Third-degree atrioventricular block
| Third-degree atrioventricular block | |
|---|---|
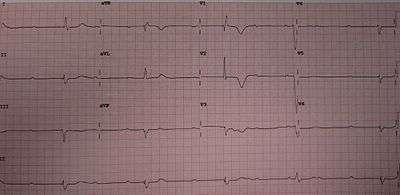 | |
| 12-lead ECG showing complete heart block | |
| Classification and external resources | |
| Specialty | cardiology |
| ICD-10 | I44.2 |
| ICD-9-CM | 426.0 |
| DiseasesDB | 10477 |
| eMedicine | emerg/235 |

Third-degree atrioventricular block (AV block), also known as complete heart block, is a medical condition in which the impulse generated in the sinoatrial node (SA node) in the atrium of the heart does not propagate to the ventricles.[1]
Because the impulse is blocked, an accessory pacemaker in the lower chambers will typically activate the ventricles. This is known as an escape rhythm. Since this accessory pacemaker also activates independently of the impulse generated at the SA node, two independent rhythms can be noted on the electrocardiogram (ECG).
- The P waves with a regular P-to-P interval (in other words, a sinus rhythm) represent the first rhythm.
- The QRS complexes with a regular R-to-R interval represent the second rhythm. The PR interval will be variable, as the hallmark of complete heart block is lack of any apparent relationship between P waves and QRS complexes.
Patients with third-degree AV block typically experience severe bradycardia (an abnormally-low measured heart rate), hypotension, and at times, hemodynamic instability.[2]
Cause
Many conditions can cause third-degree heart block, but the most common cause is coronary ischemia. Progressive degeneration of the electrical conduction system of the heart can lead to third-degree heart block. This may be preceded by first-degree AV block, second-degree AV block, bundle branch block, or bifascicular block. In addition, acute myocardial infarction may present with third-degree AV block.
An inferior wall myocardial infarction may cause damage to the AV node, causing third-degree heart block. In this case, the damage is usually transitory. Studies have shown that third-degree heart block in the setting of an inferior wall myocardial infarction typically resolves within 2 weeks.[3] The escape rhythm typically originates in the AV junction, producing a narrow complex escape rhythm.
An anterior wall myocardial infarction may damage the distal conduction system of the heart, causing third-degree heart block. This is typically extensive, permanent damage to the conduction system, necessitating a permanent pacemaker to be placed.[4] The escape rhythm typically originates in the ventricles, producing a wide complex escape rhythm.
Third-degree heart block may also be congenital and has been linked to the presence of lupus in the mother.[5] It is thought that maternal antibodies may cross the placenta and attack the heart tissue during gestation. The cause of congenital third-degree heart block in many patients is unknown. Studies suggest that the prevalence of congenital third-degree heart block is between 1 in 15,000 and 1 in 22,000 live births.
Hyperkalemia in those with previous cardiac disease[6] and Lyme disease can also result in third-degree heart block.[7]
Prognosis
The prognosis of patients with complete heart block is generally poor without therapy. Patients with 1st and 2nd degree heart block are usually asymptomatic.[8]
Treatment
Treatment in emergency situations ultimately involves electrical pacing. Pharmacological management of suspected beta-blocker overdose might be treated with glucagon, calcium channel blocker overdose treated with calcium chloride and digitalis toxicity treated with the digoxin immune Fab.[9]
Third-degree AV block can be treated by use of a dual-chamber artificial pacemaker.[10] This type of device typically listens for a pulse from the SA node via lead in the right atrium and sends a pulse via a lead to the right ventricle at an appropriate delay, driving both the right and left ventricles. Pacemakers in this role are usually programmed to enforce a minimum heart rate and to record instances of atrial flutter and atrial fibrillation, two common secondary conditions that can accompany third-degree AV block. Since pacemaker correction of third-degree block requires full-time pacing of the ventricles, a potential side effect is pacemaker syndrome, and may necessitate use of a biventricular pacemaker, which has an additional 3rd lead placed in a vein in the left ventricle, providing a more coordinated pacing of both ventricles.
The 2005 Joint European Resuscitation and Resuscitation Council (UK) guidelines[11] state that atropine is the first line treatment especially if there were any adverse signs, namely: 1) heart rate < 40 bpm, 2) systolic blood pressure < 100 mm Hg, 3) signs of heart failure, and 4) ventricular arrhythmias requiring suppression. If these fail to respond to atropine or there is a potential risk of asystole, transvenous pacing is indicated. The risk factors for asystole include 1) previous asystole, 2) complete heart block with wide complexes, and 3) ventricular pause for > 3 seconds. Mobitz Type 2 AV block is another indication for pacing.
As with other forms of heart block, secondary prevention may also include medicines to control blood pressure and atrial fibrillation, as well as lifestyle and dietary changes to reduce risk factors associated with heart attack and stroke.
See also
- Cardiac pacemaker
- Electrical conduction system of the heart
- Electrocardiogram (ECG)
- Atrioventricular block
- First-degree AV block
- Second-degree AV block
References
- ↑ "ECG Conduction Abnormalities". Retrieved 2009-01-07.
- ↑ "Heart Block". NHS Choices. National Health Service (UK). Retrieved 25 August 2015.
- ↑ Sclarovsky, S; Strasberg, B; Hirshberg, A; Arditi, A; Lewin, RF; Agmon, J (July 1984). "Advanced early and late atrioventricular block in acute inferior wall myocardial infarction.". American Heart Journal. 108 (1): 19–24. doi:10.1016/0002-8703(84)90539-8. PMID 6731277.
- ↑ Dorney, E (September 1981). "The role of pacemaker therapy in acute myocardial infarction.". Primary care. 8 (3): 509–17. PMID 7031733.
- ↑ Brucato, A; Previtali, E; Ramoni, V; Ghidoni, S (September 2010). "Arrhythmias presenting in neonatal lupus.". Scandinavian journal of immunology. 72 (3): 198–204. doi:10.1111/j.1365-3083.2010.02441.x. PMID 20696016.
- ↑ Sohoni A, Perez B, Singh A (2010). "Wenckebach Block due to Hyperkalemia: A Case Report". Emerg Med Int. 2010: 879751. doi:10.1155/2010/879751. PMC 3200192
 . PMID 22046534.
. PMID 22046534. - ↑ Forrester, JD; Mead, P (October 2014). "Third-degree heart block associated with lyme carditis: review of published cases.". Clinical Infectious Diseases. 59 (7): 996–1000. doi:10.1093/cid/ciu411. PMID 24879781.
- ↑ Edhag O, Swahn A (1976). "Prognosis of patients with complete heart block or arrhythmic syncope who were not treated with artificial pacemakers. A long-term follow-up study of 101 patients.". Acta Med Scand. 200 (6): 457–63. doi:10.1111/j.0954-6820.1976.tb08264.x. PMID 1015354.
- ↑ "Atrioventricular block, Treatment Options". BMJ Best Practice. BMJ (British Medical Journal). Retrieved 25 August 2015.
- ↑ Dretzke, J.; et al. "Compared to single chamber ventricular pacemakers, dual chamber pacemakers may reduce the incidence of complications in people with sick sinus syndrome and atrioventricular block". Cochrane reviews. Retrieved 25 August 2015.
- ↑ "Peri-arrest arrhythmias". Resuscitation guidelines. Resuscitation Council UK. Retrieved 25 August 2015.