rigid plastic cannula about 1 inch in length that can be placed into the tracheostomy after removal of a tracheostomy tube to maintain patency of the lumen.
History
Portex Medical (England and France) produced the first cuffless plastic 'Ivory' endotracheal tubes, in conjunction with Magill's design later adding a cuff as manufacturing techniques became more viable, these were glued on by hand to make the famous Blue-line tube copied by many other manufacturers. Mallinckrodt GmBH developed the disposable endotracheal tube and produced a plethora of design variations, adding the 'Murphy Eye' to their tubes in case of 'accidental' placement of the tube to avoid right bronchial occlusion. David S. Sheridan was one of the manufacturers of the American markets "disposable" plastic tracheal tube now used routinely in surgery. Previously, red rubber (Rusch-Germany) tubes were used, then sterilized for re-use..
Applications
Tracheal tubes can also be used to deliver oxygen in higher concentrations than found in air, or to administer other gases such as helium, nitric oxide, nitrous oxide, xenon, or certain volatile anesthetic agents such as desflurane, isoflurane, or sevoflurane. Tracheal tubes may also be used as a route for administration of certain medications such as salbutamol, atropine, epinephrine, ipratropium, and lidocaine. Tracheal tubes are commonly used for airway management in the settings of general anesthesia, critical care, mechanical ventilation, and emergency medicine.
Endotracheal tube
| Age | Weight | (Inner) diameter (mm) |
|---|---|---|
| Premie | 3 kg | 2.5–3.0[1] |
| 0–6 months | 3.5 kg | 3.0–3.5[1] |
| 6–12 months | 7 kg | 3.5–4.0[1] |
| 1–3 years | 10–12 kg | 4.0–4.5[1] |
| 4–7 years | 16–18 kg | 5.0–5.5[1] |
| 8–10 years | 24–30 kg | 5.5–6.5[1] |
| Adult female | 7.0-7.5[2] | |
| Adult male | 8.0-9.0[2] |


Most endotracheal tubes today are constructed of polyvinyl chloride, but specialty tubes constructed of silicone rubber, latex rubber, or stainless steel are also widely available. Most tubes have an inflatable cuff to seal the trachea and bronchial tree against air leakage and aspiration of gastric contents, blood, secretions, and other fluids. Uncuffed tubes are also available, though their use is limited mostly to pediatric patients (in small children, the cricoid cartilage, the narrowest portion of the pediatric airway, often provides an adequate seal for mechanical ventilation).
Types of endotracheal tube include oral or nasal, cuffed or uncuffed, preformed (e.g. RAE (Ring, Adair, and Elwyn) tube), reinforced tubes, and double-lumen endobronchial tubes. For human use, tubes range in size from 2 to 10.5 mm in internal diameter (ID). The size is chosen based on the patient's body size, with the smaller sizes being used for pediatric and neonatal patients. Tubes larger than 6 mm ID usually have an inflatable cuff. Originally made from red rubber, most modern tubes are made from polyvinyl chloride. Those placed in a laser field may be flexometallic. Robertshaw (and others) developed double-lumen endo-bronchial tubes for thoracic surgery. These allow single-lung ventilation while the other lung is collapsed to make surgery easier. The deflated lung is re-inflated as surgery finishes to check for fistulas (tears). Another type of endotracheal tube has a small second lumen opening above the inflatable cuff, which can be used for suction of the nasopharngeal area and above the cuff to aid extubation (removal). This allows suctioning of secretions which sit above the cuff which helps reduce the risk of chest infections in long-term intubated patients.
The "armored" endotracheal tubes are cuffed, wire-reinforced, silicone rubber tubes which are quite flexible but yet difficult to compress or kink. This can make them useful for situations in which the trachea is anticipated to remain intubated for a prolonged duration, or if the neck is to remain flexed during surgery. Polyvinyl chloride tubes are relatively stiff in comparison. Preformed tubes (such as the oral and nasal RAE tubes, named after the inventors Ring, Adair and Elwyn) are also widely available for special applications. These may also be constructed of polyvinyl chloride or wire-reinforced silicone rubber. Other tubes (such as the Bivona Fome-Cuf tube) are designed specifically for use in laser surgery in and around the airway. Various types of double-lumen endotracheal (actually, endobronchial) tubes have been developed (Carlens,[3] White, Robertshaw, etc.) for ventilating each lung independently—this is useful during pulmonary and other thoracic operations.
Tracheostomy tube
Several types of tracheostomy tubes are available, depending on the requirements of the patient, including Shiley, Bivona (a silicon tube with metal rings that are good for airways with damage to the tracheal rings or otherwise not straight), and fenestrated.
Tracheal button
A tracheal button is generally used in people with severe obstructive sleep apnea, who often wear this device during waking hours and remove it while sleeping to ensure a patent airway and reduce the risk of asphyxiation. Since the tube does not extend far into the trachea, it is easy to breathe and speak with the device in place.
See also
References
- 1 2 3 4 5 6 "Equipment Sizing Chart". University of Iowa Children's Hospital. Retrieved 2015-11-07.
- 1 2 Varshney, Manu; Kumar, Rakesh; Sharma, Kavita; Varshney, PreetiG (2011). "Appropriate depth of placement of oral endotracheal tube and its possible determinants in Indian adult patients". Indian Journal of Anaesthesia. 55 (5): 488. doi:10.4103/0019-5049.89880. ISSN 0019-5049.
- ↑ Carlens E (October 1949). "A new flexible double-lumen catheter for bronchospirometry". J Thorac Surg. 18 (5): 742–746. PMID 18149050.
Further reading
- Brodsky, JB; Lemmens, JM (2003). "Left Double-Lumen Tubes: Clinical Experience With 1,170 Patients" (PDF). Journal of Cardiothoracic and Vascular Anesthesia. 17 (3): 289–98. doi:10.1016/S1053-0770(03)00046-6. PMID 12827573.
External links
- Resource explaining various types of endotracheal tubes
- ACLS algorithms with manual that includes further tracheal tube information.