Food desert


A food desert exists when particularly nutritious food is difficult to obtain due to availability, affordability, distance, or number of supermarkets in a given area, urban or rural.[1][2] This has health and diet implications in individuals living in these areas where nutritious food is not readily available, though some of these claims such as linking food deserts with obesity in children are disputed.[2][3][4]
Food deserts are associated with poor food access as racially and socioeconomically discriminatory policies and patterns of development such as Redlining have resulted in uneven distribution of resources including supermarkets.[5] Researchers are interested in understanding the relationship between these affected areas and policies, but in varying capacities. They have employed a variety of methods to assess food access including: directories and census data, focus groups, food store assessments, food use inventories, GIS technology, interviews, questionnaires and surveys measuring consumers food access perceptions.[6] For example, the U.S. Department of Agriculture Food Access Research Atlas provides an interactive map that identifies areas of low food access in low income urban and rural areas.[7]
Definitions
While there are a myriad of definitions for the term food desert, none of them are necessarily mutually exclusive from one another as each recognizes that food deserts exist when people have limited access to particularly nutritious foods. However, because different parameters and measures may be used depending on the group, variations in definitions exist according to the:
- type of area, whether it be urban or rural[8]
- economic barriers and affordability of accessing nutritious foods, including the cost of transportation, price of foods, and incomes of those in the area[6][9][10]
- distance to the nearest supermarket or grocery store[11]
- amount of supermarkets in the given area[11]
- type of foods offered, whether it be fresh or prepared[6][10]
- nutritional values of the foods offered[12]
The multitude of definitions which vary by country have fueled controversy over the existence of food deserts.[6]
Measuring food access

Distance
Distance-based measurements are commonly used to measure food accessibility and to distinguish whether or not a community is a food desert. There is no one set method on how to determine the distance, but it is commonly measured with the center of an area to the nearest grocery store.[13]
The United States Department of Agriculture Economic Research Service (USDA ERS) measures distance by dividing the country into multiple 0.5 km square grids. The distance from the geographical center of each grid to the nearest grocery store is measured to determine food accessibility for the people living in that grid.[13][14] Health Canada divides areas into buffer zones ,which is formed by using people’s homes, schools or workplaces as the center. The Euclidean distance or the shortest route distance between the two points of interest is then measured for gaining food access data.[15]
Different factors can be excluded or included into the measurement to vary the scale of distance. The online mapping tool “Food Access Research Atlas” uses four different measurement standards when measuring an area of low food access.[16]
The first measurement standard uses the original food desert mapping tool “Food Desert Locator”, which disregards other possible factors, and defines low food access areas or food deserts, as having at least 33% or 500 people of a census tract's population in an urban area living 1 mile (10 miles for rural area) away from a large grocery store or a supermarket.[13][17]
The second and third measurement standards simply adjust the scale of distance while taking income into consideration, and defines a food desert as the low income census tract residing at least 0.5 miles away in urban areas (10 miles in rural areas) or 1 mile away in urban areas (20 miles in rural areas) from the large grocery store.[16]
The fourth measurement standard takes vehicular mobility into account. A food desert exists if 100 households or more, which have no access to vehicles, lives at least 0.5 miles away from the nearest large grocery store; for populations with access to vehicles, 500 households or more living at least 20 miles away.[16][18]
Fresh food availability
A food retailer is typically considered healthy food provider if it sells a variety of fresh food, such as fruits and vegetables. Some types of fresh food retailers are:
- supermarkets
- local grocery stores
- warehouse clubs
- community gardens
- farmers’ markets
Other food retailers, such as fast food restaurants and convenience stores, are not classified as sources of healthy, fresh food.[13] These food providers usually only provide a limited variety of foods that do not make up a healthy diet. A possible factor affecting obesity and other "diet-related diseases” is the closer proximity of fast food restaurants and convenience stores in comparison to “full-access” grocery stores.[13]
Countries from all over the world have differing dietary models and views on nutrition. These distinct national nutrition guides are a part of the controversy surrounding the definition of food deserts. A food desert is defined as an area with limited access to nutritious foods, so a universal identification of food deserts cannot be created without a global consensus on nutrition.
Income and food prices
Another criteria of measuring food access is based on the level of income. Section 7527 on Food, Conservation, and Energy Act of 2008, the food desert is also defined as “an area with limited access to affordable and nutritious food, particularly such an area composed of predominantly lower-income communities.”[19] Accessing healthy food becomes a bigger problem with in low-income neighborhoods because of different components brought up after their level of income. According to USDA, when measuring food access, researchers should “consider...to measure prices of foods faced by individuals and areas” and how “prices affect the shopping and consumption behaviors of consumers.”[20] Through the experiment on measuring economics access to supermarkets on low-income communities in King County, Washington, the researchers address how we can measure food access[21] In this experiment, they identify that “Measures of access to food must include travel duration and mode and supermarket food costs,” and these two aspects are greatly influenced by the level of income.[21]
The residents living in low-income neighborhoods often find difficulty to access grocery stores and supermarkets that offer a variety of fresh and nutritious foods. Instead, they are limited to shop at convenience stores and small neighborhood stores that do not have a full range of affordable and healthy foods. According to The Reinvestment Fund (TRF) and Low Supermarket Access areas (TRF 2012), the density of car ownerships is much lower in poorer communities.[17] Accessing healthy foods then becomes more difficult without reliable transportation. The Food Access Research Atlas (ERS 2013) maps out the measurement of food access in both low- and high-income communities. Under this measure, they point out the significance of number of cars within and a number of supermarkets in the area.[17]
In another hand, healthy food may be also out of their reach because healthy foods normally cost more than unhealthy fast foods. Those impacted by food deserts have an average income between $5,000 and $20,000 annually.[22] This leads to the situation that they have cheap foods to fit their budgets. According to USDA, “Research that considers the prices paid for the same food across household income levels indicates that while some of the very poorest households—those earning less than $8,000 per year—may pay between 0.5 percent and 1.3 percent more for their groceries than households earning slightly more, households earning between $8,000 and $30,000 tend to pay the lowest prices for groceries, whereas higher income households pay significantly higher prices.”[20] Researchers have examined that area settings impact on food affordability and nutritious foods are cheaper in more advantaged neighbourhoods. “Several studies have found retail prices for the same foods to be higher in deprived areas,” where there is a lack of availability of supermarkets and food stores. Even when there are healthy foods available, it may be not affordable for many residents in poorer communities.[15]
Implications
Food retailers are not encouraged to develop in low-income areas because of market conditions such as high development costs and a perceived low return in investment. Because of this, residents of low-income areas in inner cities or of rural areas have less access to affordable healthful foods.[13] Access to healthy foods like fresh fruits and vegetables, low-fat milk, and whole grains is a key component to good health and well being. Individuals who have access to supermarkets in general tend to have healthier diets and are at lower risk of chronic disease such as diabetes.[23]
Affordability
Research indicates that low-income households shop where food prices are lower, and generally cannot afford healthful foods. Compared with residents of higher-income neighborhoods, low SES (socioeconomic status) individuals generally have diets higher in meat and processed foods with a low intake of fruits and vegetables.[24]
According to 2010 reports from the U.S. Department of Agriculture, there are approximately 29.7 million people (9.7% of the population) living in low-income areas that are more than 1 mile from a supermarket.[13] Researchers have determined that the physical distance from full service supermarkets leaves residents more likely to purchase food from convenience stores or corner shops that stock mainly cheap, processed foods or foods high in fat, sugar, and sodium—also known as “energy-dense” foods.[25]
Chain supermarkets, which benefit from economies of scale to offer consumers low prices are also less prevalent in low-income urban areas. For example, only 22% of the chain supermarkets in Minneapolis were located in the inner-city compared to more than 50% of the non-chain supermarkets.[26]
Fringe food retailers in food deserts can have a 30-60% markup on prices, provide a limited selection of products and a dominant marketing of processed foods. Report findings from the United States Department of Agriculture reveal that prices for similar goods are on average higher at convenience stores than at supermarkets.[13]
In addition, low-income individuals are more likely to purchase inexpensive fats and sugars over fresh fruits and vegetables that are more expensive on a per calorie basis.[2] On average, the most energy-dense foods only cost $1.76 per 1,000 calories, compared to $18.16 per 1,000 calories for low-energy nutritious foods.[27] As a result, people of low SES ultimately spend up to 37% more on their food purchases.[28]
In addition to higher priced grocery stores, many people living in low income neighborhoods spend more on transportation to bring their groceries home. The Colorado Health Foundation found that taxi cab drivers make more trips to grocery stores at the beginning of the month when food stamps are distributed and at the end of the month before they expire.[23]
Health Outcomes
Food deserts are correlated with many poor health outcomes.
- Many studies have found a link between better access to supermarkets and a lowered risk of obesity. Conversely, many studies have also found an association between better access to convenience stores and a higher risk of obesity.[13]
- It has also been shown that proximity to fast food restaurants is correlated with a higher BMI, and proximity to a grocery store is correlated with a lower BMI.[13] Research has indicated those who eat fast food twice, rather than once, per week already see an 86% increase in obesity.[29]
- A lack of plant-based foods (fruits, vegetables, nuts, whole grains) is correlated with an increased risk of cardiovascular disease.[13]
- Beverages sweetened with sugar are linked to a higher risk of obesity, diabetes, and cardiovascular disease.[13]
- It has been shown that severe deficiencies in nutrients (notably essential vitamins, minerals, and omega-3 fatty acids) is linked to depression, bipolar disorder, schizophrenia, and obsessive-compulsive disorder (OCD).[30]
However, it is important to note that although there have been correlations found, the causal pathways are complex and not yet fully understood. Most of the studies done on food environments and health are cross-sectional and thus cannot make causal conclusions. Improvements in research are needed before causal relationships can be explicitly defined.[13]
Rural food deserts
There are different criteria for classifying a rural food desert and an urban food desert. The main factor in deciding classification is based on the distance of residents from the nearest supermarket. In a rural food desert, residents have to drive 10 miles or more to the nearest grocery store whereas in an urban food desert, residents must drive 10 miles or more to the nearest healthy food vendor.[31] This means that 20 percent of rural areas are food deserts.[32] Within these counties, there are approximately 2.4 million individuals determined to have low access to a large supermarket.[33][34] Though this may seem like one small difference in the categorization of food deserts, the rural and urban areas differ in economics and transportation, among other things.[35][36]
In terms of transportation differences, in urban areas there is usually public transportation such as buses and trains available (though people may have to take multiple to get to their destination), and a lot of private transportation, but in rural areas, there is typically little to no public transportation even though the grocery stores are far from home.[35] To worsen the matter, studies have shown that people in rural food deserts have longer commutes to work than people in other rural areas, which may be a result of the heavier reliance on public transportation. In contrast, people in urban food deserts have slightly shorter commutes to work than people in other urban areas because there is higher amounts of private transportation vehicles, walking, and biking in urban food deserts. Fortunately, improvement in vehicle availability over the past couple of decades has been helping disadvantaged residents overcome economic barriers and food access barriers in both rural and urban food deserts.[37]
Regarding economic differences, when controlling for the same products, people in urban areas pay anywhere from 3 to 37 percent more than those in rural areas. In both areas though, healthy food is, unsurprisingly, more expensive. This is especially the case in food deserts.[35] This is doubly an issue considering that all food deserts are tied to high poverty rates and low incomes.[37]
Economic pressures
There is an increased risk of rural food deserts as market pressures continue to negatively impact small grocers. Smaller grocers in rural areas struggle to be profitable for many reasons, such as low sales volumes, which makes it difficult to meet wholesale food supplier’s minimum purchasing requirements.[38] Another reason why they struggle is because they have the market power to increase the prices and decrease the supply since they are located in areas where other grocery stores are scarce and the consumers have no other options.[39] This then leads to increased prices in low-income areas, where food deserts are most commonly found. Various studies conducted have found that people who purchase their groceries in small grocery stores around their neighborhood, end up paying up to 37 percent more for the same products in supermarkets located urban areas.[35] The market pressures experienced by small grocers in rural areas also lend to groceries being more expensive in these areas than in urban areas. For example, in New Mexico the same basket of groceries cost $85 for rural residents, and $55 for urban residents.[32] However, this is not true of all rural areas. A study in Iowa showed that four rural food desert counties had lower costs on key foods that make up a nutritionally balanced diet than did the nearby larger supermarkets.[8]
According to many studies conducted, there are three times as many supermarkets in wealthy areas than in poor areas. And the grocery stores in low income communities don’t have as much variety.[35] “Economies of scale, which is when the costs of operating a store decrease as store size increases, and economies of scope, which is when the costs decrease as more product variety increases, suggests that larger stores that offer greater variety can do so and offer lower prices. Both factors may account for the ability of larger stores to survive more easily than smaller stores.”[39] Small grocers tend to offer less variety and less produce as a result.
Small grocers don’t generally offer fruits and vegetables because they are more expensive compared to processed foods, especially in food deserts where many low-income families are located. In the United States between 1989 and 2005, the price of fruits and vegetables increased 75 percent while the price of processed foods dropped more than 26 percent.[35] Even though adopting an unhealthy diet may be economically cheaper, the consequences can be detrimental. This is one of the main reasons why low-income populations and minorities are more predisposed to suffer from obesity, diabetes and cardiovascular disease.[35]
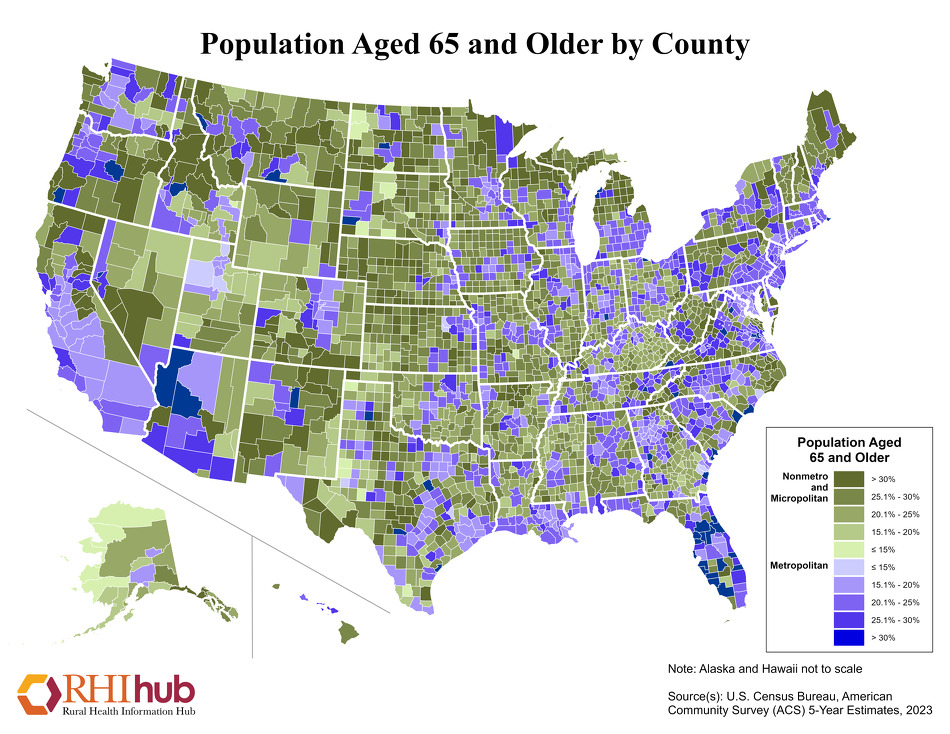
Barriers to food access for elderly living in rural food deserts
As of 2007, the elderly made up 7.5 million of the 50 million people living in rural America.[40] The U.S Census website includes maps showing the percentage of residents aged 65 and older.[41] Of these elderly citizens, nearly a half million live in rural food deserts and are food insecure, while many more may be at risk.[33][34] A study by Sharkey, et al. from seniors in the Brazos Valley showed that 14% couldn’t make their monthly allotment of food supplies last, 13% couldn’t eat balanced meals and 8.3% had to make their meals smaller or skip them.[42]
{kind=link}
Although food deserts affect a wide range of demographics, elders are particularly affected by the obstacles presented by rural food deserts because they have less access to easy and efficient means of transportation, they have limited mobility and time, and they have more specific and sensitive nutritional needs. Elders also experience difficulties in urban food deserts, but this demographic is improportionally affected by rural food deserts, because they are more likely to live in rural areas,[43] challenges associated with transportation affect them more and a higher percentage live on fixed incomes (from programs like Social Security).
Transportation
Seniors often have limited means of transportation in rural food deserts because they are much less likely to own a vehicle and drive. Studies show that at age 75, only 69% of elderly people still drive[44] (and woman and minorities drive even less),[45] which, when coupled with a lack of decent public transportation services, especially in rural areas, makes it harder for the elderly population to get food.[46] As a result, it is 9.6% more probable that elders without a car living in a food desert will skip meals than those with one.[47] Because of their lack of access to vehicles, older people are more likely to be dependent on those in their community to get food.[48]
Inability to Leave the Home
Also, seniors have constraints that make it difficult for them to leave their home, including factors such as lack of mobility, health ailments, caring for sick loved ones, and mental health concerns. Although these concerns are not limited to rural elders specifically, this combined with the transportation obstacles found in rural food deserts adds another layer of difficulty for this population. Elders often have health constraints and limited mobility, with 47% of people age 75 and over reporting some sort of physical difficulty, 27% and 15.3% reporting extreme difficulty walking a quarter of a mile and carrying 10 pounds respectively, all of which makes it very difficult to grocery shop in rural areas.[49] Also, elders are much more likely to have a sick spouse or person in the community that they have to monitor or take care of at all times, which makes it much harder to find the time to go to the grocery store, especially when it is 10+ miles away, which is the definition of a rural food desert.[31][45] Finally, studies suggest that depression (which 7 million people age 65 and older experience each year)[50] makes elders more at risk for the dangers posed by rural food deserts, especially malnutrition.[51]
Nutritional Concerns
Studies show that food insecurity leads to many health effects for elderly adults including lower BMI, limited activity and malnutrition.[47] The elderly are more sensitive to their diets and can’t handle the amount of sugar and sodium found in processed foods. They also need more nutrients because over time, digestive tracts become less efficient in nutrient absorption.[52] Also, the elderly tend to have existing diseases and/or take medications that interfere with nutrient absorption.[53] Therefore, any nutrients present in the cheaper, highly processed food are less likely to be absorbed. If an elderly person doesn’t have consistent access to enough fruits and vegetables and the proper variety of nutrients, as is the case in rural food deserts, it makes them more at risk for health problems and future ailments.[54]
Proposed solutions to rural food deserts
- Subsidized financing, such as the Health Food Financing Initiative, for food retailers in rural areas to increase retailers, stores, and farmers markets[35]
- Using the cooperative or community-owned grocery store model[35]
- Farmers markets financially help small farmers and increase access to residents[35]
- Encouraged to accept Supplemental Nutrition Assistance Program (SNAP) and the Supplemental Nutrition Program for Women, Infants and Children (WIC)
- Residents in community-supported agriculture programs (CSAs) must commit to buying some produce from a local farmer annually
- Farm-to-school initiatives allow farmers and public schools to collaborate in either selling and buying fresh food directly or in incorporating gardens in meals[35]
- Food pantries directly help communities and children in need fill the gaps during food insecurity[35]
- Increasing community education and outreach about diet and health to improve likelihood of choosing healthy, nutritious foods[35]
- Prime examples are the Supplemental Nutrition Assistance Program (SNAP) Ed and Expanded Food and Nutrition Education Program (EFNEP)
- Communities show a desire for education in nutritious food and food prep, with 89.3% in one study indicating they would be either "highly interested" or "interested" in education on preparing healthier food options.[55]
- Increasing mobility through improving public transportation access and availability[37]
- Creating more alternative forms of transportation for safer and cheaper access[37]
- Pennsylvania's Fresh Food Financing Initiative[37]
- New York City’s Healthy Bodegas Initiative[37]
Racial, ethnic, and socioeconomic disparities

Health disparities related to food access and consumption are associated with residential segregation, low incomes, and neighborhood deprivation.
In a study on urban food environments, participants described the lack of supermarkets as both a “practical impediment to healthful food purchase and a symbol of their neighborhoods’ social and economic struggles".[56] Within cities, there are more than three times as many supermarkets in wealthier neighborhoods compared with poorer areas.[24] In the United States, the number of supermarkets in low income neighborhoods is approximately 30% less than the number of stores in the highest-income neighborhoods.[57] Residents in low-income urban areas are often “forced to depend on small stores with limited selections of foods at substantially higher prices”.[28]
Research has found parallel trends between high rates of obesity and individuals of low SES and non-white ethnicity, particularly in the case of women. Research by Morland et al., found that areas with a majority of convenience stores have a higher prevalence of overweight and obese individuals, compared to areas with only supermarkets.[28] Fast food restaurants are disproportionately placed in low-income and minority neighborhoods, and are often the closest and cheapest food options. "People living in the poorest SES areas have 2.5 times the exposure to fast-food restaurants as those living in the wealthiest areas".[24] The lack of adequate food sources and limited transportation available to low-income communities are contributing factors to malnutrition among those living in low SES neighborhoods.[28]
Research has documented inequalities of access to supermarkets in urban city areas, and found a difference in access to supermarkets in poor vs non-poor areas. A study by Baker et al., found that mixed-race areas were significantly less likely to have access to foods that adhere to a healthful diet compared to predominantly white, high income areas.[4] Research by Mari Gallagher has found that African Americans are farther from healthful foods than other racial groups.[58][59][60] The availability of supermarkets in African American neighborhoods is 52% of their prevalence in white neighborhoods.[61] Moreover, Morland’s study of food-frequency data in the Atherosclerosis Risk in Communities (ARIC) study revealed that dominantly white populations had five times more supermarkets than neighborhoods with a dominantly non-white population. African Americans who lived in the same census tract with access to a supermarket were more likely to meet dietary guidelines for fruit and vegetable consumption. For each additional supermarket, an increase of 32% in fruit and vegetable intake was found.[62]
A 2010 study by Michael Correll published by the Duke Journal of Gender Law & Policy entitled “Getting Fat on Government Cheese: The Connection Between Social Welfare Participation, Gender and Obesity in America", analyzed data from the Centers for Disease Control and the U.S. Department of Health and Human Services to assess the health outcomes of women participating in the government Food Stamps and Temporary Aid to Needy Families programs. The study primarily examines and critiques the structure of current social welfare policies, but it also notes: 1) Many of the participants in the food stamps program live in “food deserts". Some 25% of food stamps participants do not have easy access to a supermarket; and 2) Under welfare-to-work reforms enacted in 1996, an adult recipient must have 30 hours a week of “work activity” to receive these benefits. Because many women are single with children and thus have limited time, this work obligation may limit their ability to travel to find nutritious foods, prepare healthful meals for themselves and their families, and exercise.[63]
Prevalence of obesity is generally higher in rural areas as compared to urban areas. Socioeconomic factors inhibit access to private cars as well as limited reliable public transportation. A 2005 study utilized geographic information systems (GIS) to determine food access in the most impoverished African American and White neighborhoods of Detroit, Michigan. The authors found that African American neighborhoods were an average of 1.1 miles farther from the nearest supermarket than the white neighborhoods, and that 28% of the residents in the most impoverished black neighborhoods did not own a car.[64]
African American communities have the least access to food with in food deserts. “Food access is particularly bad in African-American neighborhoods because of a lack of full-service supermarkets, whether independent or chain. Food access in Hispanic communities is generally better than in African-American neighborhoods due to the presence of independent and small chain supermarkets, but full-service chains are missing. Changes between 2005-2007, in general, have brought more discount stores, but few others, to African-American communities.” Hispanic communities within food deserts have targeted Hispanic food market.[65]
Research
Studies of urban and rural food environments reveal significant potential for evidence-based interventions and policies to combat the growing obesity epidemic, and to decrease some health disparities. Initial research on food deserts when the concept first appeared in the United Kingdom was narrowed to the impact of retail migration from the urban center.[4] More recent studies have explored the impact of food deserts in other geographic areas (e.g., rural and frontier), as well as among specific populations, such as minorities and elderly people. These studies address the relationship between the quality (access and availability) of retail food environments, pricing, and even obesity. The findings support that environmental factors essentially contribute to nearby people’s eating behaviors. Research conducted with variations in methods draws a more complete perspective of “multilevel influences of the retail food environment on eating behaviors (and risk of obesity).”[4]
In a small-sample research, which related fast food prevalence to the deal of food desserts, published in the Archives of Internal Medicine in 2011, 15 years of data from the study called Coronary Artery Risk Development in Young Adults (CARDIA) were used to concentrate on the fast-food consumption of more than 5,000 young American adults (aged 18–30 years) with vary geographic environments.[66] During the observed period, fast food chain, supermarket, or grocery store availability was treated as the parameter of fast food consumption, diet quality, and participants’ preferences to fresh fruits and vegetables. The key results of this longitudinal study include the following:
- Fast food consumption was directly related to the degree of proximity of fast food restaurants among low-income participants;
- For those restaurants were only within 1.00 to 2.99 km away home, approximately 1% increase in fast food supplies was correlated to a 0.13% and 0.34% increase in fast food consumption for the distance within 1 km and 3 km;[66]
- Supermarket and grocery store availability turned out to have no general correlation with diet quality and fresh food intake;
- Fast food access and individual consumption were not essentially related among the participated women of any income level;
- Overall, men had a higher frequency of fast food consumption than women.
Besides providing the evidence of how food resource availability affects diet, the study leads to a typical policy strategy to reduce food deserts, particularly for those low-income neighborhoods. That is, enhancing access to supermarkets while limiting the availability of fast food restaurants and small food stores. This is also the major objective of “widespread policy initiatives” regarding obesity across the United States in order to improve eating behavior and health among adults with different socioeconomic status.[66] The research team of this study concludes that their results implicate that “alternative policy options such as targeting specific foods or shifting food costs (subsidization or taxation)” may be complementarily necessary to promote healthy eating habits while increasing the access to large food stores in specific regions.[66]
A 2009 study of rural food deserts found a number of key differences in overall health, access to food, and the social environment of rural residents when compared to those who live in urban environments.[67] In terms of health, rural residents report overall poorer health and more physical limitations, with 12% of them rating their health as fair or poor, compared to 9% of urban residents[67] Communities that are smaller and isolated from urban influences have decreased access to the broader global market and consequently have fewer choices in food retailers. Lack of competition in the community not only restricts access to food resources, but can also result in higher food costs. The 57 recruited rural residents from Minnesota and Iowa in this study perceived that food quality and variety in their area were poor at times. They believed their current health conditions were shaped by their eating behaviors when the future chronic disease risk was affected by the history of dietary intake.[67] The researchers reached the conclusion that, for a community of people, while food choice which bound by family and household socioeconomic status remained as a personal challenge, social and physical environments played a significant role in stressing and shaping their dietary behaviors.[67]
However, the study of food deserts requires further research, including longitudinal studies of food environments, to support associations with obesity and to support neighborhood interventions. Longitudinal studies are critical in permitting the temporal outcomes of the correlation between food, nutrition status and obesity.[4] The determination of temporal associations guarantees credible historical data, including of those associated with life-course exposure, on different food and nutrition environments for future studies.[4] Future research is required to overcome the barriers facing residents of food deserts, including retail trends and location of supermarkets, in order that food retailers and city planners may develop multilevel interventions to address barriers to health at the individual and environmental level. Multilevel studies such as the two above examples that examine geographic differences in the access and availability of food, as well as nutritional quality of food, provide information for public health to explain disparities.
Other recent studies have shown some correlations between food availability and health, including a 2010 study that correlated distance from supermarkets with increases in body mass index.[68] The specific study suggests the associations between distance and decreased availability of healthy foods and increased risks of obesity. Among elderly people in particular, malnutrition caused by inadequate access to food can lead to other health risks. For those suffering from weight loss and undernutrition, risks include increased and longer hospitalizations, early admission to long term care facilities, and overall increased morbidity and mortality.[69] Nutritional disorders with co-morbidities are the ninth most frequent diagnostic category among hospitalized rural elderly Medicare beneficiaries. Elderly adults struggling with obesity and overnutrition related to limited food choices are at risk of exacerbating existing chronic conditions, such as heart disease and diabetes, and increased functional decline.[69][70]
Food desert issues by region
Food deserts can be found in many countries around the world, even more wealthy countries such as the United States, Canada, the United Kingdom, New Zealand, and Australia.[71]
The research available on food deserts worldwide is not as richly documented as it is in United States. “Food deserts exist, at least in the United States. Evidence is both abundant and robust enough for us to conclude that Americans living in low income and minority areas tend to have poor access to healthy food. However, Studies on the price of food were generally of low-quality, and their findings were mixed. Evidence from other countries is sparse and equivocal. The evidence that is available is much less compelling than evidence from the United States. On this basis, evidence from other countries does not warrant firm conclusions at this time on whether access to healthy, affordable food systematically varies to disadvantaged so socioeconomically deprived ares.” Beaulac, Julie, Elizabeth Kristjansson PhD, and Steven Cummins PhD.[72] This publication concluded that there is just not enough documented information to support that this is a worldwide problem, not saying that it is not a problem, but there is not enough concrete information to base a claim.
Europe
“European (non-UK) food access research also frequently highlights the problem of poverty in relation to accessing a healthy diet.” French researches have noted that lower income consumers have a tendency to reach for more affordable items such as high caloric foods, (i.e. cereals, sweets, and added fats) instead of nutrient rich single source foods.[73]
United Kingdom
British food deserts can be broadly classified into twelve geographical types, based on the interaction of socioeconomic factors of physical access to shops, financial access (affordability of) healthy food, and attitudes towards consumption of healthy food, the desire to consume it rather than fast / convenience food, possession of cooking skills, that is, psychological access. These twelve neighbourhood types are 1) inner city executive flat areas (too fast lifestyle to cook healthily), 2) inner city ethnic minority areas (cost of food vs low wages), 3) inner city deprived areas severed by main roads from retail areas (poor physical access), 4) declining suburban areas (shops closing, poor physical access to supermarkets), 5) planned local authority housing areas (low income, and shops often lack fresh produce), 6) student residence areas (preference for fast food outlets, little demand for fresh produce), 7) Wealthy suburban areas, most shop by car, but some less mobile pensioners with no car. Areas 8 - 12 are rural food deserts. 8) is small market town centres losing trade to out-of-town supermarkets, leaving the car-less without easy access, 9) market town suburbs, poor bus service to centre perhaps 1 or 2 miles (2 - 3 kilometres) distant, 10), smaller rural towns, lack full range of fresh produce, 11) remoter villages, no shop, and under-served by mobile shops, 12) dispersed settlements, no focal point for shop [74]
Furey et al. describes food desert creation as arising where “high competition from large chain supermarkets has created a void”.[75]
Australia
“In Melbourne, households with lower individual socio-economic position and area disadvantages have restricted access to food because of lack of money and /or having physical limitations due difficulty lifting or lack of access to a car for food shopping.” Households where the head of the house was not born in Australia had less access to food, reduced access to transportation or finances. [71]
In Western Australia, a private/public partnership between government and non-governmental entities set out to increase fruit and vegetable consumption in children. The partnership developed policies to improve school lunch nutrition, restrict food advertising targeting children, and support mass media efforts which promote fruit and vegetable consumption. 2 years after implementing these policies Western Australian schools increased their sale of healthy foods.[76]
Africa
Definition
African food deserts deviate from the commonly held definitions and assumptions of North American and European food deserts. In particular, African food deserts are not inscribed in stereotypical structure and organization of food deserts in the Western world. African food deserts are more complex and multifaceted due to accelerated urbanization, the various ways individuals acquire food through formal and informal food economy markets, familial dynamics of the household, and African social, political and economic effects.[77] As defined by Battersby and Crush (2013), “African food deserts are defined as poor, often informal, urban neighborhoods characterized by high food insecurity and low dietary diversity, with multiple markets and market and non-market food sources but variable household access to food.”[77]
General presumptions of food deserts often pertain to the distance between where an individual lives and the nearest supermarket. In Western nations, supermarkets prevail over traders and vendors but food sourcing methods within Africa are reversed. Certain regions have more fluidity to food resource allocation in an informal economy where traders and vendors are available within the areas they live and other local areas.[77] Urban agriculture also plays a big role within Africa as pastoralism is widely practiced as populations raise their own livestock and grow their own food creating informal rural-urban food transfer systems. These food sourcing practices vary in regions throughout Africa based on geography, local history, etc., but a study by Pendleton et al. (2012) shows with statistical analysis that local trade vending and pastoralism does not increase food security in Africa’s neighborhoods but rather limits resources available to the entire community thus creating a food desert.[78] Low-income populations are still more inclined to source food in the ways discussed but supermarket growth in Africa, in both urban and rural areas, is cutting off these common food sourcing methods leading to worsening food security levels.[79]
In accordance with this, households within the same food desert environments source food differently based on a differentiation of household variables.[77] Neighborhoods in Africa are not as segregated by income levels as in the West. Most neighborhoods have a high mix of various income levels, thus some households are more food insecure than others due to mobility and other economic reasons. Those with higher incomes are more likely to shop at the nearest grocery store due to having better access to transportation. Lower income households tend to stick to sourcing food from local vendors or through pastoralism which is not as stable as sourcing it from supermarkets due to vendors operating only at minimal, specific times and supermarket growth overtaking farming lands.[79] Furthermore, gender roles play an important role in African food deserts as there is greater access to food in households headed by a man than a woman.[77] This is due to various socio-political effects in Africa towards women that do not affect modern, Western women who have more access to financial opportunities. In Africa, women are two times more likely to be more food insecure compared to men if they are heads of the household. Women have less mobility within Africa and thus will have to rely more on the insecure food sourcing practices.
Differences in Measuring Food Deserts
Food deserts in Africa are measured in different ways than they are in western countries. In Africa, food deserts are not signified by a lack of supermarkets in poorer areas due to the fact that Africans also utilize informal food sources such as traders or vendors. In a study done by the African Food Security Urban Network (AFSUN), it was found that nearly 70% of poor African households in urban areas sourced part of their food needs from vendors and traders, while 79% of these households utilized a supermarket. When these studies took frequency into account, it was found that poor Africans use informal vendors more often for most of their needs, and only go to supermarkets to buy large quantities of a staple.[77]
A difference also arises in the measurement of distance due to the fact that African cities suffer from a large degree of fragmentation which leads to the poor having to utilize public transportation to travel large distances, spending up to 3 hours a day in transit. With much of the day wasted in transit, poor Africans have less time to spend on shopping or preparing food which forces them to buy more expensive, less nutritious, already prepared foods from either street vendors or restaurants.[79] This fragmentation and mobility also leads to many poor Africans shopping for groceries in places outside their township. A study in Soweto, Johannesburg in 2004 showed most urban poor spend about 50% of their expenses in places outside of the towns in which they reside.[77]
The variety of factors affecting the levels of food insecurity make it difficult to apply the western concept of food deserts to this problem of food access in Africa. Different households within the same cities in Africa, face differing levels of food insecurity, because, as the AFSUN survey results indicate, there are a wide variety of factors, such as gender, income, and education that affect access to nutritious food.[77]
Impacts
Africa is one of the fastest urbanizing regions in the world, but as the urban population is growing, so is the population without reliable access to a healthy and varied diet. However, the predominant understanding of an urban food desert and proposed solutions are still shaped largely by characteristics of food insecurity in rural regions, and a greater emphasis is placed on rural food insecurity. A survey of databases conducted by Battersby in early 2011 revealed that the keywords “NOT rural,” reduced the number of results returned for database CSA Illumina from 361 to 114. Furthermore, South African policy papers categorize food insecurity under Rural Development.[79]
The 1995 Income and Expenditure Survey conducted in South Africa assessed an urban food insecurity rate of 27 percent, relative to the rural rate of 62 percent.[80] Later studies such as the National Food Consumption Survey of 1999[81] and South African Social Attitudes Survey of 2008 also independently assessed the urban food insecurity rate to be roughly half of that of the rural rate.[82]
However, a food insecurity survey conducted in 2000 on the rural Eastern Cape, rural Western Cape, and urban Cape Town assessed food insecurity to be 83, 69, and 81 percent, respectively. Instead of using the rural understanding of a food desert, which is usually associated with the distribution of market retailers such as supermarkets, this survey took into account various other urban African factors and went beyond what Battersby calls “the simple rural:urban binary.” Such factors include the tendency of residents to utilize formal food sources over informal sources such as agriculture and local markets.[79]
As compared to the West, Africa is undergoing rapid economic and urban development which contributes to growth that undercuts the food sourcing mechanisms already in place. Many regions in Africa grow their own food, rely on starch staples, and regularly use food vendors and traders in their areas of residence. With African economic growth contributing to the building of supermarkets and other urban renewal practices, it takes land space away from pastoral communities that grow and harvest their own food and reduces the resources vendors use to attain the products they sell, limiting their business practices and giving rise to food deserts in Africa.[79] Modern African food systems in towns and cities are coming about rapidly changing and destabilizing the already high food insecurity practices already in place. A revised definition of food deserts in Africa that reflects the challenges of this rapid urbanization would prove useful for researchers and policymakers alike.[77]
North America
United States
.jpg)
Maps, showing the distribution of food deserts in the United States can be found in Morton and Blanchard's 2007 article.[8]
Despite differences in terminology, most research in the United States supports the hypothesis that on the neighborhood level, there are disparities in the retail food environment.[4]
In the interest of profitability, larger supermarkets have followed this trend and are most prevalent in these white suburban neighborhoods.[28]
According to a report to Congress prepared by the U.S. Department of Agriculture, assessing the extent of limited access to affordable, nutritious food, approximately 2.4 million households in the United States are more than a mile from a supermarket and lack access to a vehicle.[38]
Barriers and proposed solutions
Access is not the only determinant to healthful eating. There are many environmental determinants that predict a positive outcome in healthful eating for residents of current food desert areas, such as transportation, culture, social capital, and food price. A criticism of current research on food access and obesity assumes a “simplistic deprivation effect associated with poor-quality food environments".[4]
Audit research suggests that supermarkets are the most effective way to supply communities with a wide selection of fresh and relatively affordable healthful food. Moreover, supermarkets typically are open year-round, provide convenient hours of operation, and generally accept Electronic Benefit Transfer (EBT).[83] As a result, many programs focus on increasing incentives for supermarkets to operate in these underserved areas. Some incentives include property or sales tax breaks. Community-level interventions that focus on getting healthful food to low-income areas through farmers markets, mobile carts or community gardens.[38]
One community intervention that increases food access is the community garden. Community gardens enable individuals to grow their own food on a designated area of land that is shared with other community members. Community garden programs increased access to affordable, nutritious food in rural, suburban and urban areas. They also help strengthen community and social support for participants.[84]
The USDA released an extensive report to Congress in 2009 as a request to reform the Food, Conservation, and Energy Act of 2008. The study outlines a list of recommendations for addressing access issues in food deserts that include the above options, but also includes transportation reform as a solution.[38] Transportation is a significant barrier in rural food deserts (rural realities). Evaluating current transportation in these communities and developing community-specific solutions can target populations limited by current transportation options (rural realities). According to Morton and Blanchard, there is a need to address the added complications of individuals living in these isolated communities. Proposed solutions include utilizing a combination of public and private resources. Current transit assistance and meal-provisioning programs that are already established in many communities, such Meals on Wheels, have initiatives that focus on providing food residents with limited mobility and ability to shop at traditional food retailers.[85]
In early 2010 the Obama administration unveiled the Healthy Food Financing Initiative (HFFI) that will promote a range of interventions that expand access to nutritious foods, including developing and equipping grocery stores and other small businesses and retailers selling healthful food in communities that currently lack these options. The initiative provided more than $400 million in funding intended to bring grocery stores and healthful food retailers to low-income rural and urban communities. This effort is in concert with Michelle Obama’s “Let’s Move” campaign to counter childhood obesity. The initiative receives funding from the Treasury Department, Department of Agriculture and Department of Health and Human Services.[86]
Several states and cities within the United States are also implementing comprehensive programs that involve public-private partnership and a combination of financing initiatives and community-level interventions.[38] The Pennsylvania Fresh Food Financing Initiative, for example is a public-private partnership aimed at encouraging the development of new supermarkets by providing grants of up to $250,000 or loans of up to $2.5 million per store to defray the infrastructure costs of developing a new store. So far, $41.8 million in grants and loans have funded 58 stores.[38]
The New York City FRESH program (Food Retail Expansion Health) is one of the most comprehensive attempts to increase access to full-service grocery stores in underserved areas. They offer an abatement of land or building taxes for a period of 25 years and a sales tax exemption on building materials.[61]
Community-level interventions are useful in that they are less expensive and easier to implement than programs that encourage the creation of new stores. They require less space, promote local farmers and increase community and social capital.
Citizens of a rural community in North Carolina collaborated to develop and implement a solution to the problem of access to food in Bertie County, the poorest in the state.[87] Community members, in conjunction with a class at the public high school, designed and constructed a pavilion to serve as the home for a local farmers’ market. This is one example of committed civic engagement, which can be a strong determinant in the successful development of community-specific solutions and improved access to food. Community involvement and the incorporation of local organizations and volunteerism can improve the effectiveness of food safety nets and alternative solutions such as community gardens.[67]
Universities have coordinated with local business and community leaders to solve food scarcity issues. In 2008, La Salle University and The Fresh Grocer teamed up to open a grocery store in Germantown, Philadelphia. The Germantown neighborhood was plagued with a decades-long food desert, but thanks to a coordination between two enterprises, the Fresh Grocer was able to provide more than 250 jobs to Philadelphians and provide healthy food.[88][89] College students have also started their own community gardens to assist the underprivileged members of their neighborhood.
Farmers markets can be costly for low-income individuals living in these communities.[61] The City of New York has implemented several community-level initiatives such as increasing the number farmers markets in underserved areas and increasing their use by residents through the Health Bucks program. This program offers $2 coupons purchasing fresh fruits and vegetables at participating farmers markets. This program was intended to reduce barriers to access based on affordability. Through this program, EBT sales at farmers’ markets more than doubled from $40,000 in 2007 to over $89,000 in 2008. The program is being expanded into upstate New York as the Fresh Bucks program.[90]
Another proposed solution involves increased local food production and distribution in urban centers. The New York City Regional Foodshed is an initiative examining the local food production capacity of the New York City Metropolitan Region.[91]
In response to the lack of healthy food access, the Westwood community in Denver, CO partnered with the non-profit Re:Vision to create a system of community gardens in 2010. As of 2015, they have plans to expand the initiative and open a food cooperative in the neighborhood.[92]
State and federal agencies in New York are working together to create a program that allows EBT users the option to purchase healthful foods online and have them delivered to their homes. In the fall of 2016 a pilot program was launched in conjunction with an established food delivery company, FreshDirect. This pilot allows two zip codes in the Bronx to have access to the services provided by FreshDirect and the option to pay by EBT. The advancements being made by the USDA to enhance access to fresh local foods could eliminate the existence of food deserts in areas that gain access to this food delivery model.[93]
In addition to government and community programs, families have been known to work together and pool their resources in order to survive. It is not uncommon for families to develop a "network" of sharing,[94] bartering their goods and services. They exchange clothing, provide childcare, sell personal possessions, share transportation resources and in extreme cases share housing. People living in food deserts see this as survival techniques, they are creating ways to feed their families.[95][96]
Mexico
Food Resources
Approximately 25 to 35 percent of nine Mexican states are classified under Serious Food Insecurity, with their numbers accenting the statistic that of the population of Mexico citizens, spanning across all states, lacking adequate access to food is at least ten percent. Between the years of 2003 and 2005, the total supply of food into the nation is actually sufficient to feed the entire nation with an average of 3,270 kilocalories per daily capita. This caloric sustenance is in surplus of the 1,850 kilocalorie minimum requirement.[97]
A large portion of Mexico’s population relies on agriculture for food. However, the government’s attempts to balance subsidies (which encourage farmers to grow more crops) while trying to keep food prices low can complicate the process of obtaining locally grown foods. Recently, decreased government support of agriculture has crippled maize farmers’ ability to produce enough food to feed the population. In addition, Mexico is vulnerable to drought which can further cripple agriculture.[98] This decreases access to local foods and forces people to look to grocery stores for cheap alternatives.
Diet Trends
Due to the rather rapid changes of Latin American diets switching from complex carbohydrates and fresh fruits and vegetables to saturated fat and starches, obesity and chronic disease persist alongside undernutrition. Both rural and urban areas are equally affected, as the rural areas see children suffering from nutritional deficits while the increase in refined foods and increasingly sedentary lifestyles of the city lead to chronic disease and obesity. More specifically, energy in Latin America is now tending to come from sugars instead of legumes, as well as an increase in more refined foods and less complex carbohydrates. This is a result of globalization as nations tend to rely on highly processed foods instead of local producers. Additionally, in Mexico, animal proteins have been replacing vegetable proteins, with increase in prevalence by 50% from the 1960s to the 1990s. The total cholesterol availability in Mexico surpasses the US guidelines for daily intake, at over 300 mg per day, a result of the increased availability of saturated fats.[99]
RURAL DIETS:
Rural diets consist mainly of vegetables and very little animal or saturated fats, though rural Mexican populations have shown a decrease in their fruit and vegetable intake beginning in the 1980s.[99] Urbanization usually entailed abandoning traditional foods and adopting Western, highly processed diets. The two diets contrast due to the low levels of sugar in the rural diet as well as healthier preservation methods and high fiber content. In Northern Mexico, rural populations who transitioned from their traditional diets to more processed diets now suffer from a dramatic increase in obesity and diabetes.[100]
URBAN DIETS:
Those who migrate to cities and have increased incomes become more sedentary and have easier access to fast food and supermarkets, which are taking over distribution in urban areas and pushing out smaller markets. Due to globalization, the Latin American markets have been overtaken by transnational food corporations and are losing local distributors. More affluent households tend to buy more meat and less oils and grains, while the poorer urban households are able to purchase foods that exceed their energy needs but are lacking in essential vitamins, such as vitamins A and C, as well as iron, zinc and folate.[100] In a survey conducted on 650 urban school lunches, none of them were found to be healthy and only one percent were found to be adequate.[101]
Obesity
Because of the lack of access to foods that contain the necessary nutrients and an increasing demand of labor due to globalization, many from Mexico’s working class are forced to adopt a diet that presents negative health impacts. In a survey conducted by National Health Survey in 2000, it was found that the prevalence of obesity in the sample population was 67% in women and 61% in men. A similar survey in 2003 targeting obesity from rural, low-income communities showed that around 60% of women and 50% of men were considered either overweight or obese with respect to the Body Mass Index.[102]
Economically, the rising obesity rate in Mexico is also taking a toll on its health care system. According to a study published by Cambridge University Press, cost of treatment for obesity related diseases is projected to grow from an estimated $806 million in 2010 to $1.2 billion in 2030 and $1.7 billion in 2050. Recent efforts have been made by the Mexican government to address the issue of obesity as a reduction of 1% in mean BMI would reduce the cost by $43 million in 2030 and $85 million in 2050 respectively. Through initiatives that focus on the narrative of a healthier lifestyle, the government aims to reduce the projected obesity prevalence. However, not much is known about the effectiveness of those programs and their relationships to the reduction to food deserts.[103]
For more information, see Obesity in Mexico.
Beyond physical access
A pilot study conducted by Cummins et al. has shown that access to food options is not the only barrier to healthier diets and improved health outcomes. Their study focused on a community that had been funded by the Pennsylvania Fresh Food Financing Initiative. They conducted follow up after a grocery store was built in a food desert to assess the impact. They found that “simply building new food retail stores may not be sufficient to promote behavior change related to diet.”[104] Pearson et al. have also found that physical access is not the sole determinant of fruit and vegetable consumption and urge food policy to focus on the social and cultural barriers to healthy eating.[105]
Wrigley et al. collected data before and after a food desert intervention to explore factors affecting supermarket choice and perceptions regarding healthy diet, in Leeds, United Kingdom. Pre-tests were administered prior to a new store opening and post-tests were delivered 2 years after the new store had opened. The results showed that nearly half of the food desert residents began shopping at the newly built store, however, only modest improvements in diet were recorded.[106][107] Other studies have documented a sense of loyalty towards the owners of neighborhood convenience stores as an explanation as to why residents may not change their shopping behaviors.[6]
It is important to note, this demographic is mostly nonstandard workers. “Nonstandard work arrangements are nonstandard schedules such as work hours that fall outside “typical business hours (i.e. the nine-to-five day), including rotating shifts and night or evening shifts.” In this situation it makes it harder for people working these hours to make it to a traditional grocery store, especially smaller stores that typically close earlier. Therefore, it illustrates how this problem continues to evolve. It inevitably sends this demographic in search of other alternatives such as fast food or convenience stores, that are generally open later.[108]
There are safety concerns for residents of food deserts. Many food deserts are in high crime area, with bulletproof glass or bars on the windows, not a comfortable shopping environment. “For example, residents mentioned the environment inside store, poor upkeep and customer service, as well as issues outside the store such as community violence and proximity to liquor stores.” The neighborhoods have higher rates of community violence, with most having a lack of transportation. These residents will also have to walk these streets caring their food or taking a bus, and maybe also being responsible for a child or children.[65]
See also
- Agroecology
- Banking desert
- Book desert
- Food desert in West Oakland
- Food Empowerment Project
- Food safety
- Food security
References
- ↑ USDA Defines Food Deserts | American Nutrition Association
- 1 2 3 Story, Mary; Kaphingst, Karen M.; Robinson-o'Brien, Ramona; Glanz, Karen (2008). "Creating Healthy Food and Eating Environments: Policy and Environmental Approaches". Annual Review of Public Health. 29: 253–72. doi:10.1146/annurev.publhealth.29.020907.090926. PMID 18031223.
- ↑ http://www.nytimes.com/2012/04/18/health/research/pairing-of-food-deserts-and-obesity-challenged-in-studies.html[]
- 1 2 3 4 5 6 7 8 Ford, Paula B; Dzewaltowski, David A (2008). "Disparities in obesity prevalence due to variation in the retail food environment: Three testable hypotheses". Nutrition Reviews. 66 (4): 216–28. doi:10.1111/j.1753-4887.2008.00026.x. PMID 18366535.
- ↑ Eisenhauer, Elizabeth (2001). "In poor health: Supermarket redlining and urban nutrition". GeoJournal. 53 (2): 125–33. doi:10.1023/A:1015772503007.
- 1 2 3 4 5 Walker, Renee E.; Keane, Christopher R.; Burke, Jessica G. (2010). "Disparities and access to healthy food in the United States: A review of food deserts literature". Health & Place. 16 (5): 876–84. doi:10.1016/j.healthplace.2010.04.013.
- ↑ USDA ERS - Go to the Atlas. From: http://www.ers.usda.gov/data-products/food-access-research-atlas/go-to-the-atlas.aspx
- 1 2 3 Morton, Lois Wright; Blanchard, Troy C. (2007). "Starved for access: life in rural America's food deserts" (PDF). Rural Realities. Rural Sociological Society. 1 (4): 1–10.
- ↑ Reisig, V.; Hobbiss, A. (2000). "Food deserts and how to tackle them: A study of one city's approach". Health Education Journal. 59 (2): 137–49. doi:10.1177/001789690005900203.
- 1 2 Cummins, S.; MacIntyre, S (2002). "'Food deserts'—evidence and assumption in health policy making". BMJ. 325 (7361): 436–8. doi:10.1136/bmj.325.7361.436. PMC 1123946
 . PMID 12193363.
. PMID 12193363. - 1 2 Hendrickson, Deja; Smith, Chery; Eikenberry, Nicole (2006). "Fruit and vegetable access in four low-income food deserts communities in Minnesota". Agriculture and Human Values. 23 (3): 371–83. doi:10.1007/s10460-006-9002-8.
- ↑ Larsen, Kristian; Gilliland, Jason (2009). "A farmers' market in a food desert: Evaluating impacts on the price and availability of healthy food". Health & Place. 15 (4): 1158–62. doi:10.1016/j.healthplace.2009.06.007.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 "Access to Affordable and Nutritious Food: Measuring and Understanding Food Deserts and Their Consequences" (PDF). United States Department of Agriculture Economic Research Service. Jun 2009. Retrieved 13 Nov 2016.
- ↑ Liese, Angela D.; Hibbert, James D.; Ma, Xiaoguang; Bell, Bethany A.; Battersby, Sarah E. (2014). "Where Are the Food Deserts? An Evaluation of Policy-Relevant Measures of Community Food Access in South Carolina". Journal of Hunger & Environmental Nutrition. 9: 16–32. doi:10.1080/19320248.2013.873009.
- 1 2 "Measuring the Food Environment in Canada". Food and Nutrition. Health Canada. 11 Oct 2013. Retrieved 13 Nov 2016.
- 1 2 3 "Go to the Atlas". Food Access Research Atlas. United States Department of Agriculture Economic Research Service. 19 Oct 2016. Retrieved 13 Nov 2016.
- 1 2 3 Ver Ploeg, M.; Dutko, P.; Breneman, V. (2014). "Measuring Food Access and Food Deserts for Policy Purposes". Applied Economic Perspectives and Policy. 37 (2): 205–25. doi:10.1093/aepp/ppu035.
- ↑ Ploeg, Michele. "Access to Affordable and Nutritious Food: Updated Estimates of Distance to Supermarkets Using 2010 Data" (PDF). A Report from the Economic Research Service. United States Department of Agriculture Economic Research Service.
- ↑ Food, Conservation, and Energy Act of 2008, 110th Cong, 2nd Sess, HR 6124, Title VII. Access 10 Nov.2016. Available at: http://www.gpo.gov/fdsys/pkg/BILLS-110hr6124eh/pdf/BILLS-110hr6124eh.pdf
- 1 2 Access to affordable and nutritious food: Measuring and understanding food deserts and their consequences: Report to Congress. Washington, D.C.: U.S. Dept. of Agriculture, Economic Research Service. Jun 2009. Web. 10 Nov 2016.
- 1 2 Jiao, Junfeng; Moudon, Anne V.; Ulmer, Jared; Hurvitz, Philip M.; Drewnowski, Adam (2012). "How to Identify Food Deserts: Measuring Physical and Economic Access to Supermarkets in King County, Washington". American Journal of Public Health. 102 (10): e32–9. doi:10.2105/AJPH.2012.300675. PMC 3490650. PMID 22897554.
- ↑ Dubowitz, Tamara; Zenk, Shannon N.; Ghosh-Dastidar, Bonnie; Cohen, Deborah A.; Beckman, Robin; Hunter, Gerald; Steiner, Elizabeth D.; Collins, Rebecca L. (August 2015). "Healthy food access for urban food desert residents: examination of the food environment, food purchasing practices, diet and BMI". Public Health Nutrition. 18 (12): 2220–2230. doi:10.1017/s1368980014002742.
- 1 2 Beck, C. (2009) Food Access in Colorado, Colorado Health Foundation.
- 1 2 3 Ming-Chen Yeh and David L. Katz. "Food, Nutrition, and the Health of Urban Populations". In Cities and the Health of the Public (Nicholas Freudenberg, Sandro Galea, and David Vlahov, eds.). Vanderbilt University Press (2006), pp. 106-127. ISBN 0-8265-1512-6.
- ↑ Bauer, K. W. (2004, January 201). Price and Availability Matter. From The New York Times: http://www.nytimes.com/roomfordebate/2011/01/23/can-wal-mart-make-us-healthier/access-to-healthy-foods-and-lower-prices-matter
- ↑ Winne, M. (2008). Closing the Food Gap: Resetting the Table in the Land of Plenty. Beacon Press.
- ↑ Monsivais, Pablo; Drewnowski, Adam (2007). "The Rising Cost of Low-Energy-Density Foods". Journal of the American Dietetic Association. 107 (12): 2071–6. doi:10.1016/j.jada.2007.09.009. PMID 18060892.
- 1 2 3 4 5 Morland, Kimberly; Wing, Steve; Diez Roux, Ana; Poole, Charles (2002). "Neighborhood characteristics associated with the location of food stores and food service places". American Journal of Preventive Medicine. 22 (1): 23–9. doi:10.1016/s0749-3797(01)00403-2. PMID 11777675.
- ↑ Brownell, Kelly (2004). "Fast Food and Obesity in Children". Pediatrics. 113: 132 – via EBSCOhost.
- ↑ Sathyanarayana Rao, TS; Asha, MR; Ramesh, BN; Jagannatha Rao, KS (2008). "Understanding nutrition, depression and mental illnesses". Indian Journal of Psychiatry. 50 (2): 77–82. doi:10.4103/0019-5545.42391. PMC 2738337. PMID 19742217.
- 1 2 "USDA Defines Food Deserts | American Nutrition Association". americannutritionassociation.org. Retrieved 2016-11-08.
- 1 2 3 Treuhaft, Sarah; Karpyn, Allison (2010). "The Grocery Gap" (PDF). PolicyLink.
- 1 2 United States Department of Agriculture-Economic Research Service. Food Access Research Atlas (formerly known as the Food desert locator). Available at: http://www.ers.usda.gov/data-products/food-access-research-atlas.aspx.
- 1 2 United States Department of Agriculture-Economic Research Service. Rural income, poverty, and welfare report. Available at: http://www.ers.usda.gov/topics/rural-economy-population/rural-poverty-well-being.aspx.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 "Food Deserts | Food Empowerment Project". www.foodispower.org. Retrieved 2016-11-08.
- ↑ "National Poverty Center | University of Michigan". www.npc.umich.edu. Retrieved 2016-11-08.
- 1 2 3 4 5 6 "Choices Magazine Online". www.choicesmagazine.org. Retrieved 2016-11-09.
- 1 2 3 4 5 6 Ver Ploeg, Michele (June 2009). Access to Affordable and Nutritious Food—Measuring and Understanding Food Deserts and Their Consequences: Report to Congress. USDA. ISBN 978-1-4379-2134-2.
- 1 2 Haider, Steven J.; Bitler, Marianne (March 2009). An Economic View of Food Deserts in the United States (PDF). Understanding the Economic Concepts and Characteristics of Food Access. National Poverty Center.
- ↑ Rural Assistance Center. (2011). "Aging".
- ↑ CensusScope. (2011). [Map illustration of percentage of Americans 65+]. Demographic Maps: An Aging Population. Retrieved from http://www.censusscope.org/us/map_65plus.html
- ↑ Sharkey, Joseph R; Johnson, Cassandra M; Dean, Wesley R (2010). "Food Access and Perceptions of the Community and Household Food Environment as Correlates of Fruit and Vegetable Intake among Rural Seniors". BMC Geriatrics. 10. doi:10.1186/1471-2318-10-32.
- ↑ Hartman, Rebecca. "Elder Health in Rural America". National Rural Health Association.
- ↑ DeGood, Kevin. "Fixing the Mobility Crisis Threatening the Baby Boom Generation" (PDF). Transportation for America.
- 1 2 Quandt, S. A.; McDonald, J; Arcury, T. A.; Bell, R. A.; Vitolins, M. Z. (2000). "Nutritional self-management of elderly widows in ruralcommunities". The Gerontologist. 40 (1): 86–96. doi:10.1093/geront/40.1.86. PMID 10750316.
- ↑ "Improve Access to Nutritious Food in Rural Areas". www.sog.unc.edu. Retrieved 2016-11-12.
- 1 2 Fitzpatrick, Katie; Greenhalgh-Stanley, Nadia; Ver Ploeg, Michele (2016). "The Impact of Food Deserts on Food Insufficiency and SNAP Participation among the Elderly". American Journal of Agricultural Economics. 98: 19–40. doi:10.1093/ajae/aav044.
- ↑ Bitto, Ella Annette; Morton, Lois Wright; Oakland, Mary Jan; Sand, Mary (2003). "Grocery Store Acess Patterns in Rural Food Deserts". Journal for the Study of Food and Society. 6 (2): 35–48. doi:10.2752/152897903786769616.
- ↑ "Summary Health Statistics: National Health Interview Survey 2014" (PDF). Center for Disease Control and Prevention. National Center for Health Statistics. 2014. Retrieved Nov 11, 2016.
- ↑ Aldrich, Nancy. "CDC Promotes Public Health Approach To Address Depression among Older Adults" (PDF). CDC. US Department of Health and Human Services. Retrieved Nov 11, 2016.
- ↑ Vafaei, Z; Mokhtari, H; Sadooghi, Z; Meamar, R; Chitsaz, A; Moeini, M (2013). "Malnutrition is associated with depression in rural elderly population". Journal of research in medical sciences. 18 (Suppl 1): S15–9. PMC 3743311. PMID 23961277.
- ↑ Marshall, T. A.; Stumbo, P. J.; Warren, J. J.; Xie, X. J. (2001). "Inadequate nutrient intakes are common and are associated with low diet variety in rural, community-dwelling elderly". The Journal of nutrition. 131 (8): 2192–6. PMID 11481416.
- ↑ Institute of Medicine (US) Food Forum. Providing Healthy and Safe Foods As We Age: Workshop Summary. Washington (DC): National Academies Press (US); 2010. 5, Nutrition Concerns for Aging Populations. Available from: https://www.ncbi.nlm.nih.gov/books/NBK51837/
- ↑ Nicklett, Emily J.; Kadell, Andria R. (2013). "Fruit and vegetable intake among older adults: A scoping review". Maturitas. 75 (4): 305–12. doi:10.1016/j.maturitas.2013.05.005. PMC 3713183. PMID 23769545.
- ↑ Palmer, A.M. (2011). "Community Food Assessment in an Urban Food Desert". Journal of the Academy of Nutrition and Dietics.
- ↑ Cannuscio, Carolyn C.; Weiss, Eve E.; Asch, David A. (2010). "The Contribution of Urban Foodways to Health Disparities". Journal of Urban Health. 87 (3): 381–93. doi:10.1007/s11524-010-9441-9. PMC 2871079. PMID 20354910.
- ↑ Chung, Chanjin; Myers, Samuel L. (1999). "Do the Poor Pay More for Food? An Analysis of Grocery Store Availability and Food Price Disparities". Journal of Consumer Affairs. 33 (2): 276–96. doi:10.1111/j.1745-6606.1999.tb00071.x. JSTOR 23859959. SSRN 2026583.
- ↑ Examining the Impact of Food Deserts on Public Health in Chicago, Mari Gallagher Research & Consulting Group, 2006. Retrieved from http://www.marigallagher.com/projects/4/
- ↑ Examining the Impact of Food Deserts on Public Health in Detroit, Mari Gallagher Research & Consulting Group, 2007. Retrieved from http://www.marigallagher.com/projects/2/
- ↑ Women and Children Last (In the Food Desert), Mari Gallagher Research & Consulting Group, 2007
- 1 2 3 Leone, A. F.; Rigby, S; Betterley, C; Park, S; Kurtz, H; Johnson, M. A.; Lee, J. S. (2011). "Store type and demographic influence on the availability and price of healthful foods, Leon County, Florida, 2008". Preventing chronic disease. 8 (6): A140. PMC 3221579. PMID 22005633.
- ↑ Morland, Kimberly; Diez Roux, Ana V.; Wing, Steve (2006). "Supermarkets, Other Food Stores, and Obesity". American Journal of Preventive Medicine. 30 (4): 333–9. doi:10.1016/j.amepre.2005.11.003. PMID 16530621.
- ↑ Correll, Michael (2010). "Getting Fat on Government Cheese: The Connection Between Social Welfare Participation, Gender, and Obesity in America". Duke Journal of Gender Law & Policy. 18: 45–77. SSRN 1921920.
- ↑ Zenk, Shannon N.; Schulz, Amy J.; Israel, Barbara A.; James, Sherman A.; Bao, Shuming; Wilson, Mark L. (2005). "Neighborhood Racial Composition, Neighborhood Poverty, and the Spatial Accessibility of Supermarkets in Metropolitan Detroit". American Journal of Public Health. 95 (4): 660–7. doi:10.2105/AJPH.2004.042150. PMC 1449238. PMID 15798127.
- 1 2 "Food Deserts in Chicago" (PDF). October 2011.
- 1 2 3 4 Boone-Heinonen, Janne; Gordon-Larsen, P; Kiefe, C. I.; Shikany, J. M.; Lewis, C. E.; Popkin, B. M. (2011). "Fast Food Restaurants and Food Stores". Archives of Internal Medicine. 171 (13): 1162–70. doi:10.1001/archinternmed.2011.283. PMC 3178268. PMID 21747011.
- 1 2 3 4 5 Smith, Chery; Morton, Lois W. (2009). "Rural Food Deserts: Low-income Perspectives on Food Access in Minnesota and Iowa". Journal of Nutrition Education and Behavior. 41 (3): 176–87. doi:10.1016/j.jneb.2008.06.008. PMID 19411051.
- ↑ "Review: Research on Availability of Healthy Food in Food Deserts. Web-based document at DataHaven with summary of numerous recent studies on food desert impacts on health.". DataHaven. 2011-01-31. Retrieved 2011-02-01.
- 1 2 Thompson Martin, C.; Kayser-Jones, J.; Stotts, N.; Porter, C.; Froelicher, E. S. (2006). "Nutritional Risk and Low Weight in Community-Living Older Adults: A Review of the Literature (1995-2005)". The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 61 (9): 927–34. doi:10.1093/gerona/61.9.927.
- ↑ Jensen, Gordon L.; Friedmann, Janet M. (2002). "Obesity is Associated with Functional Decline in Community-Dwelling Rural Older Persons". Journal of the American Geriatrics Society. 50 (5): 918–23. doi:10.1046/j.1532-5415.2002.50220.x. PMID 12028181.
- 1 2 Burns, Cate; Bentley, Rebecca; Thornton, Lukar; Kavanagh, Anne (2011). "Reduced food access due to a lack of money, inability to lift and lack of access to a car for food shopping: A multilevel study in Melbourne, Victoria". Public Health Nutrition. 14 (6): 1017–23. doi:10.1017/S136898001000385X. PMID 21338555.
- ↑ Beaulac, J; Kristjansson, E; Cummins, S (2009). "A systematic review of food deserts, 1966-2007". Preventing chronic disease. 6 (3): A105. PMC 2722409. PMID 19527577.
- ↑ Shaw, Hillary (2012). "Access to healthy food in Nantes, France". British Food Journal. 114 (2): 224–38. doi:10.1108/00070701211202403.
- ↑ (Shaw H, The Consuming Geographies of Food: Diet, Food Deserts and Obesity, 2014, Routledge, 2014, pp. 132–133), see also http://www.fooddeserts.org
- ↑ Furey, Sinéad; Strugnell, Christopher; McIlveen, Heather (2001). "An investigation of the potential existence of 'food deserts' in rural and urban areas of Northern Ireland". Agriculture and Human Values. 18 (4): 447. doi:10.1023/A:1015218502547.
- ↑ Pollard, Christina M; Lewis, Janette M; Binns, Colin W (2008). "Selecting interventions to promote fruit and vegetable consumption: From policy to action, a planning framework case study in Western Australia". Australia and New Zealand Health Policy. 5: 27. doi:10.1186/1743-8462-5-27. PMC 2621230. PMID 19108736.
- 1 2 3 4 5 6 7 8 9 Battersby, Jane; Crush, Jonathan (2014). "Africa's Urban Food Deserts". Urban Forum. 25 (2): 143–51. doi:10.1007/s12132-014-9225-5.
- ↑ Crush, Jonathan; Frayne, Bruce; Pendleton, Wade (2012). "The Crisis of Food Insecurity in African Cities". Journal of Hunger & Environmental Nutrition. 7 (2–3): 271–92. doi:10.1080/19320248.2012.702448.
- 1 2 3 4 5 6 Battersby, Jane (2012). "Beyond the Food Desert: Finding Ways to Speak About Urban Food Security in South Africa". Geografiska Annaler: Series B, Human Geography. 94 (2): 141–59. doi:10.1111/j.1468-0467.2012.00401.x.
- ↑ Central Statistical Service. "Income and Expenditure Survey 1995." DataFirst. N.p., 25 Oct. 2012. Web. 10 Nov. 2016. https://www.datafirst.uct.ac.za/dataportal/index.php/catalog/264
- ↑ Labadarios, D; Steyn, NP; Maunder, E; MacIntryre, U; Gericke, G; Swart, R; Huskisson, J; Dannhauser, A; Vorster, HH; Nesmvuni, AE; Nel, JH (2007). "The National Food Consumption Survey (NFCS): South Africa, 1999". Public Health Nutrition. 8 (5). doi:10.1079/PHN2005816.
- ↑ Human Sciences Research Council. "South African Social Attitudes Survey 2008." DataFirst. N.p., 1 July 2014. Web. 10 Nov. 2016. https://www.datafirst.uct.ac.za/dataportal/index.php/catalog/488
- ↑ Neckerman, K. M., Bader, M., Purciel, M., & Yousefzadeh, P. (2009). Measuring Food Access in Urban Areas. Built Environment and Health . Neighborhood Revitalization. (2011). Retrieved 3 10, 2011, from The District of Columbia: http://dmped.dc.gov/DC/DMPED/Programs+and+Initiatives/Neighborhood+Revitalization
- ↑ Hale, James; Knapp, Corrine; Bardwell, Lisa; Buchenau, Michael; Marshall, Julie; Sancar, Fahriye; Litt, Jill S. (2011). "Connecting food environments and health through the relational nature of aesthetics: Gaining insight through the community gardening experience". Social Science & Medicine. 72 (11): 1853–63. doi:10.1016/j.socscimed.2011.03.044. PMID 21596466.
- ↑ Meals on Wheels Association of America. (2011). The rural initiative. Retrieved from http://www.mowaa.org/page.aspx?pid=244.[]
- ↑ http://www.hhs.gov/news/press/2010pres/02/20100219a.html[]
- ↑ Schwartz, Ariel (2011). "High school students build a farmer's market in a food desert". Fast Company.
- ↑ http://www.progressivegrocer.com/la-salle-university-fresh-grocer-opens-today[]
- ↑ http://articles.philly.com/2009-08-22/news/25276116_1_supermarket-shoprite-pizza-shops[]
- ↑ Michele Ver Ploeg (2010). Access to Affordable and Nutritious Food: Measuring and Understanding Food Deserts and Their Consequences: Report to Congress. DIANE Publishing. p. 107. ISBN 978-1-4379-2134-2.
- ↑ Bonnelly, Vanessa Espaillat (January 28, 2010). "The New York City Regional Foodshed".
- ↑ Re:Vision Westwood Food Cooperative http://www.revisioninternational.org/westwood-food-coop/
- ↑ FoodStamps. "Use Your EBT to Shop for Groceries Online". www.foodstamps.org. Retrieved 2016-11-08.
- ↑ Miranne, McInnis, Stack (1998). Untitled.
- ↑ Miranne, K. B. (1998). "Income Packaging as a Survival Strategy for Welfare Mothers". Affilia. 13 (2): 211–32. doi:10.1177/088610999801300206.
- ↑ McInnis-Dittrich, K. (1995). "Women of the Shadows: Appalachian Women's Participation in the Informal Economy". Affilia. 10 (4): 398–412. doi:10.1177/088610999501000404.
- ↑ "Nutrition country profiles: Mexico summary". www.fao.org. Retrieved 2016-11-10.
- ↑ Appendini, Kirsten; Liverman, Diana (1994). "Agricultural policy, climate change and food security in Mexico". Food Policy. 19 (2): 149–64. doi:10.1016/0306-9192(94)90067-1.
- 1 2 Bermudez, Odilia I.; Tucker, Katherine L. (2003). "Trends in dietary patterns of Latin American populations". Cadernos de Saúde Pública. 19: S87–S99. doi:10.1590/S0102-311X2003000700010.
- 1 2 Uauy, Ricardo; Monteiro, Carlos Augusto (2004). "The Challenge of Improving Food and Nutrition in Latin America". Food and Nutrition Bulletin. 25 (2): 175–82. doi:10.1177/156482650402500211. PMID 15214264.
- ↑ Vargas, Lilian; Jiménez-Cruz, Arturo; Bacardí-Gascón, Montserrat (2013). "Unhealthy and Healthy Food Consumption Inside and Outside of the School by Pre-school and Elementary School Mexican Children in Tijuana, Mexico". Journal of Community Health. 38 (6): 1166–74. doi:10.1007/s10900-013-9729-2. PMID 23864428.
- ↑ Fernald, L. C.; Gutierrez, J. P.; Neufeld, L. M.; Olaiz, G; Bertozzi, S. M.; Mietus-Snyder, M; Gertler, P. J. (2004). "High Prevalence of Obesity Among the Poor in Mexico". JAMA. 291 (21): 2544–5. doi:10.1001/jama.291.21.2544. PMID 15173143.
- ↑ Rtveladze, Ketevan; Marsh, Tim; Barquera, Simon; Sanchez Romero, Luz Maria; Levy, David; Melendez, Guillermo; Webber, Laura; Kilpi, Fanny; McPherson, Klim; Brown, Martin (2013). "Obesity prevalence in Mexico: Impact on health and economic burden". Public Health Nutrition. 17 (1): 233–9. doi:10.1017/S1368980013000086. PMID 23369462.
- ↑ Cummins, S.; Flint, E.; Matthews, S. A. (2014). "New Neighborhood Grocery Store Increased Awareness of Food Access but Did Not Alter Dietary Habits or Obesity". Health Affairs. 33 (2): 283–91. doi:10.1377/hlthaff.2013.0512. PMC 4201352. PMID 24493772.
- ↑ Pearson, Tim; Russell, Jean; Campbell, Michael J.; Barker, Margo E. (2005). "Do 'food deserts' influence fruit and vegetable consumption?—a cross-sectional study". Appetite. 45 (2): 195–7. doi:10.1016/j.appet.2005.04.003. PMID 15927303.
- ↑ Wrigley, Neil; Warm, Daniel; Margetts, Barrie (2003). "Deprivation, Diet, and Food-Retail Access: Findings from the Leeds 'Food Deserts' Study". Environment and Planning A. 35: 151–88. doi:10.1068/a35150.
- ↑ Wrigley, Neil; Warm, Daniel; Margetts, Barrie; Lowe, Michelle (2004). "The Leeds 'food deserts' intervention study: What the focus groups reveal". International Journal of Retail & Distribution Management. 32 (2): 123–36. doi:10.1108/09590550410521798.
- ↑ Coleman-Jensen, Alisha J. (2010). "Working for Peanuts: Nonstandard Work and Food Insecurity Across Household Structure". Journal of Family and Economic Issues. 32: 84–97. doi:10.1007/s10834-010-9190-7.
Further reading
- Annotated bibliography of literature on food environments
- Food desert in Richmond, CA
- Food justice
- Open Source Food