Paracetamol
 | |
 | |
| Clinical data | |
|---|---|
| Pronunciation |
Paracetamol: /ˌpærəˈsɛtəmɒl/ Acetaminophen: |
| Trade names | Tylenol, Panadol, others[1] |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a681004 |
| License data |
|
| Pregnancy category | |
| Routes of administration | By mouth, through the cheek, rectal, intravenous (IV) |
| ATC code | N02BE01 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 63–89%[2]:73 |
| Protein binding | 10–25%[3] |
| Metabolism | Predominantly in the liver[4] |
| Metabolites | APAP gluc, APAP sulfate, NAPQI, APAP-GSH, APAP-cys[5] |
| Onset of action |
Pain relief onset by route: By mouth – 37 minutes[6] Buccal – 15 minutes[6] Intravenous – 8 minutes[6] |
| Biological half-life | 1–4 hours[4] |
| Excretion | Urine (85–90%)[4] |
| Identifiers | |
| |
| CAS Number |
103-90-2 |
| PubChem (CID) | 1983 |
| IUPHAR/BPS | 5239 |
| DrugBank |
DB00316 |
| ChemSpider |
1906 |
| UNII |
362O9ITL9D |
| KEGG |
D00217 |
| ChEBI |
CHEBI:46195 |
| ChEMBL |
CHEMBL112 |
| PDB ligand ID | TYL (PDBe, RCSB PDB) |
| ECHA InfoCard | 100.002.870 |
| Chemical and physical data | |
| Formula | C8H9NO2 |
| Molar mass | 151.163 g/mol |
| 3D model (Jmol) | Interactive image |
| Density | 1.263 g/cm3 |
| Melting point | 169 °C (336 °F) [7][8] |
| Boiling point | 420 °C (788 °F) |
| Solubility in water |
7.21 g/kg (0 °C)[9] |
| |
| |
| (verify) | |
Paracetamol, also known as acetaminophen or APAP, is a medication used to treat pain and fever.[10] It is typically used for mild to moderate pain.[10] There is poor evidence for fever relief in children.[11] It is often sold in combination with other ingredients such as in many cold medications.[10] In combination with opioid pain medication, paracetamol is used for more severe pain such as cancer pain and after surgery.[12] It is typically used either by mouth or rectally but is also available intravenously.[10][13] Effects last between two and four hours.[13]
Paracetamol is generally safe at recommended doses.[14] Serious skin rashes may rarely occur, and too high a dose can result in liver failure.[10] It appears to be safe during pregnancy and when breastfeeding.[10] In those with liver disease, it may still be used, but lower doses should be taken.[15] Paracetamol is classified as a mild analgesic.[13] It does not have significant anti-inflammatory activity and how it works is not entirely clear.[16]
Paracetamol was discovered in 1877.[17] It is the most commonly used medication for pain and fever in both the United States and Europe.[18] It is on the WHO Model List of Essential Medicines, the most important medications needed in a basic health system.[19] Paracetamol is available as a generic medication with trade names including Tylenol and Panadol among others.[20] The wholesale price in the developing world is less than 0.01 USD per dose.[21] In the United States it costs about 0.04 USD per dose.[22]
Medical uses
Fever
Paracetamol is used for reducing fever in people of all ages.[23] The World Health Organization (WHO) recommends that paracetamol be used to treat fever in children only if their temperature is greater than 38.5 °C (101.3 °F).[24] The efficacy of paracetamol by itself in children with fevers has been questioned[25] and a meta-analysis showed that it is less effective than ibuprofen.[26]
Pain
Paracetamol is used for the relief of mild to moderate pain. The use of the intravenous form for pain of sudden onset in people in the emergency department is supported by limited evidence.[27]
Osteoarthritis
The American College of Rheumatology recommends paracetamol as one of several treatment options for people with arthritis pain of the hip, hand, or knee that does not improve with exercise and weight loss.[28] A 2015 review, however, found it provided only a small benefit in osteoarthritis.[29]
Paracetamol has relatively little anti-inflammatory activity, unlike other common analgesics such as the NSAIDs aspirin and ibuprofen, but ibuprofen and paracetamol have similar effects in the treatment of headache. Paracetamol can relieve pain in mild arthritis, but has no effect on the underlying inflammation, redness, and swelling of the joint.[30] It has analgesic properties comparable to those of aspirin, while its anti-inflammatory effects are weaker. It is better tolerated than aspirin due to concerns about bleeding with aspirin.
Low back pain
Based on a systematic review, paracetamol is recommended by the American College of Physicians and the American Pain Society as a first-line treatment for low back pain.[31][32] However, other systematic reviews concluded that evidence for its efficacy is lacking.[29][33]
Headaches
A joint statement of the German, Austrian, and Swiss headache societies and the German Society of Neurology recommends the use of paracetamol in combination with caffeine as one of several first line therapies for treatment of tension or migraine headache.[34] In the treatment of acute migraine, it is superior to placebo, with 39% of people experiencing pain relief at 1 hour compared to 20% in the control group.[35]
Postoperative pain
Paracetamol combined with NSAIDs may be more effective for treating postoperative pain than either paracetamol alone or NSAIDs alone.[36]
Dental use
NSAIDs such as ibuprofen, naproxen, diclofenac are more effective than paracetamol for controlling dental pain or pain arising from dental procedures; combinations of NSAIDs and paracetamol are more effective than either alone.[37] Paracetamol is particularly useful when NSAIDs are contraindicated due to hypersensitivity or history of gastrointestinal ulceration or bleeding.[38] It can also be used in combination with NSAIDs when these are ineffective in controlling dental pain alone.[39] The Cochrane review of preoperative analgesics for additional pain relief in children and adolescents shows no evidence of benefit in taking paracetamol before dental treatment to help reduce pain after treatment for procedures under local anaesthetic, however the quality of evidence is low.[40]
Other
The efficacy of paracetamol when used in combination with weak opioids (such as codeine) improved for approximately 50% of people but with increases in the number experiencing side effects.[41][42] Combination drugs of paracetamol and strong opioids like morphine improve analgesic effect.[43]
The combination of paracetamol with caffeine is superior to paracetamol alone for the treatment of common pain conditions including dental pain, postpartum pain, and headache.[44]
Adverse effects
Healthy adults taking regular doses of up to 4,000 mg a day show little evidence of toxicity (although some researchers disagree). They are more likely to have abnormal liver function tests, but the significance of this is uncertain.[29]
Liver damage
Acute overdoses of paracetamol can cause potentially fatal liver damage. In 2011 the US Food and Drug Administration launched a public education program to help consumers avoid overdose, warning: "Acetaminophen can cause serious liver damage if more than directed is used."[45][46][47] In a 2011 Safety Warning the FDA immediately required manufacturers to update labels of all prescription combination acetaminophen products to warn of the potential risk for severe liver injury and required that such combinations contain no more than 325 mg of acetaminophen.[48][49] FDA has likewise requested prescribers to limit combination opioids to 325 mg of acetaminophen. Such overdoses are frequently related to high-dose recreational use of prescription opioids, as these opioids are most often combined with acetaminophen.[50] The overdose risk may be heightened by frequent consumption of alcohol.
Paracetamol toxicity is the foremost cause of acute liver failure in the Western world and accounts for most drug overdoses in the United States, the United Kingdom, Australia, and New Zealand.[51][52][53][54] According to the FDA, in the United States there were "56,000 emergency room visits, 26,000 hospitalizations, and 458 deaths per year related to acetaminophen-associated overdoses during the 1990s. Within these estimates, unintentional acetaminophen overdose accounted for nearly 25 percent of the emergency department visits, 10 percent of the hospitalizations, and 25 percent of the deaths."[55]
Paracetamol is metabolised by the liver and is hepatotoxic; side effects are multiplied when combined with alcoholic drinks, and are very likely in chronic alcoholics or patients with liver damage.[56][57] Some studies have suggested the possibility of a moderately increased risk of upper gastrointestinal complications such as stomach bleeding when high doses are taken chronically.[58] Kidney damage is seen in rare cases, most commonly in overdose.[59]
Skin reactions
On August 2, 2013, the U.S. Food and Drug Administration (FDA) issued a new warning about paracetamol. It stated that the drug could cause rare and possibly fatal skin reactions such as Stevens–Johnson syndrome and toxic epidermal necrolysis. Prescription-strength products will be required to carry a warning label about skin reactions, and the FDA has urged manufacturers to do the same with over-the-counter products.[60]
Asthma
There is an association between paracetamol use and asthma, but the evidence suggests that this likely reflects confounders[61] rather than a causal role.[62] A 2014 review found that among children the association disappeared when respiratory infections were taken into account.[63]
As of 2014, the American Academy of Pediatrics and the National Institute for Health and Care Excellence (NICE) continue to recommend paracetamol for pain and discomfort in children,[64][65][66][67][68][69] but some experts have recommended that paracetamol use by children with asthma or at risk for asthma should be avoided.[70][71]
Other factors
In contrast to aspirin, paracetamol does not prevent blood from clotting (it is not an antithrombotic), and thus may be used in patients where failure of blood coagulation is a concern; and it does not cause gastric irritation.[72] However, paracetamol does not help reduce inflammation, while aspirin does.[73] Compared to ibuprofen—whose side effects may include diarrhea, vomiting and abdominal pain—paracetamol has fewer adverse gastrointestinal effects.[74] Unlike aspirin, paracetamol is generally considered safe for children, as it is not associated with a risk of Reye's syndrome in children with viral illnesses.[75] If taken recreationally with opioids, there is weak evidence suggesting that it may cause hearing loss.[76]
Overdose
Untreated paracetamol overdose results in a lengthy, painful illness. Signs and symptoms of paracetamol toxicity may initially be absent or non-specific symptoms. The first symptoms of overdose usually begin several hours after ingestion, with nausea, vomiting, sweating, and pain as acute liver failure starts.[77] People who take overdoses of paracetamol do not fall asleep or lose consciousness, although most people who attempt suicide with paracetamol wrongly believe that they will be rendered unconscious by the drug.[78] The process of dying from an overdose takes from 3–5 days to 4–6 weeks.
Paracetamol hepatotoxicity is by far the most common cause of acute liver failure in both the United States and the United Kingdom.[54][79] Paracetamol overdose results in more calls to poison control centers in the US than overdose of any other pharmacological substance.[80] Toxicity of paracetamol is believed to be due to its quinone metabolite.[81]
Untreated overdose can lead to liver failure and death within days. Treatment is aimed at removing the paracetamol from the body and replacing glutathione.[81] Activated charcoal can be used to decrease absorption of paracetamol if the patient presents for treatment soon after the overdose. While the antidote, acetylcysteine (also called N-acetylcysteine or NAC), acts as a precursor for glutathione, helping the body regenerate enough to prevent or at least decrease the possible damage to the liver, a liver transplant is often required if damage to the liver becomes severe.[51][82] NAC was usually given following a treatment nomogram (one for patients with risk factors, and one for those without) but the use of the nomogram is no longer recommended as evidence to support the use of risk factors was poor and inconsistent, and many of the risk factors are imprecise and difficult to determine with sufficient certainty in clinical practice.[83] NAC also helps in neutralizing the imidoquinone metabolite of paracetamol.[81] Kidney failure is also a possible side effect.
Until 2004, tablets were available (brand-name in the UK Paradote) that combined paracetamol with an antidote (methionine) to protect the liver in case of an overdose. One theoretical, but rarely if ever used, option in the United States is to request a compounding pharmacy to make a similar drug mix for at-risk patients.
In June 2009, a U.S. Food and Drug Administration (FDA) advisory committee recommended that new restrictions be placed on paracetamol usage in the United States to help protect people from the potential toxic effects. The maximum dosage at any given time would be decreased from 1000 mg to 650 mg, while combinations of paracetamol and opioid analgesics would be prohibited. Committee members were particularly concerned by the fact that the present maximum dosages of paracetamol had been shown to produce alterations in hepatic function.[84]
In January 2011, the FDA asked manufacturers of prescription combination products containing paracetamol to limit the amount of paracetamol to no more than 325 mg per tablet or capsule and began requiring manufacturers to update the labels of all prescription combination paracetamol products to warn of the potential risk of severe liver damage.[85][86][87][88] Manufacturers had three years to limit the amount of paracetamol in their prescription drug products to 325 mg per dosage unit.[86][88] In November 2011, the Medicines and Healthcare products Regulatory Agency revised UK dosing of liquid paracetamol for children.[89]
Pregnancy
Experimental studies in animals and cohort studies in humans indicate no detectable increase in congenital malformations associated with paracetamol use during pregnancy.[90] Additionally, paracetamol does not affect the closure of the fetal ductus arteriosus as NSAIDs can.[91]
Paracetamol use by the mother during pregnancy is associated with an increased risk of childhood asthma.[92] It is also associated with an increase in ADHD but it is unclear whether the relationship is causal.[93] A 2015 review states that paracetamol remains a first-line recommended medication for pain and fever during pregnancy, despite these concerns.[94]
Cancer
Some studies have found an association between paracetamol and a slight increase in kidney cancer,[95] but no effect on bladder cancer risk.[96]
Mechanism of action

To date, the mechanism of action of paracetamol is not completely understood. The main mechanism proposed is the inhibition of cyclooxygenase (COX), and recent findings suggest that it is highly selective for COX-2.[97] Because of its selectivity for COX-2, it does not significantly inhibit the production of the pro-clotting thromboxanes.[97] While it has analgesic and antipyretic properties comparable to those of aspirin or other NSAIDs, its peripheral anti-inflammatory activity is usually limited by several factors, one of which is the high level of peroxides present in inflammatory lesions.
An article[98] in Nature Communications from researchers in London, UK and Lund, Sweden in November 2011 has found a hint to the analgesic mechanism of paracetamol, being that the metabolites of paracetamol (e.g., NAPQI), act on TRPA1-receptors in the spinal cord to suppress the signal transduction from the superficial layers of the dorsal horn, to alleviate pain.
This conclusion has been contested in a new hypothesis paper[99] on how paracetamol might act. The author concedes that NAPQI is the active metabolite but that this reactive compound should react not only with the thiol in TRPA1 but also with any other suitably available nucleophile that it happens to encounter. It is suggested that thiol groups in cysteine proteases, e.g. the proteases that take part in the processing of procytokines, such as those generating IL-1β and IL-6, might be the targets giving rise to overall analgesic effects.
The COX family of enzymes are responsible for the metabolism of arachidonic acid to prostaglandin H2, an unstable molecule that is, in turn, converted to numerous other pro-inflammatory compounds. Classical anti-inflammatories such as the NSAIDs block this step. Only when appropriately oxidised is the COX enzyme highly active.[100][101] Paracetamol reduces the oxidised form of the COX enzyme, preventing it from forming pro-inflammatory chemicals.[102][103] This leads to a reduced amount of prostaglandin E2 in the CNS, thus lowering the hypothalamic set-point in the thermoregulatory centre.
Aspirin is known to inhibit the cyclooxygenase (COX) family of enzymes and, because paracetamol's action is partially similar to aspirin's, much research has focused on whether paracetamol also inhibits COX. It is now clear that paracetamol acts via at least two pathways.[104][102][105][106]
The exact mechanisms by which COX is inhibited in various circumstances are still a subject of discussion. Because of differences in the activity of paracetamol, aspirin, and other NSAIDs, it has been postulated that further COX variants may exist. One theory holds that paracetamol works by inhibiting the COX-3 isoform—a COX-1 splice variant—of the COX family of enzymes.[97] When expressed in dogs, this enzyme shares a strong similarity to the other COX enzymes, produces pro-inflammatory chemicals, and is selectively inhibited by paracetamol.[107] However, some research has suggested that, in humans and mice, the COX-3 enzyme is without inflammatory action and paracetamol's blockage of it is not significant in its functioning in humans.[97][105]
Another possibility is that paracetamol blocks cyclooxygenase (as in aspirin), but that, in an inflammatory environment where the concentration of peroxides is high, the high oxidation state of paracetamol prevents its actions. This idea would mean that paracetamol has no direct effect at the site of inflammation, but instead acts in the CNS where the environment is not oxidative, to reduce temperature, etc.[107]
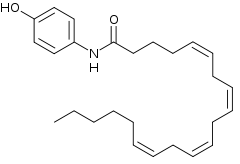
Paracetamol also modulates the endogenous cannabinoid system.[108] Paracetamol is metabolised to AM404, a compound with several actions; what is most important is that it inhibits the reuptake of the endogenous cannabinoid/vanilloid anandamide by neurons. Anandamide reuptake lowers synaptic levels of anandamide and results in more activation of the main pain receptor (nociceptor) of the body, the TRPV1 (older name: vanilloid receptor). By inhibiting anandamide reuptake, levels in the synapse remain high and are able to desensitise the TRPV1 receptor much like capsaicin. Furthermore, AM404 inhibits sodium channels, as do the anesthetics lidocaine and procaine.[109] Both of these actions by themselves have been shown to reduce pain, and are a possible mechanism for paracetamol. It has been demonstrated that when cannabinoid receptors are blocked with synthetic antagonists, paracetamol's analgesic effects are prevented, suggesting its pain-relieving action involves the endogenous cannabinoid system.[110] Spinal TRPA1 receptors have also been demonstrated to mediate antinociceptive effects of paracetamol and Δ9-tetrahydrocannabinol in mice.[111]
Increase of social behavior in mice dosed with paracetamol (which corresponds to a reduction of social rejection response in humans) does not appear to be due to cannabinoid receptor type 1 activity. It may result from serotonin receptor agonism.[112]
Pharmacokinetics
After oral administration it is rapidly absorbed by the GI tract; its volume of distribution is roughly 50 L.[113] The concentration in serum after a typical dose of paracetamol usually peaks below 30 µg/ml, which equals 200 µmol/L.[114] After 4 hours the concentration is usually less than 10 µg/mL, which equals 66 µmol/L.[114]
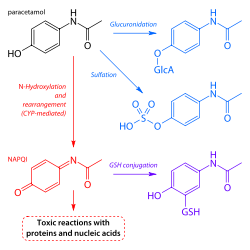
Paracetamol is metabolised primarily in the liver, into toxic and non-toxic products. Three metabolic pathways are notable:[81]
- Glucuronidation (45-55%),[4] by UGT1A1 and UGT1A6;[96]
- Sulfation (sulfate conjugation) (20–30%)[4] by SULT1A1;[96]
- N-hydroxylation and dehydration, then glutathione conjugation, (less than 15%). The hepatic cytochrome P450 enzyme system metabolises paracetamol, forming a minor yet significant alkylating metabolite known as NAPQI (N-acetyl-p-benzoquinone imine) (also known as N-acetylimidoquinone).[81][115] NAPQI is then irreversibly conjugated with the sulfhydryl groups of glutathione.[115]
All three pathways yield final products that are inactive, non-toxic, and eventually excreted by the kidneys. In the third pathway, however, the intermediate product NAPQI is toxic. NAPQI is primarily responsible for the toxic effects of paracetamol; this constitutes an example of toxication.[116] Production of NAPQI is due primarily to two isoenzymes of cytochrome P450: CYP2E1[96] and CYP3A4.[116] At usual doses, NAPQI is quickly detoxified by conjugation with glutathione.[81][115]
Chemistry
Chemical properties


Paracetamol consists of a benzene ring core, substituted by one hydroxyl group and the nitrogen atom of an amide group in the para (1,4) pattern.[117] The amide group is acetamide (ethanamide). It is an extensively conjugated system, as the lone pair on the hydroxyl oxygen, the benzene pi cloud, the nitrogen lone pair, the p orbital on the carbonyl carbon, and the lone pair on the carbonyl oxygen are all conjugated. The presence of two activating groups also make the benzene ring highly reactive toward electrophilic aromatic substitution. As the substituents are ortho, para-directing and para with respect to each other, all positions on the ring are more or less equally activated. The conjugation also greatly reduces the basicity of the oxygens and the nitrogen, while making the hydroxyl acidic through delocalisation of charge developed on the phenoxide anion.
Paracetamol is part of the class of drugs known as "aniline analgesics"; it is the only such drug still in use today.[104] It is not considered an NSAID because it does not exhibit significant anti-inflammatory activity (it is a weak COX inhibitor).[118][119] This is despite the evidence that paracetamol and NSAIDs have some similar pharmacological activity.[120]
Synthesis
Original (Boots) method
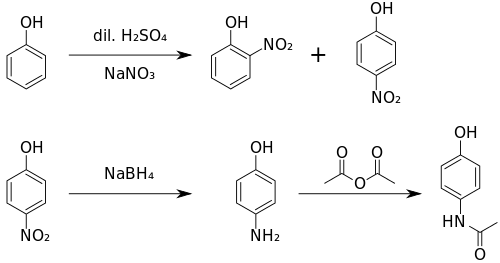
The original method for production involves the nitration of phenol with sodium nitrate gives a mixture of two isomers, from which the wanted 4-nitrophenol (bp 279 °C) can easily be separated by steam distillation. In this electrophilic aromatic substitution reaction, phenol's oxygen is strongly activating, thus the reaction requires only mild conditions as compared to nitration of benzene itself. The nitro group is then reduced to an amine, giving 4-aminophenol. Finally, the amine is acetylated with acetic anhydride.[121] Industrially direct hydrogenation is used, but in the laboratory scale sodium borohydride serves.[122][123]
Green(er) synthesis
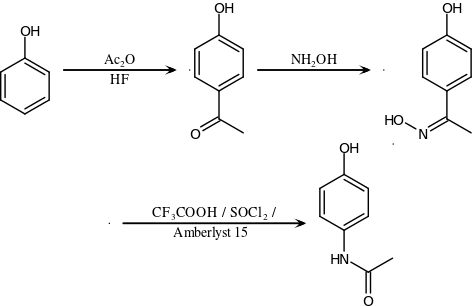
An alternative industrial synthesis developed by Hoechst–Celanese involves direct acylation of phenol with acetic anhydride catalyzed by HF, conversion of the ketone to a ketoxime with hydroxylamine, followed by the acid-catalyzed Beckmann rearrangement to give the amide.[123][124]
Direct synthesis
More recently (2014) a "one-pot" synthesis from hydroquinone has been described before the Royal Society of Chemistry.[125][126] The process may be summarized as follows:
- Hydroquinone, ammonium acetate, and acetic acid were mixed in an argon atmosphere and heated slowly to 230 °C. The mixture was stirred at this temperature for 15 hours. After cooling the acetic acid was evaporated and the precipitate was filtered, washed with water and dried to give paracetamol as a white solid.
The authors go on to claim an 88% yield and 99% purity.
Reactions
4-Aminophenol may be obtained by the amide hydrolysis of paracetamol. 4-Aminophenol prepared this way, and related to the commercially available Metol, has been used as a developer in photography by hobbyists.[127] This reaction is also used to determine paracetamol in urine samples: After hydrolysis with hydrochloric acid, 4-aminophenol reacts in ammonia solution with a phenol derivate, e.g. salicylic acid, to form an indophenol dye under oxidization by air.[128]
History

Acetanilide was the first aniline derivative serendipitously found to possess analgesic as well as antipyretic properties, and was quickly introduced into medical practice under the name of Antifebrin by A. Cahn and P. Hepp in 1886.[129] But its unacceptable toxic effects, the most alarming being cyanosis due to methemoglobinemia, prompted the search for less toxic aniline derivatives.[104] Harmon Northrop Morse had already synthesised paracetamol at Johns Hopkins University via the reduction of p-nitrophenol with tin in glacial acetic acid in 1877,[130][131] but it was not until 1887 that clinical pharmacologist Joseph von Mering tried paracetamol on patients.[104] In 1893, von Mering published a paper reporting on the clinical results of paracetamol with phenacetin, another aniline derivative.[132] Von Mering claimed that, unlike phenacetin, paracetamol had a slight tendency to produce methemoglobinemia. Paracetamol was then quickly discarded in favor of phenacetin. The sales of phenacetin established Bayer as a leading pharmaceutical company.[133] Overshadowed in part by aspirin, introduced into medicine by Heinrich Dreser in 1899, phenacetin was popular for many decades, particularly in widely advertised over-the-counter "headache mixtures", usually containing phenacetin, an aminopyrine derivative of aspirin, caffeine, and sometimes a barbiturate.[104]
Paracetamol is the active metabolite of phenacetin and acetanilide, both once popular as analgesics and antipyretics in their own right.[113][134] However, unlike phenacetin, acetanilide and their combinations, paracetamol is not considered carcinogenic at therapeutic doses.[135]
Von Mering's claims remained essentially unchallenged for half a century, until two teams of researchers from the United States analyzed the metabolism of acetanilide and paracetamol.[133] In 1947 David Lester and Leon Greenberg found strong evidence that paracetamol was a major metabolite of acetanilide in human blood, and in a subsequent study they reported that large doses of paracetamol given to albino rats did not cause methemoglobinemia.[136] In three papers published in the September 1948 issue of the Journal of Pharmacology and Experimental Therapeutics, Bernard Brodie, Julius Axelrod and Frederick Flinn confirmed using more specific methods that paracetamol was the major metabolite of acetanilide in human blood, and established that it was just as efficacious an analgesic as its precursor.[137][138][139] They also suggested that methemoglobinemia is produced in humans mainly by another metabolite, phenylhydroxylamine. A follow-up paper by Brodie and Axelrod in 1949 established that phenacetin was also metabolised to paracetamol.[140] This led to a "rediscovery" of paracetamol.[104] It has been suggested that contamination of paracetamol with 4-aminophenol, the substance von Mering synthesised it from, may be the cause for his spurious findings.[133]
Paracetamol was first marketed in the United States in 1950 under the name Triagesic, a combination of paracetamol, aspirin, and caffeine.[131] Reports in 1951 of three users stricken with the blood disease agranulocytosis led to its removal from the marketplace, and it took several years until it became clear that the disease was unconnected.[131] Paracetamol was marketed in 1953 by Sterling-Winthrop Co. as Panadol, available only by prescription, and promoted as preferable to aspirin since it was safe for children and people with ulcers.[131][133][141] In 1955, paracetamol was marketed as Children's Tylenol Elixir by McNeil Laboratories.[142] In 1956, 500 mg tablets of paracetamol went on sale in the United Kingdom under the trade name Panadol, produced by Frederick Stearns & Co, a subsidiary of Sterling Drug Inc. In 1963, paracetamol was added to the British Pharmacopoeia, and has gained popularity since then as an analgesic agent with few side-effects and little interaction with other pharmaceutical agents.[131] Concerns about paracetamol's safety delayed its widespread acceptance until the 1970s, but in the 1980s paracetamol sales exceeded those of aspirin in many countries, including the United Kingdom. This was accompanied by the commercial demise of phenacetin, blamed as the cause of analgesic nephropathy and hematological toxicity.[104] In 1988 Sterling Winthrop was acquired by Eastman Kodak which sold the over the counter drug rights to SmithKline Beecham in 1994.[143]
Available without a prescription since 1959,[144] it has since become a common household drug.[145] Patents on paracetamol have long expired, and generic versions of the drug are widely available.[1][146]
Society and culture
Naming
Acetaminophen is the name generally used in the United States (USAN), Japan (JAN), Canada[147] Venezuela, Colombia.,[148] and Iran; paracetamol is used in international venues (INN, AAN, BAN).[147][148][149] In some contexts, such as on prescription bottles of painkillers that incorporate this medicine, it is simply abbreviated as APAP, for acetyl-para-aminophenol.
Both acetaminophen and paracetamol come from a chemical name for the compound: para-acetylaminophenol and para-acetylaminophenol.
Available forms



Paracetamol is available in a tablet, capsule, liquid suspension, suppository, intravenous, intramuscular and effervescent form. The common adult dose is 500 mg to 1000 mg. The recommended maximum daily dose for adults is 4000 mg. In recommended doses, paracetamol is generally safe for children and infants as well as for adults,[150] although rare cases of acute liver injury have been linked to amounts lower than 2500 mg per day.[151]
In some formulations, paracetamol is combined with the opioid codeine, sometimes referred to as co-codamol (BAN) and Panadeine in Australia. In the U.S., this combination is available only by prescription, while the lowest-strength preparation is over the counter in Canada, and in other countries other strengths may be available over the counter. Paracetamol is also combined with other opioids such as dihydrocodeine, referred to as co-dydramol (BAN), oxycodone or hydrocodone. Another very commonly used analgesic combination includes paracetamol in combination with propoxyphene napsylate. A combination of paracetamol, codeine, and the calmative doxylamine succinate is also available. The efficacy of paracetamol/codeine combinations has been questioned by recent research.[43]
Paracetamol is commonly used in multi-ingredient preparations for migraine headache, typically including butalbital and paracetamol with or without caffeine, and sometimes containing codeine.
Paracetamol is sometimes combined with phenylephrine hydrochloride.[152] Sometimes a third active ingredient, such as ascorbic acid,[152][153] caffeine,[154][155] chlorpheniramine maleate,[156] or guaifenesin[157][158][159] is added to this combination.
When marketed in combination with diphenhydramine hydrochloride, it is frequently given the label "PM" and is meant as a sleep aid. Diphenhydramine hydrochloride is known to have hypnotic effects and is non-habit forming. Unfortunately it has been implicated in the occasional development of restless leg syndrome.[160]
Controversy
In September 2013, an episode of This American Life entitled "Use Only as Directed"[161] highlighted deaths from paracetamol overdose. This report was followed by two reports by ProPublica[162][163] alleging that the "FDA has long been aware of studies showing the risks of acetaminophen. So has the maker of Tylenol, McNeil Consumer Healthcare, a division of Johnson & Johnson" and "McNeil, the maker of Tylenol, ... has repeatedly opposed safety warnings, dosage restrictions and other measures meant to safeguard users of the drug."
A report prepared by an internal FDA working group describes a history of FDA initiatives designed to educate consumers about the risk of paracetamol overdose and notes that one challenge to the Agency has been "identifying the appropriate message about the relative safety of acetaminophen, especially compared to other OTC pain relievers (e.g., aspirin and other NSAIDs)". The report notes that "Chronic use of NSAIDs is also associated with significant morbidity and mortality. NSAID gastrointestinal risk is substantial, with deaths and hospitalization estimated in one publication as 3200 and 32,000 per year respectively. Possible cardiovascular toxicity with chronic NSAID use has been a major discussion recently", finally noting that "The goal of the educational efforts is not to decrease appropriate acetaminophen use or encourage substitution of NSAID use, but rather to educate consumers so that they can avoid unnecessary health risks."[164]
Veterinary use
Cats
Paracetamol is extremely toxic to cats, which lack the necessary glucuronyl transferase enzymes to break it down safely. Initial symptoms include vomiting, salivation, and discoloration of the tongue and gums.
Unlike an overdose in humans, liver damage is rarely the cause of death; instead, methemoglobin formation and the production of Heinz bodies in red blood cells inhibit oxygen transport by the blood, causing asphyxiation (methemoglobemia and hemolytic anemia).[165]
Treatment with N-acetylcysteine,[166] methylene blue or both is sometimes effective after the ingestion of small doses of paracetamol.
Dogs
Although paracetamol is believed to have no significant anti-inflammatory activity, it has been reported as effective as aspirin in the treatment of musculoskeletal pain in dogs.[167]
A paracetamol-codeine product (trade name Pardale-V)[168] licensed for use in dogs is available on veterinary prescription in the UK.[168] It should be administered to dogs only on veterinary advice and with extreme caution.[168]
The main effect of toxicity in dogs is liver damage, and GI ulceration has been reported.[166][169][170][171] N-acetylcysteine treatment is efficacious in dogs when administered within 2 hours of paracetamol ingestion.[166][167]
Snakes
Paracetamol is also lethal to snakes, and has been suggested as a chemical control program for the invasive brown tree snake (Boiga irregularis) in Guam.[172][173] Doses of 80 mg are inserted into dead mice scattered by helicopter.[174]
References
- 1 2 "International Listings for Paracetamol". Retrieved 11 January 2016.
- ↑ Working Group of the Australian and New Zealand College of Anaesthetists and Faculty of Pain Medicine (2010). Macintyre, PE; Schug, SA; Scott, DA; Visser, EJ; Walker, SM, eds. Acute Pain Management: Scientific Evidence (PDF) (3rd ed.). Melbourne, Australia: National Health and Medical Research Council. ISBN 9780977517459.
- ↑ "Tylenol, Tylenol Infants' Drops (acetaminophen) dosing, indications, interactions, adverse effects, and more". Medscape Reference. WebMD. Retrieved 10 May 2014.
- 1 2 3 4 5 "Codapane Forte Paracetamol and codeine phosphate PRODUCT INFORMATION" (PDF). TGA eBusiness Services. Alphapharm Pty Limited. 29 April 2013. Retrieved 10 May 2014.
- ↑ "Acetaminophen Pathway (therapeutic doses), Pharmacokinetics". Retrieved 13 January 2016.
- 1 2 3 Pickering G, Macian N, Libert F, Cardot JM, Coissard S, Perovitch P, Maury M, Dubray C (September 2014). "Buccal acetaminophen provides fast analgesia: two randomized clinical trials in healthy volunteers". Drug Des. Devel. Ther. 8: 1621–1627. doi:10.2147/DDDT.S63476. PMC 4189711
 . PMID 25302017.
. PMID 25302017. bAPAP has a faster time of antinociception onset (15 minutes, P<0.01) and greater antinociception at 50 minutes (P<0.01, CT1) and 30 minutes (P<0.01, CT2) than ivAPAP and sAPAP. All routes are similar after 50 minutes. ... In postoperative conditions for acute pain of mild to moderate intensity, the quickest reported time to onset of analgesia with APAP is 8 minutes9 for the iv route and 37 minutes6 for the oral route.
- ↑ Karthikeyan, M.; Glen, R. C.; Bender, A. (2005). "General Melting Point Prediction Based on a Diverse Compound Data Set and Artificial Neural Networks". Journal of Chemical Information and Modeling. 45 (3): 581–590. doi:10.1021/ci0500132. PMID 15921448.
- ↑ "melting point data for paracetamol". Lxsrv7.oru.edu. Retrieved 19 March 2011.
- 1 2 3 4 5 Granberg RA, Rasmuson AC (1999). "Solubility of paracetamol in pure solvents". Journal of Chemical & Engineering Data. 44 (6): 1391–95. doi:10.1021/je990124v.
- 1 2 3 4 5 6 "Acetaminophen". The American Society of Health-System Pharmacists. Retrieved 16 September 2016.
- ↑ Meremikwu, M; Oyo-Ita, A (2002). "Paracetamol for treating fever in children". The Cochrane database of systematic reviews (2): CD003676. doi:10.1002/14651858.CD003676. PMID 12076499.
- ↑ Scottish Intercollegiate Guidelines Network (SIGN) (2008). "6.1 and 7.1.1". Guideline 106: Control of pain in adults with cancer (PDF). Scotland: National Health Service (NHS). ISBN 9781905813384.
- 1 2 3 Hochhauser, Daniel (2014). Cancer and its Management. John Wiley & Sons. p. 119. ISBN 9781118468715.
- ↑ Russell, FM; Shann, F; Curtis, N; Mulholland, K (2003). "Evidence on the use of paracetamol in febrile children". Bulletin of the World Health Organization. 81 (5): 367–72. PMC 2572451. PMID 12856055.
- ↑ Lewis, JH; Stine, JG (June 2013). "Review article: prescribing medications in patients with cirrhosis - a practical guide". Alimentary pharmacology & therapeutics. 37 (12): 1132–56. doi:10.1111/apt.12324. PMID 23638982.
- ↑ McKay, Gerard A.; Walters, Matthew R. (2013). "Non-Opioid Analgesics". Lecture Notes Clinical Pharmacology and Therapeutics (9th ed.). Hoboken: Wiley. ISBN 9781118344897.
- ↑ Mangus, Brent C.; Miller, Michael G. (2005). Pharmacology application in athletic training. Philadelphia, Pennsylvania: F.A. Davis. p. 39. ISBN 9780803620278.
- ↑ Aghababian, Richard V. (22 October 2010). Essentials of emergency medicine. Jones & Bartlett Publishers. p. 814. ISBN 978-1-4496-1846-9.
- ↑ "WHO Model list of essential medicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ Hamilton, Richard J. (2013). Tarascon pocket pharmacopoeia : 2013 classic shirt-pocket edition (27th ed.). Burlington, Massachusetts: Jones & Bartlett Learning. p. 12. ISBN 9781449665869.
- ↑ "Paracetamol". Retrieved 11 January 2016.
- ↑ "Acetaminophen prices, coupons and patient assistance programs". Retrieved 19 February 2016.
- ↑ "Acetaminophen". The American Society of Health-System Pharmacists. Retrieved 3 April 2011.
- ↑ "Baby paracetamol asthma concern". BBC News. September 19, 2008. Retrieved September 19, 2008.
- ↑ Meremikwu M, Oyo-Ita A (2002). "Paracetamol for treating fever in children". Cochrane Database Syst Rev (2): CD003676. doi:10.1002/14651858.CD003676. PMID 12076499.
- ↑ Perrott DA, Piira T, Goodenough B, Champion GD (2004). "Efficacy and safety of acetaminophen vs ibuprofen for treating children's pain or fever: a meta-analysis". Arch Pediatr Adolesc Med. 158 (6): 521–6. doi:10.1001/archpedi.158.6.521. PMID 15184213.
- ↑ Sin, B; Wai, M; Tatunchak, T; Motov, SM (29 January 2016). "The use of intravenous acetaminophen for acute pain in the emergency department.". Academic Emergency Medicine. 23: 543–53. doi:10.1111/acem.12921. PMID 26824905.
- ↑ Hochberg MC, Altman RD, April KT, et al. (April 2012). "American College of Rheumatology 2012 recommendations for the use of nonpharmacologic and pharmacologic therapies in osteoarthritis of the hand, hip, and knee". Arthritis Care Res (Hoboken). 64 (4): 465–74. doi:10.1002/acr.21596. PMID 22563589.
- 1 2 3 Machado, GC; Maher, CG; Ferreira, PH; Pinheiro, MB; Lin, CW; Day, RO; McLachlan, AJ; Ferreira, ML (31 March 2015). "Efficacy and safety of paracetamol for spinal pain and osteoarthritis: systematic review and meta-analysis of randomised placebo controlled trials.". BMJ (Clinical research ed.). 350: h1225. doi:10.1136/bmj.h1225. PMID 25828856.
- ↑ "Paracetamol". Arthritis Research UK. Retrieved October 16, 2013.
- ↑ "National Guideline Clearinghouse | Expert Commentaries: Diagnosis and Treatment of Low Back Pain: A Joint Clinical Practice Guideline from the American College of Physicians and the American Pain Society. What's New? What's Different?".
- ↑ Chou R, Huffman LH (October 2007). "Medications for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline". Ann. Intern. Med. 147 (7): 505–14. doi:10.7326/0003-4819-147-7-200710020-00008. PMID 17909211.
- ↑ Davies RA, Maher CG, Hancock MJ (November 2008). "A systematic review of paracetamol for non-specific low back pain". Eur Spine J. 17 (11): 1423–30. doi:10.1007/s00586-008-0783-x. PMC 2583194. PMID 18797937.
- ↑ Haag G, Diener HC, May A, et al. (April 2011). "Self-medication of migraine and tension-type headache: summary of the evidence-based recommendations of the Deutsche Migräne und Kopfschmerzgesellschaft (DMKG), the Deutsche Gesellschaft für Neurologie (DGN), the Österreichische Kopfschmerzgesellschaft (ÖKSG) and the Schweizerische Kopfwehgesellschaft (SKG)". J Headache Pain. 12 (2): 201–17. doi:10.1007/s10194-010-0266-4. PMC 3075399. PMID 21181425.
- ↑ Derry S, Moore RA (2013). "Paracetamol (acetaminophen) with or without an antiemetic for acute migraine headaches in adults". Cochrane Database Syst Rev. 4: CD008040. doi:10.1002/14651858.CD008040.pub3. PMID 23633349.
- ↑ Ong, CK; Seymour, RA; Lirk, P; Merry, AF (1 April 2010). "Combining paracetamol (acetaminophen) with nonsteroidal antiinflammatory drugs: a qualitative systematic review of analgesic efficacy for acute postoperative pain.". Anesthesia and Analgesia. 110 (4): 1170–9. doi:10.1213/ANE.0b013e3181cf9281. PMID 20142348.
- ↑ Moore, RA; Derry, C (January 2013). "Efficacy of OTC analgesics.". International journal of clinical practice. Supplement (178): 21–5. doi:10.1111/ijcp.12054. PMID 23163544.
- ↑ "Relieving dental pain". American Dental Association. December 2016.
- ↑ Bailey, E; Worthington, H; Coulthard, P (April 2014). "Ibuprofen and/or paracetamol (acetaminophen) for pain relief after surgical removal of lower wisdom teeth, a Cochrane systematic review.". British dental journal. 216 (8): 451–5. PMID 24762895.
- ↑ Ashley, PF; Parekh, S; Moles, DR; Anand, P; MacDonald, LC (8 August 2016). "Preoperative analgesics for additional pain relief in children and adolescents having dental treatment.". The Cochrane database of systematic reviews (8): CD008392. PMID 27501304.
- ↑ Anton J M de Craen, Giuseppe Di Giulio, Angela J E M Lampe-Schoenmaeckers, Alphons G H Kessels, Jos Kleijnen (1996). "Analgesic efficacy and safety of paracetamol-codeine combinations versus paracetamol alone: a systematic review". BMJ. 313 (7053): 321–324. doi:10.1136/bmj.313.7053.321.
- ↑ Laurence Toms; Sheena Derry; R Andrew Moore; Henry J McQuay (2009). "Single dose oral paracetamol (acetaminophen) with codeine for postoperative pain in adults". Cochrane Database of Systematic Reviews (1). doi:10.1002/14651858.CD001547.pub2.
- 1 2 Murnion B (2010). "Combination analgesics in adults". Australian Prescriber (33): 113–5.
- ↑ Derry CJ, Derry S, Moore RA (2012). "Caffeine as an analgesic adjuvant for acute pain in adults". Cochrane Database Syst Rev. 3: CD009281. doi:10.1002/14651858.CD009281.pub2. PMID 22419343.
- ↑ US FDA. Page Last Updated: January 16, 2014. Acetaminophen Information Page accessed February 23, 2014
- ↑ US FDA. Page updated August 6, 2013 Acetaminophen Toxicity Page accessed February 23, 2014
- ↑ US FDA Page updated November 19, 2013 Using Acetaminophen and Nonsteroidal Anti-inflammatory Drugs Safely Page accessed February 23, 2014
- ↑ US FDA. January 13, 2011 FDA limits acetaminophen in prescription combination products; requires liver toxicity warnings Page accessed February 23, 2014
- ↑ Research, Center for Drug Evaluation and. "Drug Safety and Availability - FDA Drug Safety Communication: Prescription Acetaminophen Products to be Limited to 325 mg Per Dosage Unit; Boxed Warning Will Highlight Potential for Severe Liver Failure". www.fda.gov. Retrieved February 27, 2016.
- ↑ "FDA: Acetaminophen doses over 325 mg may lead to liver damage". Cnn.com. January 16, 2014. Retrieved 2014-02-18.
- 1 2 Daly FF, Fountain JS, Murray L, Graudins A, Buckley NA (2008). "Guidelines for the management of paracetamol poisoning in Australia and New Zealand—explanation and elaboration. A consensus statement from clinical toxicologists consulting to the Australasian poisons information centres". Med J Aust. 188 (5): 296–301. PMID 18312195.
- ↑ Khashab M, Tector AJ, Kwo PY (2007). "Epidemiology of acute liver failure". Curr Gastroenterol Rep. 9 (1): 66–73. doi:10.1007/s11894-008-0023-x. PMID 17335680.
- ↑ Hawkins LC, Edwards JN, Dargan PI (2007). "Impact of restricting paracetamol pack sizes on paracetamol poisoning in the United Kingdom: a review of the literature". Drug Saf. 30 (6): 465–79. doi:10.2165/00002018-200730060-00002. PMID 17536874.
- 1 2 Larson AM; Polson J; Fontana RJ; et al. (2005). "Acetaminophen-induced acute liver failure: results of a United States multicenter, prospective study". Hepatology. 42 (6): 1364–72. doi:10.1002/hep.20948. PMID 16317692.
- ↑ US FDA Date Posted Jan 14, 2011. Prescription Drug Products Containing Acetaminophen: Actions to Reduce Liver Injury from Unintentional Overdose Page accessed February 23, 2014
- ↑ Hughes, John (2008). Pain Management: From Basics to Clinical Practice. Elsevier Health Sciences. ISBN 9780443103360.
- ↑ Dukes, MNG; Jeffrey K Aronson (2000). Meyler's Side Effects of Drugs, Vol XIV. Elsevier. ISBN 9780444500939.
- ↑ García Rodríguez LA, Hernández-Díaz S (December 15, 2000). "The risk of upper gastrointestinal complications associated with nonsteroidal anti-inflammatory drugs, glucocorticoids, acetaminophen, and combinations of these agents". Arthritis Research & Therapy. 3 (2): 98–101. doi:10.1186/ar146. PMC 128885. PMID 11178116.
- ↑ "Painkillers 'cause kidney damage'". BBC News. November 23, 2003. Retrieved March 27, 2010.
- ↑ "FDA Warns of Rare Acetaminophen Risk". August 1, 2013. Retrieved 12 April 2016.
- ↑ Henderson, AJ; Shaheen, SO (Mar 2013). "Acetaminophen and asthma.". Paediatric Respiratory Reviews. 14 (1): 9–15; quiz 16. doi:10.1016/j.prrv.2012.04.004. PMID 23347656.
- ↑ Heintze, K; Petersen, KU (Jun 2013). "The case of drug causation of childhood asthma: antibiotics and paracetamol.". European journal of clinical pharmacology. 69 (6): 1197–209. doi:10.1007/s00228-012-1463-7. PMC 3651816. PMID 23292157.
- ↑ Cheelo, M; Lodge, CJ; Dharmage, SC; Simpson, JA; Matheson, M; Heinrich, J; Lowe, AJ (26 November 2014). "Paracetamol exposure in pregnancy and early childhood and development of childhood asthma: a systematic review and meta-analysis.". Archives of Disease in Childhood. 100: 81–9. doi:10.1136/archdischild-2012-303043. PMID 25429049.
- ↑ "Feverish illness in children: Assessment and initial management in children younger than 5 years". NICE clinical guidelines. UK National Institute for Health and Care Excellence. May 2013. Retrieved 25 February 2014.
- ↑ "Common over-the-counter medications". Healthychildren.org. American Academy of Pediatrics. July 10, 2013. Retrieved February 23, 2014.
- ↑ Heintze, K; Petersen, KU (Jun 2013). "The case of drug causation of childhood asthma: antibiotics and paracetamol". European Journal of Clinical Pharmacology. 69 (6): 1197–209. doi:10.1007/s00228-012-1463-7. PMC 3651816. PMID 23292157.
- ↑ "Link between Calpol and asthma 'not proven'". NHS Choices. UK National Health Service. September 16, 2013. Retrieved February 23, 2014.
- ↑ Section on Clinical Pharmacology and Therapeutics; Committee on Drugs; Sullivan, JE; Farrar, HC (Mar 2011). "Fever and antipyretic use in children". Pediatrics. American Academy of Pediatrics. 127 (3): 580–7. doi:10.1542/peds.2010-3852. PMID 21357332.
- ↑ CHMP Pharmacovigilance Working Party (February 24, 2011). Pharmacovigilance Working Party (PhVWP) February 2011 plenary meeting (PDF) (Report). European Medicines Agency & Heads of Medicines Agencies. pp. 6–7.
- ↑ Martinez-Gimeno, A; García-Marcos, Luis (Apr 2013). "The association between acetaminophen and asthma: should its pediatric use be banned?". Expert Review of Respiratory Medicine. 7 (2): 113–22. doi:10.1586/ers.13.8. PMID 23547988.
- ↑ McBride, JT (Dec 2011). "The association of acetaminophen and asthma prevalence and severity.". Pediatrics. 128 (6): 1181–5. doi:10.1542/peds.2011-1106. PMID 22065272.
- ↑ Sarg, Michael; Ann D Gross; Roberta Altman (2007). The Cancer Dictionary. Infobase Publishing. ISBN 9780816064113.
- ↑ Neuss,G (2007). Chemistry: Course Companion. Oxford University Press. ISBN 978-0-19-915146-2.
- ↑ Ebrahimi, Sedigheh; Soheil Ashkani Esfahani; Hamid Reza Ghaffarian; Mahsima Khoshneviszade (2010). "Comparison of efficacy and safety of acetaminophen and ibuprofen administration as single dose to reduce fever in children". Iranian Journal of Pediatrics. 20 (4): 500–501.
- ↑ Lesko SM, Mitchell AA (1999). "The safety of acetaminophen and ibuprofen among children younger than two years old". Pediatrics. 104 (4): e39. doi:10.1542/peds.104.4.e39. PMID 10506264.
- ↑ Yorgason, JG; Luxford, W; Kalinec, F (Dec 2011). "In vitro and in vivo models of drug ototoxicity: studying the mechanisms of a clinical problem.". Expert opinion on drug metabolism & toxicology. 7 (12): 1521–34. doi:10.1517/17425255.2011.614231. PMID 21999330.
- ↑ Rumack B, Matthew H (1975). "Acetaminophen poisoning and toxicity". Pediatrics. 55 (6): 871–76. PMID 1134886.
- ↑ "Paracetamol". University of Oxford Centre for Suicide Research. 25 March 2013. Retrieved 20 April 2013.
- ↑ Ryder SD, Beckingham IJ (2001). "ABC of diseases of liver, pancreas, and biliary system. Other causes of parenchymal liver disease". BMJ. 322 (7281): 290–92. doi:10.1136/bmj.322.7281.290. PMC 1119531. PMID 11157536.
- ↑ Lee WM (2004). "Acetaminophen and the U. S. Acute Liver Failure Study Group: lowering the risks of hepatic failure". Hepatology. 40 (1): 6–9. doi:10.1002/hep.20293. PMID 15239078.
- 1 2 3 4 5 6 Mehta, Sweety (August 25, 2012) Metabolism of Paracetamol (Acetaminophen), Acetanilide and Phenacetin. pharmaxchange.info
- ↑ "Highlights of Prescribing Information" (PDF). Acetadote. Retrieved 2014-02-10.
- ↑ "Paracetamol overdose: new guidance on treatment with intravenous acetylcysteine". Drug Safety Update. 6 (2): A1. September 2012.
- ↑ "FDA May Restrict Acetaminophen". Webmd.com. 2009-07-01. Retrieved 2011-03-19.
- ↑ "FDA limits acetaminophen in prescription combination products; requires liver toxicity warnings" (Press release). U. S. Food and Drug Administration (FDA). January 13, 2011. Retrieved January 13, 2011.
- 1 2 "FDA Drug Safety Communication: Prescription Acetaminophen Products to be Limited to 325 mg Per Dosage Unit; Boxed Warning Will Highlight Potential for Severe Liver Failure". U. S. Food and Drug Administration (FDA). January 13, 2011. Retrieved January 13, 2011.
- ↑ Matthew Perrone (January 13, 2011). "FDA orders lowering pain reliever in Vicodin". The Boston Globe. Associated Press. Retrieved January 13, 2011.
- 1 2 Gardiner Harris (January 13, 2011). "F. D. A. Plans New Limits on Prescription Painkillers". The New York Times. Retrieved January 13, 2011.
- ↑ "Liquid paracetamol for children: Revised UK dosing instructions have been introduced". Mhra.gov.uk. Retrieved 2014-02-18.
- ↑ Scialli, AR; Ang, R; Breitmeyer, J; Royal, MA (Dec 2010). "A review of the literature on the effects of acetaminophen on pregnancy outcome" (PDF). Reproductive Toxicology (Elmsford, N.Y.). 30 (4): 495–507. doi:10.1016/j.reprotox.2010.07.007. PMID 20659550.
- ↑ Rudolph, AM (Feb 23, 1981). "Effects of aspirin and acetaminophen in pregnancy and in the newborn". Archives of Internal Medicine. 141 (3): 358–63. doi:10.1001/archinte.141.3.358. PMID 7469626.
- ↑ Eyers, S; Weatherall, M; Jefferies, S; Beasley, R (Apr 2011). "Paracetamol in pregnancy and the risk of wheezing in offspring: a systematic review and meta-analysis" (PDF). Clinical and Experimental Allergy. 41 (4): 482–9. doi:10.1111/j.1365-2222.2010.03691.x. PMID 21338428.
- ↑ Blaser, JA; Allan, GM (July 2014). "Acetaminophen in pregnancy and future risk of ADHD in offspring.". Canadian Family Physician. 60 (7): 642. PMID 25022638.
- ↑ de Fays, L; Van Malderen, K; De Smet, K; Sawchik, J; Verlinden, V; Hamdani, J; Dogné, JM; Dan, B (August 2015). "Use of paracetamol during pregnancy and child neurological development.". Developmental medicine and child neurology. 57 (8): 718–24. doi:10.1111/dmcn.12745. PMID 25851072.
- ↑ Choueiri, TK.; Je, Y.; Cho, E. (2014). "Analgesic use and the risk of kidney cancer: a meta-analysis of epidemiologic studies.". International Journal of Cancer. 134 (2): 384–396. doi:10.1002/ijc.28093. PMC 3815746. PMID 23400756.
- 1 2 3 4 Fortuny, J.; Kogevinas, M.; Garcia-Closas, M.; Real, F. X.; Tardòn, A.; Garcia-Closas, R.; Serra, C.; Carrato, A.; Lloreta, J.; Rothman, N.; Villanueva, C.; Dosemeci, M.; Malats, N.; Silverman, D. (2006). "Use of Analgesics and Nonsteroidal Anti-inflammatory Drugs, Genetic Predisposition, and Bladder Cancer Risk in Spain". Cancer Epidemiology, Biomarkers & Prevention. 15 (9): 1696–1702. doi:10.1158/1055-9965.EPI-06-0038. PMID 16985032.
- 1 2 3 4 Hinz, B.; Cheremina, O.; Brune, K. (2008). "Acetaminophen (paracetamol) is a selective cyclooxygenase-2 inhibitor in man.". The FASEB Journal. 22 (2): 383–390. doi:10.1096/fj.07-8506com. PMID 17884974.
- ↑ Andersson DA, Gentry C, Alenmyr L, Killander D, Lewis SE, Andersson A, Bucher B, Galzi JL, Sterner O, Bevan S, Högestätt ED, Zygmunt PM (2011). "TRPA1 mediates spinal antinociception induced by acetaminophen and the cannabinoid Δ(9)-tetrahydrocannabiorcol". Nat Commun. 2: 551. doi:10.1038/ncomms1559. PMID 22109525.
- ↑ Claesson, A. "On the mechanism of paracetamol's analgesic activity and a note on related NSAID pharmacology". SlideShare. Retrieved 1 March 2013.
- ↑ Ohki S, Ogino N, Yamamoto S, Hayaishi O (1979). "Prostaglandin hydroperoxidase, an integral part of prostaglandin endoperoxide synthetase from bovine vesicular gland microsomes". J. Biol. Chem. 254 (3): 829–36. PMID 104998.
- ↑ Harvison PJ, Egan RW, Gale PH, Nelson SD (1986). "Acetaminophen as a cosubstrate and inhibitor of prostaglandin H synthase". Adv. Exp. Med. Biol. Advances in Experimental Medicine and Biology. 197: 739–47. doi:10.1007/978-1-4684-5134-4_68. ISBN 978-1-4684-5136-8. PMID 3094341.
- 1 2 Aronoff DM, Oates JA, Boutaud O (2006). "New insights into the mechanism of action of acetaminophen: Its clinical pharmacologic characteristics reflect its inhibition of the two prostaglandin H2 synthases". Clin. Pharmacol. Ther. 79 (1): 9–19. doi:10.1016/j.clpt.2005.09.009. PMID 16413237.
- ↑ Roberts, L.J. II. & Marrow, J.D. "Analgesic-antipyretic and Antiinflammatory Agents and Drugs Employed in the Treatment of Gout" in, "Goodman & Gilman's The Pharmacological Basis of Therapeutics 10th Edition" by Hardman, J.G. & Limbird, L.E. Published by McGraw Hill, 2001, pp.687–731 ISBN 0071354697
- 1 2 3 4 5 6 7 Bertolini A, Ferrari A, Ottani A, Guerzoni S, Tacchi R, Leone S (2006). "Paracetamol: new vistas of an old drug". CNS Drug Reviews. 12 (3–4): 250–75. doi:10.1111/j.1527-3458.2006.00250.x. PMID 17227290.
- 1 2 Kis B, Snipes JA, Busija DW (2005). "Acetaminophen and the cyclooxygenase-3 puzzle: sorting out facts, fictions, and uncertainties". J. Pharmacol. Exp. Ther. 315 (1): 1–7. doi:10.1124/jpet.105.085431. PMID 15879007.
- ↑ Graham GG, Scott KF (2005). "Mechanism of action of paracetamol". American journal of therapeutics. 12 (1): 46–55. doi:10.1097/00045391-200501000-00008. PMID 15662292.
- 1 2 Chandrasekharan NV, Dai H, Roos KL, et al. (2002). "COX-3, a cyclooxygenase-1 variant inhibited by acetaminophen and other analgesic/antipyretic drugs: cloning, structure, and expression". Proc. Natl. Acad. Sci. U.S.A. 99 (21): 13926–31. doi:10.1073/pnas.162468699. PMC 129799. PMID 12242329.
- ↑ Högestätt ED, Jönsson BA, Ermund A, et al. (2005). "Conversion of acetaminophen to the bioactive N-acylphenolamine AM404 via fatty acid amide hydrolase-dependent arachidonic acid conjugation in the nervous system". J. Biol. Chem. 280 (36): 31405–12. doi:10.1074/jbc.M501489200. PMID 15987694.
- ↑ Köfalvi A (2008). "9. Alternative interacting sites and novel receptors for cannabinoid ligands". Cannabinoids and the Brain. Springer-Verlag. pp. 131–160. doi:10.1007/978-0-387-74349-3_9. ISBN 978-0-387-74348-6.
- ↑ Ottani A, Leone S, Sandrini M, Ferrari A, Bertolini A (2006). "The analgesic activity of paracetamol is prevented by the blockade of cannabinoid CB1 receptors". Eur. J. Pharmacol. 531 (1–3): 280–1. doi:10.1016/j.ejphar.2005.12.015. PMID 16438952.
- ↑ Andersson, David A; Gentry, Clive; Alenmyr, Lisa; Killander, Dan; Lewis, Simon E; Andersson, Anders; Bucher, Bernard; Galzi, Jean-Luc; Sterner, Olov; Bevan, Stuart; Högestätt, Edward D; Zygmunt, Peter M (November 2011). "TRPA1 mediates spinal antinociception induced by acetaminophen and the cannabinoid Δ9-tetrahydrocannabiorcol". Nature Communications. 2 (2): 551. doi:10.1038/ncomms1559. PMID 22109525.
- ↑ Gould, G. G.; Seillier, A.; Weiss, G.; Giuffrida, A.; Burke, T. F.; Hensler, J. G.; Rock, C.; Tristan, A.; McMahon, L. R.; Salazar, A.; O'Connor, J. C.; Satsangi, N.; Satsangi, R. K.; Gu, T. T.; Treat, K.; Smolik, C.; Schultz, S. T. (2012). "Acetaminophen differentially enhances social behavior and cortical cannabinoid levels in inbred mice". Progress in Neuro-Psychopharmacology and Biological Psychiatry. 38 (2): 260–269. doi:10.1016/j.pnpbp.2012.04.011. PMC 3389197. PMID 22542870.
- 1 2 Graham, GG; Davies, MJ; Day, RO; Mohamudally, A; Scott, KF (June 2013). "The modern pharmacology of paracetamol: therapeutic actions, mechanism of action, metabolism, toxicity and recent pharmacological findings.". Inflammopharmacology. 21 (3): 201–32. doi:10.1007/s10787-013-0172-x. PMID 23719833.
- 1 2 John Marx; Ron Walls; Robert Hockberger (2013). Rosen's Emergency Medicine - Concepts and Clinical Practice. Elsevier Health Sciences. ISBN 9781455749874.
- 1 2 3 Borne, Ronald F. "Nonsteroidal Anti-inflammatory Drugs" in Principles of Medicinal Chemistry, Fourth Edition. Eds. Foye, William O.; Lemke, Thomas L.; Williams, David A. Published by Williams & Wilkins, 1995. p. 544–545.
- 1 2 Brayfield, A, ed. (15 January 2014). "Paracetamol". Martindale: The Complete Drug Reference. London, UK: Pharmaceutical Press. Retrieved 10 May 2014.
- ↑ Bales, JR; Nicholson JK; Sadler PJ (1985). "Two-dimensional proton nuclear magnetic resonance "maps" of acetaminophen metabolites in human urine". Clinical Chemistry. 31 (5): 757–762. PMID 3987005.
- ↑ Viswanathan, A. N.; Feskanich, D.; Schernhammer, E. S.; Hankinson, S. E. (2008). "Aspirin, NSAID, and Acetaminophen Use and the Risk of Endometrial Cancer". Cancer Research. 68 (7): 2507–13. doi:10.1158/0008-5472.CAN-07-6257. PMC 2857531. PMID 18381460.
- ↑ Altinoz, M. A.; Korkmaz, R. (2004). "NF-kappaB, macrophage migration inhibitory factor and cyclooxygenase-inhibitions as likely mechanisms behind the acetaminophen- and NSAID-prevention of the ovarian cancer". Neoplasma. 51 (4): 239–247. PMID 15254653.
- ↑ Byrant, Bronwen; Knights, Katleen; Salerno, Evelyn (2007). Pharmacology for health professionals. Elsevier. p. 270. ISBN 9780729537872.
- ↑ Ellis, Frank (2002). Paracetamol: a curriculum resource. Cambridge: Royal Society of Chemistry. ISBN 0-85404-375-6.
- ↑ Anthony S. Travis (2007). "Manufacture and uses of the anilines: A vast array of processes and products". In Zvi Rappoport. The chemistry of Anilines Part 1. Wiley. p. 764. ISBN 978-0-470-87171-3.
- 1 2 Elmar Friderichs, Thomas Christoph, Helmut Buschmann (2005), "Analgesics and Antipyretics", Ullmann's Encyclopedia of Industrial Chemistry, Weinheim: Wiley-VCH, doi:10.1002/14356007.a02_269.pub2
- ↑ US patent 4524217, Kenneth G. Davenport & Charles B. Hilton, "Process for producing N-acyl-hydroxy aromatic amines", published 1985-06-18, assigned to Celanese Corporation
- ↑ Joncour, Roxan; Duguet, Nicolas; Métay, Estelle; Ferreira, Amadéo; Lemaire, Marc (2014). "Amidation of phenol derivatives: a direct synthesis of paracetamol (acetaminophen) from Hydroquinone". Green Chem. 16: 2997–3002. doi:10.1039/C4GC00166D.
- ↑ Joncour, Roxan; Duguet, Nicolas; Métay, Estelle; Ferreira, Amadéo; Lemaire, Marc. "Supplementary Information Amidation of phenol derivatives: a direct synthesis of paracetamol (acetaminophen) from hydroquinone" (PDF).
- ↑ Henney, K; Dudley B (1939). Handbook of Photography. Whittlesey House. p. 324.
- ↑ Novotny PE, Elser RC (1984). "Indophenol method for acetaminophen in serum examined" (PDF). Clin. Chem. 30 (6): 884–6. PMID 6723045.
- ↑ Cahn, A; Hepp P (1886). "Das Antifebrin, ein neues Fiebermittel". Centralbl. Klin. Med. 7: 561–64.
- ↑ Morse, H.N. (1878). "Ueber eine neue Darstellungsmethode der Acetylamidophenole" [On a new method of preparing acetylamidophenol]. Berichte der deutschen chemischen Gesellschaft (in German). 11 (1): 232–3. doi:10.1002/cber.18780110151.
- 1 2 3 4 5 Milton Silverman; Mia Lydecker; Philip Randolph Lee (1992). Bad Medicine: The Prescription Drug Industry in the Third World. Stanford University Press. pp. 88–90. ISBN 0804716692.
- ↑ Von Mering, J (1893). "Beitrage zur Kenntniss der Antipyretica". Ther Monatsch. 7: 577–587.
- 1 2 3 4 Sneader, Walter (2005). Drug Discovery: A History. Hoboken, N.J.: Wiley. p. 439. ISBN 0471899801.
- ↑ Toussaint, K; Yang, XC; Zielinski, MA; Reigle, KL; Sacavage, SD; Nagar, S; Raffa, RB (December 2010). "What do we (not) know about how paracetamol (acetaminophen) works?" (PDF). Journal of Clinical Pharmacy and Therapeutics. 35 (6): 617–38. doi:10.1111/j.1365-2710.2009.01143.x. PMID 21054454.
- ↑ Bergman K, Müller L, Teigen SW (1996). "The genotoxicity and carcinogenicity of paracetamol: a regulatory (re)view". Mutat Res. 349 (2): 263–88. doi:10.1016/0027-5107(95)00185-9. PMID 8600357.
- ↑ Lester D, Greenberg LA, Carroll RP (1947). "The metabolic fate of acetanilid and other aniline derivatives: II. Major metabolites of acetanilid appearing in the blood". J. Pharmacol. Exp. Ther. 90 (1): 68–75. PMID 20241897.
- ↑ Brodie, BB; Axelrod J (1948). "The estimation of acetanilide and its metabolic products, aniline, N-acetyl p-aminophenol and p-aminophenol (free and total conjugated) in biological fluids and tissues". J. Pharmacol. Exp. Ther. 94 (1): 22–28. PMID 18885610.
- ↑ Brodie, BB; Axelrod J (1948). "The fate of acetanilide in man" (PDF). J. Pharmacol. Exp. Ther. 94 (1): 29–38. PMID 18885611.
- ↑ Flinn, Frederick B; Brodie BB (1948). "The effect on the pain threshold of N-acetyl p-aminophenol, a product derived in the body from acetanilide". J. Pharmacol. Exp. Ther. 94 (1): 76–77. PMID 18885618.
- ↑ Brodie BB, Axelrod J (1949). "The fate of acetophenetidin (phenacetin) in man and methods for the estimation of acetophenitidin and its metabolites in biological material". J Pharmacol Exp Ther. 94 (1): 58–67.
- ↑ Landau, Ralph; Achilladelis, Basil; Scriabine, Alexander (1999). Pharmaceutical Innovation: Revolutionizing Human Health. Chemical Heritage Foundation. pp. 248–249. ISBN 978-0-941901-21-5.
- ↑ Rapoport, Alan (15 December 1991). Headache Relief. Touchstone. p. 97. ISBN 978-0-671-74803-6.
- ↑ "SEC Info - Eastman Kodak Co - '8-K' for 6/30/94". Retrieved 3 March 2016.
- ↑ "Our Story". McNEIL-PPC, Inc. Retrieved March 8, 2014.
- ↑ "Medication and Drugs". MedicineNet. 1996–2010. Retrieved April 22, 2010.
- ↑ Thakkar, KB; Billa, G (Sep 2013). "The concept of: Generic drugs and patented drugs vs. brand name drugs and non-proprietary (generic) name drugs". Front Pharmacol. 4: 113. doi:10.3389/fphar.2013.00113. PMID 24062686.
- 1 2 Macintyre, Pamela; Rowbotham, David; Walker, Suellen (26 September 2008). Clinical Pain Management Second Edition: Acute Pain. CRC Press. p. 85. ISBN 978-0-340-94009-9.
- 1 2 International Nonproprietary Names (INN) for Pharmaceutical Substances: Lists 1-96 of Proposed INN and lists 1-57 of Recommended INN, cumulative list N°12. World Health Organization. 2007. p. v. ISBN 9789240560253. Retrieved 20 January 2014.
- ↑ "TGA Approved Terminology for Medicines, Section 1 – Chemical Substances" (PDF). Therapeutic Goods Administration, Department of Health and Ageing, Australian Government. July 1999: 97.
- ↑ "Acetaminophen." Physicians' Desk Reference, 63rd ed. Montvale, NJ: Thomson PDR; 2009: 1915–1916.
- ↑ "Acetaminophen Overdose and Liver Injury—Background and Options for Reducing Injury", Charles Ganley, MD, Gerald Dal Pan, MD, Bob Rappaport, MD, May 22, 2009, Retrieved July 8, 2010.
- 1 2 Atkinson, Hartley C.; Stanescu, Ioana; Anderson, Brian J. (2014). "Increased Phenylephrine Plasma Levels with Administration of Acetaminophen". New England Journal of Medicine. 370 (12): 1171–1172. doi:10.1056/NEJMc1313942. ISSN 0028-4793. PMID 24645960.
- ↑ "Ascorbic acid/Phenylephrine/Paracetamol". NHS Choices. National Health Service. Retrieved March 25, 2014.
- ↑ "Phenylephrine/Caffeine/Paracetamol dual relief". NHS Choices. National Health Service. Retrieved March 25, 2014.
- ↑ "Beechams Decongestant Plus With Paracetamol". NHS Choices. National Health Service. Retrieved March 25, 2014.
- ↑ Senyuva, H.; Ozden, T. (2002). "Simultaneous High-Performance Liquid Chromatographic Determination of Paracetamol, Phenylephrine HCl, and Chlorpheniramine Maleate in Pharmaceutical Dosage Forms" (PDF). Journal of Chromatographic Science. 40 (2): 97–100. doi:10.1093/chromsci/40.2.97. ISSN 0021-9665. PMID 11881712.
- ↑ Janin, A.; Monnet, J. (2014). "Bioavailability of paracetamol, phenylephrine hydrochloride and guaifenesin in a fixed-combination syrup versus an oral reference product". Journal of International Medical Research. 42 (2): 347–359. doi:10.1177/0300060513503762. ISSN 0300-0605. PMID 24553480.
- ↑ "Paracetamol – phenylephrine hydrochloride – guaifenesin". NPS MedicineWise. National Prescribing Service (Australia). Retrieved March 25, 2014.
- ↑ "Phenylephrine/Guaifenesin/Paracetamol". NHS Choices. National Health Service. Archived from the original on September 12, 2013. Retrieved March 25, 2014.
- ↑ "Treating a Restless Legs Sydnrome (RLS)". Consumer Reports. 2011.
- ↑ "Use Only as Directed". This American Life. Episode 505. Chicago. 20 September 2013. Public Radio International. WBEZ. Retrieved 24 September 2013.
- ↑ Gerth, Jeff; T. Christian Miller (20 September 2013). "Use Only as Directed". ProPublica. Retrieved 24 September 2013.
- ↑ Miller, T. Christian; Jeff Gerth (20 September 2013). "Dose of Confusion". ProPublica. Retrieved 24 September 2013.
- ↑ "www.fda.gov" (PDF).
- ↑ Allen AL (2003). "The diagnosis of acetaminophen toxicosis in a cat". Can Vet J. 44 (6): 509–10. PMC 340185. PMID 12839249.
- 1 2 3 Richardson, JA (2000). "Management of acetaminophen and ibuprofen toxicoses in dogs and cats" (PDF). J. Vet. Emerg. Crit. Care. 10 (4): 285–91. doi:10.1111/j.1476-4431.2000.tb00013.x.
- 1 2 Maddison, Jill E.; Stephen W. Page; David Church (2002). Small Animal Clinical Pharmacology. Elsevier Health Sciences. pp. 260–1. ISBN 0702025739.
- 1 2 3 "Pardale-V Oral Tablets". NOAH Compendium of Data Sheets for Animal Medicines. The National Office of Animal Health (NOAH). 11 November 2010. Retrieved 20 January 2011.
- ↑ Villar D, Buck WB, Gonzalez JM (1998). "Ibuprofen, aspirin and acetaminophen toxicosis and treatment in dogs and cats". Vet Hum Toxicol. 40 (3): 156–62. PMID 9610496.
- ↑ Meadows, Irina; Gwaltney-Brant, Sharon (2006). "The 10 Most Common Toxicoses in Dogs". Veterinary Medicine: 142–8.
- ↑ Dunayer, E (2004). "Ibuprofen toxicosis in dogs, cats, and ferrets". Veterinary Medicine: 580–6.
- ↑ Johnston J, Savarie P, Primus T, Eisemann J, Hurley J, Kohler D (2002). "Risk assessment of an acetaminophen baiting program for chemical control of brown tree snakes on Guam: evaluation of baits, snake residues, and potential primary and secondary hazards". Environ Sci Technol. 36 (17): 3827–33. doi:10.1021/es015873n. PMID 12322757.
- ↑ Brad Lendon (2010-09-07). "Tylenol-loaded mice dropped from air to control snakes". CNN. Retrieved 2010-09-07.
- ↑ Sabrina Richards (2012-05-01). "It's Raining Mice". The Scientist.
External links
| Wikimedia Commons has media related to Paracetamol. |
 Pharmacy and Pharmacology portal
Pharmacy and Pharmacology portal- Paracetamol at Chemsynthesis
- Paracetamol International Chemical Safety Cards
- The Julius Axelrod Papers
- FDA: Safe Use of Over-the-Counter Pain Relievers/Fever Reducers
- FDA: Consumer Update "Acetaminophen and Liver Injury: Q and A for Consumers" (link)
- FDA: Consumer Update "Acetaminophen and Liver Injury: Q and A for Consumers" (PDF)
- U.S. National Library of Medicine: Drug Information Portal–Paracetamol
- Acetaminophen bound to proteins in the PDB