Golfer's elbow
| Golfer's elbow | |
|---|---|
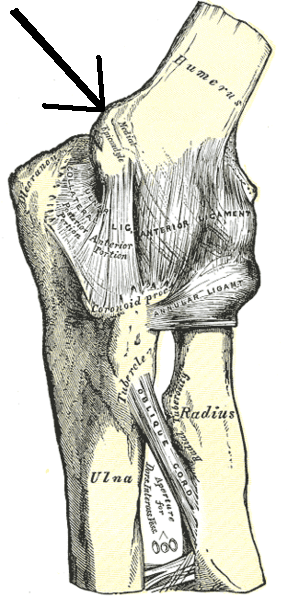 | |
| Left elbow-joint, showing anterior and ulnar collateral ligaments. (Medial epicondyle labeled at center top.) | |
| Classification and external resources | |
| Specialty | rheumatology |
| ICD-10 | M77.0 |
| ICD-9-CM | 726.31 |
| DiseasesDB | 5356 |
| eMedicine | sports/74 pmr/74 |
Golfer's elbow, or medial epicondylitis, is tendinosis of the medial epicondyle of the elbow. It is in some ways similar to tennis elbow.
The anterior forearm contains several muscles that are involved with flexing the digits of the hand, and flexing and pronating the wrist. The tendons of these muscles come together in a common tendinous sheath, which originates from the medial epicondyle of the humerus at the elbow joint. In response to minor injury, or sometimes for no obvious reason at all, this point of insertion becomes inflamed.
Causes
The condition is called Golfer's Elbow because in making a golf swing this tendon is stressed, especially if a non-overlapping (baseball style) grip is used; many people, however, who develop the condition have never handled a golf club. It is also sometimes called Pitcher's Elbow[1] due to the same tendon being stressed by the throwing of objects such as a baseball, but this usage is much less frequent. Other names are Climber's Elbow and Little League Elbow: all of the flexors of the fingers and the pronators of the forearm insert at the medial epicondyle of the humerus to include: pronator teres, flexor carpi radialis, flexor carpi ulnaris, flexor digitorum superficialis, and palmaris longus;[2] making this the most common elbow injury for rock climbers, whose sport is very grip intensive. The pain is normally caused due to stress on the tendon as a result of the large amount of grip exerted by the digits and torsion of the wrist which is caused by the use and action of the cluster of muscles on the condyle of the ulna.[3]
Epicondylitis is much more common on the lateral side of the elbow (tennis elbow), rather than the medial side. In most cases, its onset is gradual and symptoms often persist for weeks before patients seek care. In golfer's elbow, pain at the medial epicondyle is aggravated by resisted wrist flexion and pronation, which is used to aid diagnosis. On the other hand, tennis elbow is indicated by the presence of lateral epicondylar pain precipitated by resisted wrist extension.[4][5] Although the condition is poorly understood at a cellular and molecular level, there are hypotheses that point to apoptosis and autophagic cell death as causes of chronic lateral epicondylitis.[6] The cell death may decrease the muscle density and cause a snowball effect in muscle weakness - this susceptibility can compromise a muscle's ability to maintain its integrity. So athletes, like pitchers, must work on preventing this cell death via flexibility training and other preventive measures.
Treatment
Non-specific palliative treatments include:
- Non-steroidal anti-inflammatory drugs (NSAIDs): ibuprofen, naproxen or aspirin
- Heat or ice
- A counter-force brace or "elbow strap" to reduce strain at the elbow epicondyle, to limit pain provocation and to protect against further damage.
Before anesthetics and steroids are used, conservative treatment with an occupational therapist may be attempted. Before therapy can commence, treatment such as the common rest, ice, compression and elevation (R.I.C.E.) will typically be used. This will help to decrease the pain and inflammation; rest will alleviate discomfort because golfer's elbow is an overuse injury. The patient can use a tennis elbow splint for compression. A pad can be placed anteromedially on the proximal forearm.[7] The splint is made in 30–45 degrees of elbow flexion. A daytime elbow pad also may be useful, by limiting additional trauma to the nerve.
Therapy will include a variety of exercises for muscle/tendon reconditioning, starting with stretching and gradual strengthening of the flexor-pronator muscles. Strengthening will slowly begin with isometrics and progresses to eccentric exercises helping to extend the range of motion back to where it once was. After the strengthening exercises, it is common for the patient to ice the area.[7]

Simple analgesic medication has a place, as does more specific treatment with oral anti-inflammatory medications (NSAIDs). These will help control pain and any inflammation.[7] A more invasive treatment is the injection into and around the inflamed and tender area of a long-acting glucocorticoid (steroid) agent. After causing an initial exacerbation of symptoms lasting 24 to 48 hours, this may produce a resolution of the condition in some five to seven days.
The ulnar nerve runs in the groove between the medial humeral epicondyle and the olecranon process of the ulna. It is most important that this nerve should not be damaged accidentally in the process of injecting a golfer's elbow.
If all else fails, epicondylar debridement (a surgery) may be effective. The ulnar nerve may also be decompressed surgically.[7]
The overall prognosis is good. Few patients will need to progress to steroid injection and even fewer, less than 10%, will need surgical intervention.[7]
See also
References
- ↑ "Pitcher's Elbow - Stanford Sports Medicine - Stanford Medical Outpatient Center". Stanford University Medical Center. Retrieved 9 September 2009.
- ↑ http://connect.mcgraw-hill.com/connect/hmEBook.do?setTab=sectionTabs
- ↑ http://www.webmd.com/fitness-exercise/golfers-elbow-basics
- ↑ Wilson, JJ; Best, TM (1 September 2005). "Common overuse tendon problems: A review and recommendations for treatment". Am Fam Physician. 72 (5): 811–8. Retrieved 4 June 2012.
- ↑ Matthews, Phillip. "Acute Classification in Tennis and Golfer's Elbow" (PDF). Oxford Journal. Retrieved 1 March 2012.
- ↑ Chen, J. "In chronic lateral epicondylitis, apoptosis and autophagic cell death occur in the extensor carpi radialis brevis tendon.". PubMed. Retrieved 1 March 2012.
- 1 2 3 4 5 Gibbs, Sharon J.; Dauber, Kenneth S. (8 September 2014). "Medial Epicondylitis". eMedicine. Retrieved 13 January 2014.