Vasovagal response
| Vasovagal episode | |
|---|---|
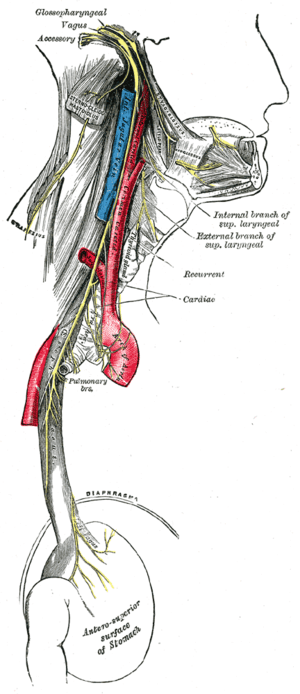 | |
| Vagus nerve | |
| Classification and external resources | |
| Specialty | Neurologycardiovascular |
| ICD-10 | R55 |
| ICD-9-CM | 78Ø.2 |
| OMIM | 609289 |
| DiseasesDB | 13777 |
| MeSH | D019462 |
A vagal episode or vasovagal response or vasovagal attack[1] (also called neurocardiogenic syncope[2]) is a malaise mediated by the vagus nerve. When it leads to fainting, also known as a "syncope", it is called a vasovagal syncope, which is the most common type of fainting.[3] Vasovagal syncope is most commonly found in adolescents and in older adults.[4]
There are different syncope syndromes which fall under the umbrella of vasovagal syncope. The common element among these conditions is the central mechanism which may lead to the loss of consciousness. The differences among them are in the factors that trigger this mechanism.
Signs and symptoms
Episodes of vasovagal response are typically recurrent and usually occur when the predisposed person is exposed to a specific trigger. Prior to losing consciousness, the individual frequently experiences early signs or symptoms such as lightheadedness, nausea, the feeling of being extremely hot or cold (accompanied by sweating), ringing in the ears (tinnitus), an uncomfortable feeling in the heart, fuzzy thoughts, confusion, a slight inability to speak/form words (sometimes combined with mild stuttering), weakness and visual disturbances such as lights seeming too bright, fuzzy or tunnel vision, black cloud-like spots in vision, and a feeling of nervousness can occur as well. The symptoms last for a few seconds before the loss of consciousness (if it is lost), which typically happens when the person is sitting up or standing.
When sufferers pass out, they fall down (unless prevented from doing so) and, when in this position, effective blood flow to the brain is immediately restored, allowing the person to regain consciousness. If the person does not fall into a fully flat, supine position, and the head remains elevated above the trunk, a state similar to a seizure may result from the blood's inability to return quickly to the brain, and the neurons in the body will fire off and generally cause muscles to twitch very slightly but mostly remain very tense. Fainting occurs with a loss of oxygen to the brain.[5]
The autonomic nervous system's physiological state (see below) leading to loss of consciousness may persist for several minutes, so
- If sufferers try to sit or stand when they wake up, they may pass out again
- The person may be nauseated, pale, and sweaty for several minutes or hours
Cause
Vasovagal syncope occurs in response to a trigger, with a corresponding malfunction in the parts of the nervous system that regulate heart rate and blood pressure. When heart rate slows, blood pressure drops, and the resulting lack of blood to the brain causes fainting and confusion.[6]
Typical triggers for vasovagal episodes include:[7]
- Prolonged standing or upright sitting
- After or during urination (micturition syncope)
- Straining, such as to have a bowel movement
- Standing up very quickly (orthostatic hypotension)
- During or post-biopsy procedures
- Stress directly related to trauma[8]
- Stress
- Postural orthostatic tachycardia syndrome (POTS). Multiple chronic episodes are experienced daily by many patients diagnosed with this syndrome. Episodes are most commonly manifested upon standing up.
- Any painful or unpleasant stimuli, such as:
- Trauma (such as hitting one's funny bone)
- Watching or experiencing medical procedures (such as venipuncture or injection)
- High pressure on or around the chest area after heavy exercise
- Severe menstrual cramps
- Sensitivity to pain
- Arousal or stimulants, e.g. sex, tickling, or adrenaline
- Sudden onset of extreme emotions
- Lack of sleep
- Hunger
- Coughing
- Being exposed to high temperatures
- Random onsets due to nerve malfunctions
- Pressing upon certain places on the throat, sinuses, and eyes (also known as vagal reflex stimulation when performed clinically)
- Use of certain drugs that affect blood pressure, such as cocaine, alcohol, marijuana, inhalants, and opiates[9]
- The sight of blood[10]
- Serotonin level / SSRI[11]
- Swallowing[12]
- (Less commonly) Low blood sugar[13]
- Time varying magnetic field[14] (e.g., transcranial magnetic stimulation)
- IUD insertion[15]
Pathophysiology
Regardless of the trigger, the mechanism of syncope is similar in the various vasovagal syncope syndromes. The nucleus tractus solitarii of the brainstem is activated directly or indirectly by the triggering stimulus, resulting in simultaneous enhancement of parasympathetic nervous system (vagal) tone and withdrawal of sympathetic nervous system tone.
This results in a spectrum of hemodynamic responses:
- On one end of the spectrum is the cardioinhibitory response, characterized by a drop in heart rate (negative chronotropic effect) and in contractility (negative inotropic effect) leading to a decrease in cardiac output that is significant enough to result in a loss of consciousness. It is thought that this response results primarily from enhancement in parasympathetic tone.
- On the other end of the spectrum is the vasodepressor response, caused by a drop in blood pressure (to as low as 80/20) without much change in heart rate. This phenomenon occurs due to vasodilation, probably as a result of withdrawal of sympathetic nervous system tone.
- The majority of people with vasovagal syncope have a mixed response somewhere between these two ends of the spectrum.
One account for these physiological responses is the Bezold-Jarisch reflex.
Diagnosis
In addition to the mechanism described above, a number of other medical conditions may cause syncope. Making the correct diagnosis for loss of consciousness is one of the most difficult challenges that a physician can face. The core of the diagnosis of vasovagal syncope rests upon a clear description by the patient of a typical pattern of triggers, symptoms, and time course. It is also pertinent to differentiate lightheadedness, seizures, vertigo, and hypoglycemia as other causes.
In patients with recurrent vasovagal syncope, diagnostic accuracy can often be improved with one of the following diagnostic tests:
- A tilt table test (results should be interpreted in the context of patients' clinical presentations and with an understanding of the sensitivity and specificity of the test)[16]
- Implantation of an insertable loop recorder
- A Holter monitor or event monitor
- An echocardiogram
- An electrophysiology study
Treatment
Treatment for vasovagal syncope focuses on avoidance of triggers, restoring blood flow to the brain during an impending episode, and measures that interrupt or prevent the pathophysiologic mechanism described above.
- The cornerstone of treatment is avoidance of triggers known to cause syncope in that person. However, a new development in psychological research has shown that patients show great reductions in vasovagal syncope through exposure-based exercises with therapists if the trigger is mental or emotional, e.g. sight of blood.[17] However, if the trigger is a specific drug, then avoidance is the only treatment.
- Because vasovagal syncope causes a decrease in blood pressure, relaxing the entire body as a mode of avoidance is not favorable.[17] A patient can move or cross his/her legs and tighten leg muscles to keep blood pressure from dropping so drastically before an injection.[18]
- Before known triggering events, the patient may increase consumption of salt and fluids to increase blood volume. Sports drinks or drinks with electrolytes may be particularly helpful.
- Discontinuation of medications known to lower blood pressure may be helpful, but stopping antihypertensive drugs can also be dangerous in some people. Taking antihypertensive drugs may worsen the syncope, as the hypertension may have been the body's way to compensate for the low blood pressure.
- Patients should be educated on how to respond to further episodes of syncope, especially if they experience prodromal warning signs: they should lie down and raise their legs, or at least lower their head to increase blood flow to the brain. If the individual has lost consciousness, he or she should be laid down with his or her head turned to the side. Tight clothing should be loosened. If the inciting factor is known, it should be removed if possible (for instance, the cause of pain).
- Wearing graded compression stockings may be helpful.
- There are certain orthostatic training exercises which have been proven to improve symptoms in people with recurrent vasovagal syncope. A technique called "Applied Tension" which involves learning to tense the muscles in the torso, arms, and legs is effective for vasovagal syncope.
- Certain medications may also be helpful:
- Beta blockers (β-adrenergic antagonists) were once the most common medication given; however, they have been shown to be ineffective in a variety of studies and are thus no longer prescribed. In addition, they may cause the syncope by lowering the blood pressure and heart rate.[19][20]
- Medications which may be effective include: CNS stimulants[21] fludrocortisone, midodrine, SSRIs[22] such as paroxetine or sertraline, disopyramide, and, in health-care settings where a syncope is anticipated, atropine epinephrine (adrenaline).[23]
- For people with the cardioinhibitory form of vasovagal syncope, implantation of a permanent pacemaker may be beneficial or even curative.[24]
- Types of Long-Term Therapy for Vasovagal Syncope include:[16]
- Preload agents
- Vasoconstrictors
- Anticholinergic agents
- Negative cardiac inotropes
- Central agents
- Mechanical device
Prognosis
Brief periods of unconsciousness do no harm and are seldom symptoms of disease.
The main danger of vasovagal syncope (or dizzy spells from vertigo) is the risk of injury by falling while unconscious. Medication therapy could possibly prevent future vasovagal responses; however, for some individuals medication is ineffective and they will continue to have fainting episodes.[25]
See also
- Roemheld Syndrome
- Postural orthostatic tachycardia syndrome
- Orthostatic hypotension
- Orthostatic intolerance
- Orthostatic tolerance
References
- ↑ "vasovagal attack" at Dorland's Medical Dictionary
- ↑ According to World Journal of Cardiology article Aydin MA, Salukhe TV, Wilke I, Willems S (2010). "Management and therapy of vasovagal syncope: A review". World Journal of Cardiology. 2: 308–15. doi:10.4330/wjc.v2.i10.308. PMC 2998831
 . PMID 21160608. the term "neurocardiogenic syncope" is no longer appropriate to use.
. PMID 21160608. the term "neurocardiogenic syncope" is no longer appropriate to use. - ↑ "Vasovagal syncope". MayoClinic.com. 7 August 2010. Retrieved 10 August 2016.
- ↑ "NEURO-CARDIOGENIC SYNCOPE" (PDF). NorthWest Ohio Cardiology Consultants: 1–2. March 2001. Archived from the original (PDF) on 2 February 2014. Retrieved 10 August 2016.
- ↑ Ajamian, Paul C (5 October 2006). "If patient faints, be laid back: what do you do when a patient passes out in your office? Lay the patient back to restore blood and oxygen to the brain.". Review of Optometry 143.7. Retrieved 10 August 2016.
- ↑ "Vasovagal syncope: Causes". MayoClinic.com. 7 August 2010. Retrieved 10 August 2016.
- ↑ "Vasomotor and vasovagal syncope". Heartdisease.about.com. Archived from the original on 2 February 2006. Retrieved 10 August 2016.
- ↑ Shalev, A., Yehuda, R., & McFarlane, A. (2000). International handbook of human response to trauma. (pp. 263-264). New York: Kluwer Academic/Plenium Publishers.
- ↑ Hilhorst, John. "Approach to syncope: Is it cardiac or not??". Cardiology. Archived from the original on 18 February 2012. Retrieved 12 August 2016.
- ↑ Zervou EK, Ziciadis K, Karabini F, Xanthi E, Chrisostomou E, Tzolou A (2005). "Vasovagal reactions in blood donors during or immediately after blood donation". Transfus Med. 15 (5): 389–94. doi:10.1111/j.1365-3148.2005.00600.x. PMID 16202053.
- ↑ Virkkunen M, Goldman D, Nielsen DA, Linnoila M (Jul 1995). "Low Brain Serotonin Turnover Rate (low CSF 5-HIAA) and Impulsive Violence". Journal of Psychiatry & Neuroscience. 20 (4): 271–275. PMC 1188701.
- ↑ Farb A, Valenti SA (1999). "Swallow syncope". Md Med J. 48 (4): 151–4. PMID 10461434.
- ↑ "fainting". The Crystal Reference Encyclopedia. 2005.
- ↑ Rossi S, Hallett M, Rossini PM, Pascual-Leone A (2009). "Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research". Clinical Neurophysiology. 120 (12): 2008–2039. doi:10.1016/j.clinph.2009.08.016. PMC 3260536. PMID 19833552.
- ↑ Baird D, Dickson J, Jensen M, Talbot M (2012). "Syncope and profound bradycardia associated with intrauterine contraceptive procedures". BMJ. 38 (3): 191–193. doi:10.1136/jfprhc-2011-100205. PMID 22253458.
- 1 2 Fenton AM, Hammill SC, Rea RF, Low PA, Shen WK (2000). "Vasovagal syncope". Ann. Intern. Med. 133 (9): 714–25. doi:10.7326/0003-4819-133-9-200011070-00014. PMID 11074905.
- 1 2 Durand, VM; DH Barlow (2006). "Essentials of Abnormal Psychology 4th Edition". p. 150. Retrieved 12 August 2016.
- ↑ France CR, France JL, Patterson SM (January 2006). "Blood pressure and cerebral oxygenation responses to skeletal muscle tension: a comparison of two physical maneuvers to prevent vasovagal reactions". Clin Physiol Funct Imaging. 26 (1): 21–5. doi:10.1111/j.1475-097X.2005.00642.x. PMID 16398666.
- ↑ Sheldon R, Connolly S, Rose S, Klingenheben T, Krahn A, Morillo C, Talajic M, Ku T, Fouad-Tarazi F, Ritchie D, Koshman ML (March 2006). "Prevention of Syncope (POST): a randomized, placebo-controlled study of metoprolol in the prevention of vasovagal syncope". Circulation. 113 (9): 1164–70. doi:10.1161/CIRCULATIONAHA.105.535161. PMID 16505178.
- ↑ Madrid AH, Ortega J, Rebollo JG, Manzano JG, Segovia JG, Sánchez A, Peña G, Moro C (February 2001). "Lack of efficacy of atenolol for the prevention of neurally mediated syncope in a highly symptomatic population: a prospective, double-blind, randomized and placebo-controlled study". J. Am. Coll. Cardiol. 37 (2): 554–9. doi:10.1016/S0735-1097(00)01155-4. PMID 11216978.
- ↑ Grubb BP, Kosinski D, Mouhaffel A, Pothoulakis A (2012-05-24). "The use of methylphenidate in the treatment of refractory neurocardiogenic syncope". Pacing Clin Electrophysiol. 19: 836–40. PMID 8734752.
- ↑ Ali Aydin, Muhammet; Salukhe, Tushar; Wilkie, Iris; Willems, Stephan (2010). "Management and therapy of vasovagal syncope: A review". World J Cardiol. 2: 308–15. doi:10.4330/wjc.v2.i10.308. PMC 2998831. PMID 21160608.
- ↑ Amy M. Karch. "epinephrine (adrenaline)". 2006 Lippincott's Nursing Drug Guide. Lippincott Williams & Wilkins. Retrieved 12 August 2016.
- ↑ "Vasovagal Syncope: What is it?". Archived from the original on 3 January 2014. Retrieved 11 August 2016.
- ↑ "Vasovagal Syncope Prognosis". MDGuidlines. Retrieved 11 August 2016.
External links
- Dysautonomia International
- Dysautonomia Information Network
- Dysautonomia Youth Network of America, Inc.
- Seattle Community Network Autism – Information regarding syncope
- Mik's Hidden Hearts Alliance for Dysautonomia
- 12 More Pages-Live & Cope with Dysautonomia