Scoliosis
| Scoliosis | |
|---|---|
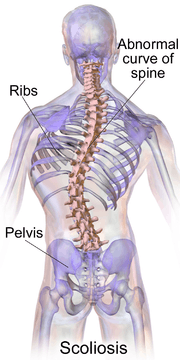 | |
| A drawing of scoliosis | |
| Pronunciation | /ˌskoʊlɪˈoʊsɪs/[1] |
| Classification and external resources | |
| Specialty | Orthopedics |
| ICD-10 | M41 |
| ICD-9-CM | 737 |
| DiseasesDB | 26545 |
| MedlinePlus | 001241 |
Scoliosis is a medical condition in which a person's spine has a sideways curve.[2] The curve is usually "S" or "C" shaped.[2] In some the degree of curve is stable, while in others it increases over time. Mild scoliosis does not typically cause problems, while severe cases can interfere with breathing.[3][4] Pain is typically not present.[5]
The cause of most cases is unknown but believed to involve a combination of genetic and environmental factors.[3] Risk factors include other affected family members. It can also occur due to another condition such as muscles spasms, cerebral palsy, Marfan syndrome, and tumors such as neurofibromatosis. Diagnosis is confirmed with plain X-rays. Scoliosis is typically classified as either structural in which the curve is fixed or functional in which the underlying spine is normal.[2]
Treatment depends on the degree of curve, location, and cause. Minor curves may simply be watched periodically. Treatments may include bracing or surgery. The brace must be fitted to the person and used daily until growing stops. Evidence for chiropractic manipulation, dietary supplements, and exercises to prevent worsening is lacking. Exercise, however, is still recommended due to its other benefits.[2]
Scoliosis occurs in about 3% of people.[6] It most commonly occurs between the ages of ten and twenty.[2] Girls typically are more severely affected than boys.[2][3] The term is from Ancient Greek: σκολίωσις skoliosis which means "a bending".[7]
Definition
Scoliosis is defined as a three-dimensional deviation in the axis of a person's spine[8] In the diagnostic sense it is defined as a spinal curvature of more than 10 degrees to the right or left as the examiner faces the person, i.e. in the coronal plane. Deformity may also exist to the front or back as the examiner looks at the person from the side, i.e. in the sagittal plane.
Scoliosis has been described as a biomechanical deformity, the progression of which depends on asymmetric forces otherwise known as the Heuter-Volkmann law.[9]
Signs and symptoms

Symptoms of scoliosis can include:
- Constipation due to tightened organs from curvature
- Pain in back, shoulders, and neck and buttock pain nearest bottom of the back
- Nerve pinching of the leg may cause the legs to cut out
- Limited mobility
- Painful menstruation (dysmenorrhea) because of a secondary pelvic tilt
The signs of scoliosis can include:
- Uneven musculature on one side of the spine
- Rib prominence or a prominent shoulder blade, caused by rotation of the rib cage in thoracic scoliosis
- Uneven hips, arms or leg lengths
- Slow nerve action
- Heart and lung problems in severe cases
- Calcium deposits (ectopic calcification) in the cartilage endplate and sometimes in the disc itself[10]
Course
People who have reached skeletal maturity are less likely to have a worsening case.[11] Some severe cases of scoliosis can lead to diminishing lung capacity, pressure exerted on the heart, and restricted physical activities.[12]
Recent longitudinal studies reveal that the most common form of the condition, late-onset idiopathic scoliosis, causes little physical impairment other than back pain and cosmetic concerns, even when untreated, with mortality rates similar to the general population.[13][14] Older beliefs that untreated idiopathic scoliosis necessarily progresses into severe (cardiopulmonary) disability by old age have been refuted by later studies.[15]
Causes
There are many causes of scoliosis, including congenital spine deformities (those present at birth like cerebral palsy, spina bifida) and neuromuscular problems, inherited diseases or conditions caused by the environment, limb length inequality and tumors.
An estimated 65% of scoliosis cases are idiopathic, about 15% are congenital and about 10% are secondary to a neuromuscular disease.[16]
Unknown
Idiopathic scoliosis represents a majority of cases, but its causes are largely unknown. Results of recent studies indicate potential heritability of the disorder. About 38% of variance in scoliosis risk is due to genetic factors, and 62% is due to the environment.[17] The genetics are likely complex however, given the inconsistent inheritance and discordance among monozygotic twins.[17] The specific genes that contribute to development of scoliosis have not been conclusively identified. At least one gene, CHD7, has been associated with the idiopathic form of scoliosis.[18] Several candidate gene studies have found associations between idiopathic scoliosis and genes mediating bone formation, bone metabolism, and connective tissue structure.[17] Several genome-wide studies have identified a number of loci as significantly linked to idiopathic scoliosis.[17] In 2006 idiopathic scoliosis was linked with three microsatellite polymorphisms in the MATN1 gene (encoding for Matrilin 1, cartilage matrix protein).[19] Fifty-three single nucleotide polymorphism markers in the DNA that are significantly associated with adolescent idiopathic scoliosis were identified through a genome-wide association study.[9]
Adolescent idiopathic scoliosis (AIS) has no clear causal agent, and is generally believed to be multifactorial.[18][20] The prevalence of scoliosis is 1% to 2% among adolescents, however the likelihood of progression among adolescents with a Cobb angle of less than 20° is about 10% to 20%.[8]
Congenital scoliosis can be attributed to a malformation of the spine during weeks three to six in utero due to a failure of formation, a failure of segmentation, or a combination of stimuli.[21] Incomplete and abnormal segmentation results in an abnormally shaped vertebra, at times fused to a normal vertebra or unilaterally fused vertebrae, leading to the abnormal lateral curvature of the spine.[22]
Secondary scoliosis
Secondary scoliosis due to neuropathic and myopathic conditions can lead to a loss of muscular support for the spinal column so that the spinal column is pulled in abnormal directions. Some conditions which may cause secondary scoliosis include muscular dystrophy, spinal muscular atrophy, poliomyelitis, cerebral palsy, spinal cord trauma, and myotonia.[23][24] Scoliosis often presents itself, or worsens, during an adolescent's growth spurt and is more often diagnosed in females than males.[8]
Scoliosis associated with known syndromes is often subclassified as "syndromic scoliosis". Scoliosis can be associated with amniotic band syndrome, Arnold–Chiari malformation, Charcot–Marie–Tooth disease, cerebral palsy, congenital diaphragmatic hernia, connective tissue disorders, muscular dystrophy, familial dysautonomia, CHARGE syndrome, Ehlers–Danlos syndrome (hyperflexibility, "floppy baby" syndrome, and other variants of the condition), fragile X syndrome,[25][26] Friedreich's ataxia, hemihypertrophy, Loeys-Dietz syndrome, Marfan's syndrome, nail–patella syndrome, neurofibromatosis, osteogenesis imperfecta, Prader–Willi syndrome, proteus syndrome, spina bifida, spinal muscular atrophy and syringomyelia.
Diagnosis

People who initially present with scoliosis are examined to determine whether the deformity has an underlying cause. During a physical examination, the following are assessed to exclude the possibility of underlying condition more serious than simple scoliosis.
The person's gait is assessed, and there is an exam for signs of other abnormalities (e.g., spina bifida as evidenced by a dimple, hairy patch, lipoma, or hemangioma). A thorough neurological examination is also performed, the skin for café au lait spots, indicative of neurofibromatosis, the feet for cavovarus deformity, abdominal reflexes and muscle tone for spasticity.
When a person can cooperate, he or she is asked to bend forward as far as possible. This is known as the Adams Forward Bend Test[27] and is often performed on school students. If a prominence is noted, then scoliosis is a possibility and an X-ray may be done to confirm the diagnosis.
As an alternative, a scoliometer may be used to diagnose the condition.[28]
When scoliosis is suspected, weight-bearing full-spine AP/coronal (front-back view) and lateral/sagittal (side view) X-rays are usually taken to assess the scoliosis curves and the kyphosis and lordosis, as these can also be affected in individuals with scoliosis. Full-length standing spine X-rays are the standard method for evaluating the severity and progression of the scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at three- to 12-month intervals to follow curve progression, and, in some instances, MRI investigation is warranted to look at the spinal cord.
The standard method for assessing the curvature quantitatively is measuring the Cobb angle, which is the angle between two lines, drawn perpendicular to the upper endplate of the uppermost vertebra involved and the lower endplate of the lowest vertebra involved. For people with two curves, Cobb angles are followed for both curves. In some people, lateral-bending X-rays are obtained to assess the flexibility of the curves or the primary and compensatory curves.
Congenital and idiopathic scoliosis that develops before age of 10 is referred to as early onset scoliosis (EOS).[29] Scoliosis that develops after 10 is referred to as adolescent idiopathic scoliosis.[3]
Genetic testing for AIS, which became available in 2009 and is still under investigation, attempts to gauge the likelihood of curve progression.[30]
Management
The traditional medical management of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression. The conventional options for children and adolescents are:[31]
- Observation
- Bracing
- Surgery
For adults, treatment usually focuses on relieving any pain:[32][33]
- Painkilling medication
- Bracing
- Surgery[34]
Treatment for idiopathic scoliosis also depends upon the severity of the curvature, the spine’s potential for further growth, and the risk that the curvature will progress. Mild scoliosis (less than 30 degrees deviation) may simply be monitored and treated with exercise. Moderately severe scoliosis (30–45 degrees) in a child who is still growing may require bracing. Severe curvatures that rapidly progress may be treated surgically with spinal rod placement. Bracing may prevent a progressive curvature, but evidence for this is not very strong. In all cases, early intervention offers the best results. A growing body of scientific research testifies to the efficacy of specialized treatment programs of physical therapy, which may include bracing.[35]
Bracing

Bracing is normally done when the person has bone growth remaining and is, in general, implemented to hold the curve and prevent it from progressing to the point where surgery is recommended. In some cases with juveniles, bracing has reduced curves significantly, going from a 40 degrees (of the curve, mentioned in length above.) out of the brace to 18 degrees in it. Braces are sometimes prescribed for adults to relieve pain related to scoliosis. Bracing involves fitting the patient with a device that covers the torso; in some cases, it extends to the neck. The most commonly used brace is a TLSO, such as a Boston brace, a corset-like appliance that fits from armpits to hips and is custom-made from fiberglass or plastic. It is sometimes worn 22–23 hours a day, depending on the doctor's prescription, and applies pressure on the curves in the spine. The effectiveness of the brace depends not only on brace design and orthotist skill but on patient compliance and amount of wear per day. The typical use of braces is for idiopathic curves that are not grave enough to warrant surgery, but they may also be used to prevent the progression of more severe curves in young children, to buy the child time to grow before performing surgery, which would prevent further growth in the part of the spine affected.
Indications for bracing: people who are still growing who present with Cobb angles less than 20 degrees should be closely monitored. People who are still growing who present with Cobb angles of 20 degrees to 29 degrees should be braced according to the risk of progression by considering age, Cobb angle increase over a six-month period, Risser sign, and clinical presentation. People who are still growing who present with Cobb angles greater than 30 degrees should be braced. However, these are guidelines and not every person will fit into this table. For example, a person who is still growing with a 17-degree Cobb angle and significant thoracic rotation or flatback could be considered for nighttime bracing. On the opposite end of the growth spectrum, a 29-degree Cobb angle and a Risser sign three or four might not need to be braced because there is reduced potential for progression.[36] The Scoliosis Research Society's recommendations for bracing include curves progressing to larger than 25°, curves presenting between 30 and 45°, Risser sign 0, 1, or 2 (an X-ray measurement of a pelvic growth area), and less than six months from the onset of menses in girls.[37]
Scoliosis braces are usually comfortable, especially when it is well designed and fit; also after the 7- to 10-day break-in period. A well fit and functioning scoliosis brace provides comfort when it is supporting the deformity and redirecting the body into a more corrected and normal physiological position.[38]
Evidence supports that bracing prevents worsening of disease but it is unclear if it changes quality of life, appearance, or back pain.[39]
Surgery


Surgery is usually recommended by orthopedists for curves with a high likelihood of progression (i.e., greater than 45 to 50° of magnitude), curves that would be cosmetically unacceptable as an adult, curves in patients with spina bifida and cerebral palsy that interfere with sitting and care, and curves that affect physiological functions such as breathing.
Surgery is indicated by the Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT) at 45 degrees to 50 degrees[40] and by the Scoliosis Research Society (SRS) at a Cobb angle of 45 degrees.[41] SOSORT uses the 45-degree to 50-degree threshold as a result of the well-documented, plus or minus five degrees measurement error that can occur while measuring Cobb angles.
Surgery for scoliosis is performed by a surgeon specializing in spine surgery. For various reasons, it is usually impossible to completely straighten a scoliotic spine, but in most cases, significant corrections are achieved.
The two main types of surgery are:
- Anterior fusion: This surgical approach is through an incision at the side of the chest wall.
- Posterior fusion: This surgical approach is through an incision on the back and involves the use of metal instrumentation to correct the curve.
One or both of these surgical procedures may be needed. The surgery may be done in one or two stages and, on average, takes four to eight hours.
Prognosis
A 50-year follow-up study published in the Journal of the American Medical Association (2003) asserted the lifelong physical health, including cardiopulmonary and neurological functions, and mental health of idiopathic scoliosis patients are comparable to those of the general population. Scoliosis that interferes with normal systemic functions is "exceptional"[42] and "rare", and "untreated [scoliosis] patients had similar death rates and were just as functional and likely to lead productive lives 50 years after diagnosis as people with normal spines".[13][43] In an earlier University of Iowa follow-up study, 91 percent of idiopathic scoliosis patients displayed normal pulmonary function, and their life expectancy was 2% longer than that of the general population.[14]
Generally, the prognosis of scoliosis depends on the likelihood of progression. The general rules of progression are larger curves carry a higher risk of progression than smaller curves, and thoracic and double primary curves carry a higher risk of progression than single lumbar or thoracolumbar curves. In addition, patients not having yet reached skeletal maturity have a higher likelihood of progression (i.e., if the patient has not yet completed the adolescent growth spurt).
Epidemiology
Scoliosis affects 2–3% of the United States population, which is equivalent to about 5 to 9 million cases.[44] A scoliosis spinal column's curve of 10° or less affects 1.5% to 3% of individuals.[37] The age of onset is usually between 10 years and 15 years (can occur at a younger age) children and adolescents, making up to 85% of those diagnosed. This is seen to be due to rapid growth spurts occurring at puberty when spinal development is most relenting to genetic and environmental influences.[45] Because female adolescents undergo growth spurts before postural musculoskeletal maturity, scoliosis is more prevalent among females.[46] Although fewer cases are present today using Cobb angle analysis for diagnosis, scoliosis remains a prevailing condition, appearing in otherwise healthy children. Incidence of idiopathic scoliosis (IS) stops after puberty when skeletal maturity is reached, however, further curvature may proceed during late adulthood due to vertebral osteoporosis and weakened musculature.[44]
Cost
The cost of scoliosis involves both monetary losses and lifestyle limitations that increase with severity. Respiratory deficiencies may also arise from thoracic deformities and cause abnormal breathing.[47] This directly affects exercise and work capacity, decreasing the overall quality of life.[44]
In the health care system of the United States, the average hospital cost for cases involving surgical procedures was $30,000 to $60,000 per patient in 2010.[48] As of 2006 the costs of bracing has been published as up to $5,000 during rapid growth periods, when braces must be consistently replaced across multiple follow-ups.[44]
Evolutionary considerations

There are links between human spinal morphology, bipedality, and scoliosis which suggest an evolutionary basis for the condition. Scoliosis has not been found in chimpanzees or gorillas.[49] Thus, it has been hypothesized that scoliosis may actually be related to humans’ morphological differences from these apes.[49] Other apes have a shorter and less mobile lower spine than humans. Some of the lumbar vertebrae in Pan are "captured", meaning that they are held fast between the ilium bones of the pelvis. Compared to humans, Old World monkeys have far larger erector spinae muscles, which are the muscles hold the spine steady.[49] These factors make the lumbar spine of most primates less flexible and far less likely to deviate than those of humans. While this may explicitly relate only to lumbar scolioses, it is possible that small imbalances in the lumbar spine could precipitate thoracic problems as well.[49]
Scoliosis may be a byproduct of strong selection for bipedalism. For a bipedal stance a highly mobile, elongated lower spine is very beneficial.[49] For instance, the human spine takes on an S-shaped curve with lumbar lordosis, which allows for better balance and support of an upright trunk.[50] Selection for bipedality was likely strong enough to justify the maintenance of such a disorder. Bipedality is hypothesized to have emerged for a variety of different reasons, many of which would have certainly conferred fitness advantages. It may increase viewing distance, which can be beneficial in hunting and foraging as well as protection from predators or other humans; it makes long distance travel more efficient for foraging or hunting; and it facilitates terrestrial feeding from grasses, trees, and bushes.[51] Given the many benefits of bipedality which depends on a particularly formed spine, it is likely that selection for bipedalism played a large role in the development of the spine as we see it today, in spite of the potential for "scoliotic deviations".[49] According to the fossil record, scoliosis may have been more prevalent among earlier hominids such as Australopithecus and Homo erectus, when bipedality was first emerging. Their fossils indicate that there may have been selection over time for a slight reduction in lumbar length to what we see today, favoring a spine that could efficiently support bipedality with a lower risk of scoliosis.[49]
See also
- Back brace
- Kyphosis
- Lordosis
- Neuromechanics of idiopathic scoliosis
- Pott disease
- Scheuermann's disease
- Schooliosis
- Scoliosis Research Society
References
- ↑ "scoliosis". Merriam Webster. Retrieved 12 August 2016.
- 1 2 3 4 5 6 "Questions and Answers about Scoliosis in Children and Adolescents". NIAMS. December 2015. Retrieved 12 August 2016.
- 1 2 3 4 "adolescent idiopathic scoliosis". Genetics Home Reference. September 2013. Retrieved 12 August 2016.
- ↑ Yang, S; Andras, LM; Redding, GJ; Skaggs, DL (January 2016). "Early-Onset Scoliosis: A Review of History, Current Treatment, and Future Directions.". Pediatrics. 137 (1). PMID 26644484.
- ↑ Agabegi, SS; Kazemi, N; Sturm, PF; Mehlman, CT (December 2015). "Natural History of Adolescent Idiopathic Scoliosis in Skeletally Mature Patients: A Critical Review.". The Journal of the American Academy of Orthopaedic Surgeons. 23 (12): 714–23. PMID 26510624.
- ↑ Shakil, H; Iqbal, ZA; Al-Ghadir, AH (2014). "Scoliosis: review of types of curves, etiological theories and conservative treatment.". Journal of back and musculoskeletal rehabilitation. 27 (2): 111–5. PMID 24284269.
- ↑ "scoliosis". Dictionary.com. Retrieved 12 August 2016.
- 1 2 3 Trobisch P, Suess O, Schwab F (December 2010). "Idiopathic Scoliosis". Disch Arztebi Int. 107 (49): 875–884. doi:10.3238/arztebl.2010.0875 (inactive 2015-01-09). PMC 3011182
 . PMID 21191550.
. PMID 21191550. - 1 2 Ogilvie J (2010). "Adolescent idiopathic scoliosis and genetic testing". Current Opinion in Pediatrics. 22 (1): 67–70. doi:10.1097/MOP.0b013e32833419ac. PMID 19949338.
- ↑ Giachelli CM (March 1999). "Ectopic calcification: gathering hard facts about soft tissue mineralization". Am. J. Pathol. 154 (3): 671–5. doi:10.1016/S0002-9440(10)65313-8. PMC 1866412. PMID 10079244.
- ↑ Thometz, J. G.; Simon, S. R. (1988-10-01). "Progression of scoliosis after skeletal maturity in institutionalized adults who have cerebral palsy". The Journal of Bone and Joint Surgery. American Volume. 70 (9): 1290–1296. ISSN 0021-9355. PMID 3182881.
- ↑ Koumbourlis, Anastassios C. "Scoliosis and the respiratory system". Paediatric Respiratory Reviews. 7 (2): 152–160. doi:10.1016/j.prrv.2006.04.009.
- 1 2 Weinstein, S. L.; Dolan, L. A.; Spratt, K.F.; Peterson, K. K.; Spoonamore, M. J.; Ponseti, I. V. (2003). "Health and Function of Patients With Untreated Idiopathic Scoliosis: A 50-Year Natural History Study". JAMA. 289 (5): 559–567. doi:10.1001/jama.289.5.559. PMID 12578488.
- 1 2 Weinstein SL, Zavala DC, Ponseti IV (June 1981). "Idiopathic scoliosis: long-term follow-up and prognosis in untreated patients". The Journal of bone and joint surgery. 63 (5): 702–12. PMID 6453874.
- ↑ "It was once assumed, on the basis of studies in heterogeneous patient populations, that patients with untreated adolescent scoliosis would necessarily become wheelchair-dependent in old age and were likely to die of cardiopulmonary arrest for reasons related to scoliosis. This is no longer held to be the case. (Dtsch Arztebl Int. Dec 2010; 107(49): 875–884.)"
- ↑ Page 90 in: Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
- 1 2 3 4 Gorman, Kristen Fay; Julien, Cédric; Moreau, Alain (14 June 2012). "The genetic epidemiology of idiopathic scoliosis". European Spine Journal. 21 (10): 1905–1919. doi:10.1007/s00586-012-2389-6. PMID 22695700.
- 1 2 Ogilvie JW, Braun J, Argyle V, Nelson L, Meade M, Ward K (2006). "The search for idiopathic scoliosis genes". Spine. 31 (6): 679–681. doi:10.1097/01.brs.0000202527.25356.90. PMID 16540873.
- ↑ Lucio Montanaro; Patrizio Parisini; Tiziana Greggi; Mario Di Silvestre; Davide Campoccia; Simona Rizzi; Carla R. Arciola (2006). "Evidence of a linkage between matrilin-1 gene (MATN1) and idiopathic scoliosis". Scoliosis. 1: 21. doi:10.1186/1748-7161-1-21. PMC 1769398. PMID 17176459.
- ↑ Kouwenhoven JW, Castelein RM; Castelein (2008). "The pathogenesis of adolescent idiopathic scoliosis: review of the literature". Spine. 33 (26): 2898–2908. doi:10.1097/BRS.0b013e3181891751. PMID 19092622.
- ↑ "What is Scoliosis: What Causes Scoliosis?". MedicalBug. 17 February 2012. Retrieved 18 March 2012.
- ↑ Scoliosis Research Society. (2014). Congenital Scoliosis. Scoliosis Research Society. http://www.srs.org/professionals/conditions_and_treatment/congenital_scoliosis/
- ↑ Trontelj, J., Pecak, F., & Dimitrijevic, M. (1979). Segmental Neurophysiological Mechanisms in Scoliosis. The Journal of Bone and Joint Surgery Vol. 61-B, No. 3. HighWire.
- ↑ POSNA. (2014). Neuromuscular Scoliosis. The Pediatric Orthopaedic Society of North America. http://www.posna.org/education/StudyGuide/neuromuscularScoliosis.asp
- ↑ "Fragile X syndrome". Department for Work and Pensions, U.K. Retrieved 29 August 2011.
- ↑ "Orthopaedic aspects of fragile-X syndrome". J Bone Joint Surg Am. The National Center for Biotechnology Information. 72: 889–96. Jul 1990. PMID 2195034.
- ↑ "Scoliosis symptoms — pain, flat back, screening, self-assessment". iscoliosis.com.
- ↑ "Scoliometer (Inclinometer)". National Scoliosis Foundation.
- ↑ "Early Onset Scoliosis | Scoliosis Research Society". www.srs.org. Retrieved 2016-07-10.
- ↑ M. Stenning; I. Nelson (2011). "Recent advances in the treatment of scoliosis in children". British Editorial Society of Bone and Joint Surgery. Retrieved 1 January 2014.
- ↑ "Treating scoliosis in children". NHS Choices. 19 February 2013. Retrieved 14 May 2014.
- ↑ "Scoliosis – Treatment in adults". NHS Choices. 19 February 2013. Retrieved 14 May 2014.
- ↑ "Idiopathic Scoliosis – Adult Nonoperative Management". Scoliosis Research Society. Retrieved 14 May 2014.
- ↑ "Idiopathic Scoliosis – Adult Surgical Treatment". Scoliosis Research Society. Retrieved 14 May 2014.
- ↑ Negrini S, Fusco C, Minozzi S, Atanasio S, Zaina F, Romano M (2008). "Exercises reduce the progression rate of adolescent idiopathic scoliosis: results of a comprehensive systematic review of the literature". Disability and Rehabilitation. 30 (10): 772–785. doi:10.1080/09638280801889568. PMID 18432435.
- ↑ Wood, Grant (2013) Published in the Academy Today (The Edge) by the American Academy of Orthosits and Prosthetist. To Brace or Not to Brace: The Three-Dimensional Nature and Growth Considerations for Adolescent Idiopathic Scoliosis, July 2013 edition pages 5 – 8,
- 1 2 Herring JA (2002). Tachdjian's Pediatric Orthopaedics. Philadelphia PA: W.B. Saunders. ISBN 0-7216-5684-6.
- ↑ Wood, G.I. (2013), Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT): The Cheneau Brace using Rigo Principles and the Wood Cheneau Rigo (WCR) Brace. Chicago, IL.
- ↑ Negrini, S; Minozzi, S; Bettany-Saltikov, J; Chockalingam, N; Grivas, TB; Kotwicki, T; Maruyama, T; Romano, M; Zaina, F (18 June 2015). "Braces for idiopathic scoliosis in adolescents.". The Cochrane database of systematic reviews (6): CD006850. PMID 26086959.
- ↑ Negrini S, et al. Scoliosis Orthopaedic and Rehabilitation Treatment, SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. 2011. http://www.scoliosisjournal.com/content/7/1/3 . Accessed January 27, 2013.
- ↑ http://www.srs.org/patient_and_family/scoliosis/idiopathic/ adolescents/surgical_treatment.htm. Accessed January 27, 2013
- ↑ Health and Function of Patients With Untreated Idiopathic Scoliosis—Reply
- ↑ Many With Scoliosis Can Skip Treatments
- 1 2 3 4 Negrini, S., Aulisa, A.G., Aulisa, L., Circo, A.B., Claude de Mauroy, J., Durmala, J., Grivas, T.B., Knott, P., Kotwicki, T., Maruyama, T., Minozzi, S., O’Brien, J.P., Papadopoulos,D., Rigo, M., Rivard, C.H., Romano, M., Wynne, J.H., Villagrasa, M., Weiss, H., Zaina, F. (2012). 2011 SOSORT guidelines: Orthopaedic and Rehabilitation treatment of idiopathic scoliosis during growth. Scoliosis, 7 (3), 1–35.
- ↑ Edery P.; Margaritte-Jeannin P.; Biot B.; Labalme A.; Bernard J.; Chastang J.; Kassai B.; Plais M.; Moldovan Fl.; Clerget-Darpoux F. (2011). "New disease gene location and high genetic heterogeneity in idiopathic scoliosis". European Journal of Human Genetics. 19: 865–869. doi:10.1038/ejhg.2011.31.
- ↑ Burwell, R.G. (2003). Aetiology of idiopathic scoliosis: current concepts. Pedriatric Rehabilitation, 6 (3–4), 137–170.
- ↑ Larson, N. (2011). Early onset scoliosis: What the primary care provider needs to know and implications for practice. Journal of the American Academy of Nurse Practitioners, 23, 392–403.
- ↑ Kamerlink, J., Quirno, M., Auerbach, J., Milby, A., Windsor, L., Dean, L., Dryer, J., Errico, T., Lonner, B. (2010). Hospital cost analysis of adolescent idiopathic scoliosis correction surgery in 125 consecutive cases. Journal of Bone & Joint Surgery, 92-A (5), 1097–1104.
- 1 2 3 4 5 6 7 Lovejoy OC (Jan 2005). "The natural history of human gait and posture: Part 1. Spine and pelvis." Gait & Posture 21 (1): 95–112.
- ↑ Harcourt-Smith, William E (2007). Handbook of Paleoanthropology. Chapter 5: Springer Berlin Heidelberg. pp. 1483–1518.
- ↑ Hunt, Kevin D (March 1994). "The evolution of human bipedality: ecology and functional morphology". Journal of Human Evolution. 26 (3): 182–202. doi:10.1006/jhev.1994.1011.
External links
| Wikimedia Commons has media related to Scoliosis. |
- Scoliosis at DMOZ
- Scoliosis Australia is a project of the Spine Society of Australia, an Affiliate of the Australian Orthopaedic Association. The website provides information about scoliosis.
- Early Onset Scoliosis is the abnormal, side-to-side curve of spine in children under 5 years old, often including children with congenital scoliosis (present at birth, with spine abnormalities) and infantile scoliosis (birth to 3 years).
- Questions and Answers about Scoliosis in Children and Adolescents - US National Institute of Arthritis and Musculoskeletal and Skin Diseases