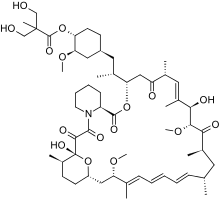
Temsirolimus
 | |
| Clinical data | |
|---|---|
| Trade names | Torisel |
| AHFS/Drugs.com | Monograph |
| MedlinePlus | a607071 |
| License data | |
| Pregnancy category | |
| Routes of administration | Intravenous |
| ATC code | L01XE09 (WHO) |
| Legal status | |
| Legal status | |
| Pharmacokinetic data | |
| Metabolism | Hepatic |
| Biological half-life | 17.3 hr (temsirolimus); 54.6 hr (sirolimus)[1] |
| Excretion | Urine (4.6%), faeces (78%)[1] |
| Identifiers | |
| |
| CAS Number |
162635-04-3 |
| PubChem (CID) | 6918289 |
| IUPHAR/BPS | 5892 |
| DrugBank |
DB06287 |
| ChemSpider |
21468899 |
| UNII |
624KN6GM2T |
| KEGG |
D06068 |
| ChEMBL |
CHEMBL1201182 |
| ECHA InfoCard | 100.211.882 |
| Chemical and physical data | |
| Formula | C56H87NO16 |
| Molar mass | 1030.28 |
| | |
Temsirolimus (CCI-779) is an intravenous drug for the treatment of renal cell carcinoma (RCC), developed by Wyeth Pharmaceuticals and approved by the U.S. Food and Drug Administration (FDA) in late May 2007,[2] and was also approved by the European Medicines Agency (EMEA) on November 2007. It is a derivative and prodrug of sirolimus and is sold as Torisel.
Mechanism of action
Temsirolimus is a specific inhibitor of mTOR and interferes with the synthesis of proteins that regulate proliferation, growth, and survival of tumor cells. Though temsirolimus shows activity on its own, it is also known to be converted to sirolimus (rapamycin) in vivo;[3] therefore, its activity may be more attributed to its metabolite rather than the prodrug itself (despite claims to the contrary by the manufacturer).[4] Treatment with temsirolimus leads to cell cycle arrest in the G1 phase, and also inhibits tumor angiogenesis by reducing synthesis of VEGF.[5]
mTOR (mammalian target of rapamycin) is a kinase enzyme inside the cell that collects and interprets the numerous and varied growth and survival signals received by tumor cells.[6] When the kinase activity of mTOR is activated, its downstream effectors, the synthesis of cell cycle proteins such as cyclin D and hypoxia-inducible factor-1a (HIF-1a) are increased. HIF-1a then stimulates VEGF.[7] Whether or not mTOR kinase is activated, determines whether the tumor cell produces key proteins needed for proliferation, growth, survival, and angiogenesis.[8]
mTOR is activated in tumor cells by various mechanisms including growth factor surface receptor tyrosine kinases, oncogenes, and loss of tumor suppressor genes. These activating factors are known to be important for malignant transformation and progression.[9] mTOR is particularly important in the biology of renal cancer (RCC) owing to its function in regulating HIF-1a levels. Mutation or loss of the von Hippel Lindau tumor-suppressor gene is common in RCC and is manifested by reduced degradation of HIF-1a. In RCC tumors, activated mTOR further exacerbates accumulation of HIF-1a by increasing synthesis of this transcription factor and its angiogenic target gene products.[10]
Efficacy
In an international Three-arm phase III study with 626 previously untreated, poor-prognosis patients, temsirolimus, interferon-α and the combination of both agents was compared. Median overall survival improved significantly in the temsirolimus group (10.9 months) compared with interferon-α group (7.3 months) and the combination group (8.4 months). Further studies are needed to determine the role of temsirolimus in the first-line treatment of patients with a more favorable prognosis, how it can be combined with other targeted agents and as sequential therapy with sunitinib or sorafenib.[11]
Adverse reactions
The toxicity profile is based on what was found in the phase III trial.[12]
- adverse reaction
- fatigue
- skin rash
- mucositis
- hematologic abnormalities
- hemoglobin decreased
- lymphocytes decreased
- laboratory abnormalities
- triglycerides increased
- glucose increased
- phosphorus decreased
Temsirolimus has been generally well tolerated in clinical settings by patients with advanced RCC. In patients with RCC, the adverse effect profile of temsirolimus is primarily metabolic in nature, with minimal impact on QoL compared with the commonly seen side-effects with oral multikinase inhibitors. Temsirolimus’ high level of specificity for mTOR likely contributes to the tolerability of temsirolimus. However, temsirolimus increases mortality in cancer patients.[13]
Lung toxicity
Temsirolimus is associated with lung toxicity, and the risk of developing this complication may be increased among subjects with abnormal pre-treatment pulmonary functions or history of lung disease.[14] The risk of interstitial lung disease is increased with temsirolimus doses greater than 25 mg, symptoms of which may include dry cough, fever, eosinophilia, chest pain, and dyspnea on exertion. Toxicity usually occurred early (within days to weeks) or late (months to years) after treatment.[15]
Dosing
The recommended dose of temsirolimus is 25 mg IV infused over 30–60 minutes once per week (Wyeth Pharmaceuticals, Inc., 2007). Weekly treatment may continue until disease progression or until patients experience intolerable side effects.
Although infusion reactions can occur while temsirolimus is being administered, most hypersensitivity reactions occurring on the same day as temsirolimus administration were not severe. Antihistamine pretreatment (e.g. 25–50 mg diphenhydramine, 30 minutes prior to administration) is recommended to minimize the risk of an allergic reaction.[12][15]
See also
References
- 1 2 Temsirolimus Drug Monograph. CCO Formulary - June 2014: Cancer Care Ontario. p. 2.
- ↑ "FDA Approves New Drug for Advanced Kidney Cancer" (Press release). Food and Drug Administration. May 30, 2007. Retrieved October 15, 2013.
- ↑ Hastings, Kenneth. "Pharmacology Review, Application Number 22-088" (PDF). FDA. Retrieved 7 March 2015.
- ↑ "Temsirolimus Monograph for Professionals". Drugs.com. Drugs.com. Retrieved 7 March 2015.
- ↑ Wan, Xiaolin; Shen, Na; Mendoza, Arnulfo; Khanna, Chand; Helman, Lee J. (2006). "CCI-779 Inhibits Rhabdomyosarcoma Xenograft Growth by an Antiangiogenic Mechanism Linked to the Targeting of mTOR/Hif-1α/VEGF Signaling". Neoplasia. 8 (5): 394–401. doi:10.1593/neo.05820. PMC 1592447
 . PMID 16790088.
. PMID 16790088. - ↑ Rubio-Viqueira, B; Hidalgo, M (2006). "Targeting mTOR for cancer treatment". Current Opinion in Investigational Drugs. 7 (6): 501–12. PMID 16784020.
- ↑ Hudson, C. C.; Liu, M.; Chiang, G. G.; Otterness, D. M.; Loomis, D. C.; Kaper, F.; Giaccia, A. J.; Abraham, R. T. (2002). "Regulation of Hypoxia-Inducible Factor 1 Expression and Function by the Mammalian Target of Rapamycin". Molecular and Cellular Biology. 22 (20): 7004–14. doi:10.1128/MCB.22.20.7004-7014.2002. PMC 139825. PMID 12242281.
- ↑ Del Bufalo, D.; Ciuffreda, L; Trisciuoglio, D; Desideri, M; Cognetti, F; Zupi, G; Milella, M (2006). "Antiangiogenic Potential of the Mammalian Target of Rapamycin Inhibitor Temsirolimus". Cancer Research. 66 (11): 5549–54. doi:10.1158/0008-5472.CAN-05-2825. PMID 16740688.
- ↑ Dancey, Janet E. (2006). "Therapeutic targets: MTOR and related pathways". Cancer Biology & Therapy. 5 (9): 1065. doi:10.4161/cbt.5.9.3175.
- ↑ Thomas, George V; Tran, Chris; Mellinghoff, Ingo K; Welsbie, Derek S; Chan, Emily; Fueger, Barbara; Czernin, Johannes; Sawyers, Charles L (2005). "Hypoxia-inducible factor determines sensitivity to inhibitors of mTOR in kidney cancer". Nature Medicine. 12 (1): 122–7. doi:10.1038/nm1337. PMID 16341243.
- ↑ Hudes, Gary; Carducci, Michael; Tomczak, Piotr; Dutcher, Janice; Figlin, Robert; Kapoor, Anil; Staroslawska, Elzbieta; Sosman, Jeffrey; McDermott, David; Bodrogi, István; Kovacevic, Zoran; Lesovoy, Vladimir; Schmidt-Wolf, Ingo G.H.; Barbarash, Olga; Gokmen, Erhan; O'Toole, Timothy; Lustgarten, Stephanie; Moore, Laurence; Motzer, Robert J.; Global Arcc, Trial (2007). "Temsirolimus, Interferon Alfa, or Both for Advanced Renal-Cell Carcinoma". New England Journal of Medicine. 356 (22): 2271–81. doi:10.1056/NEJMoa066838. PMID 17538086.
- 1 2 Bellmunt, J.; Szczylik, C.; Feingold, J.; Strahs, A.; Berkenblit, A. (2008). "Temsirolimus safety profile and management of toxic effects in patients with advanced renal cell carcinoma and poor prognostic features". Annals of Oncology. 19 (8): 1387–92. doi:10.1093/annonc/mdn066. PMID 18385198.
- ↑ Choueiri, T. K.; Je, Y.; Sonpavde, G.; Richards, C. J.; Galsky, M. D.; Nguyen, P. L.; Schutz, F.; Heng, D. Y.; Kaymakcalan, M. D. (2013). "Incidence and risk of treatment-related mortality in cancer patients treated with the mammalian target of rapamycin inhibitors". Annals of Oncology. 24 (8): 2092–7. doi:10.1093/annonc/mdt155. PMID 23658373. Lay summary – MedPage Today (Feb 17, 2013).
- ↑ Duran, I.; Siu, L.L.; Oza, A.M.; Chung, T.-B.; Sturgeon, J.; Townsley, C.A.; Pond, G.R.; Seymour, L.; Niroumand, M. (2006). "Characterisation of the lung toxicity of the cell cycle inhibitor temsirolimus". European Journal of Cancer. 42 (12): 1875–80. doi:10.1016/j.ejca.2006.03.015. PMID 16806903.
- 1 2 Temsirolimus Drug Monograph. CCO Formulary - June 2014: Cancer Care Ontario. p. 4.