Streptococcus mutans
| Streptococcus mutans | |
|---|---|
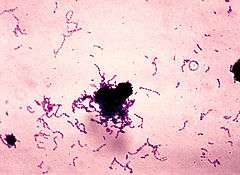 | |
| Stain of S. mutans in thioglycollate broth culture. | |
| Scientific classification | |
| Kingdom: | Bacteria |
| Phylum: | Firmicutes |
| Class: | Coccus |
| Order: | Lactobacillales |
| Family: | Streptococcaceae |
| Genus: | Streptococcus |
| Species: | S. mutans |
| Binomial name | |
| Streptococcus mutans Clarke 1924 | |
Streptococcus mutans is a facultatively anaerobic, gram-positive coccus (round bacterium) commonly found in the human oral cavity and is a significant contributor to tooth decay.[1][2] It is part of the "streptococci" (plural, non-italic lowercase), an informal general name for all species in the genus Streptococcus.The microbe was first described by J Kilian Clarke in 1924.[3]
This bacterium, along with the closely related species Streptococcus sobrinus, can cohabit the mouth: Both contribute to oral disease, and the expense of differentiating them in laboratory testing is often not clinically necessary. Therefore, for clinical purposes they are often considered together as a group, called the mutans streptococci (plural, non-italic due to it being an informal group name).[4] This grouping of similar bacteria with similar tropism can also be seen in the viridans streptococci, another group of Streptococcus species.
Ecology
S. mutans is naturally present in the human oral microbiota, along with at least 25 other species of oral streptococci. The taxonomy of these bacteria remains tentative.[5] Different areas of the oral cavity present different ecological niches, and each species has specific properties for colonizing different oral sites. S. mutans is most prevalent on the pits and fissures, constituting 39% of the total streptococci in the oral cavity. Fewer S. mutans bacteria are found on the buccal surface (2–9%).[6]
Oral streptococci have both harmless and harmful bacteria. However, under special conditions commensal streptococci can become opportunistic pathogens, initiating disease and damaging the host. Imbalances in the microbial biota can initiate oral diseases.
Role in disease
Tooth decay
Early colonizers of the tooth surface are mainly Neisseria spp. and streptococci, including S. mutans. The growth and metabolism of these pioneer species changes local environmental conditions (e.g., Eh, pH, coaggregation, and substrate availability), thereby enabling more fastidious organisms to further colonize after them, forming dental plaque.[7] Along with S. sobrinus, S. mutans plays a major role in tooth decay, metabolizing sucrose to lactic acid[2] using the enzyme glucansucrase.[8] The acidic environment created in the mouth by this process is what causes the highly mineralized tooth enamel to be vulnerable to decay. S. mutans is one of a few specialized organisms equipped with receptors that improve adhesion to the surface of teeth. Sucrose is used by S. mutans to produce a sticky, extracellular, dextran-based polysaccharide that allows them to cohere, forming plaque. S. mutans produces dextran via the enzyme dextransucrase (a hexosyltransferase) using sucrose as a substrate in the following reaction:
- n sucrose → (glucose)n + n fructose
Sucrose is the only sugar that bacteria can use to form this sticky polysaccharide.[1]
However, many other sugars—glucose, fructose, lactose—can also be digested by S. mutans, but they produce lactic acid as an end product. The combination of plaque and acid leads to dental decay.[9] Due to the role S. mutans plays in tooth decay, many attempts have been made to create a vaccine for the organism. So far, such vaccines have not been successful in humans.[10] Recently, proteins involved in the colonization of teeth by S. mutans have been shown to produce antibodies that inhibit the cariogenic process.[11] A molecule recently synthesized at Yale University and the University of Chile, called Keep 32, is supposed to be able to kill S. mutans. Another candidate is a peptide called C16G2, synthesised at UCLA.
It is believed that Streptococcus mutans acquired the gene that enables it to produce biofilms through horizontal gene transfer with other lactic acid bacterial species, such as Lactobacillus.[12]
Life in the oral cavity
Surviving in the oral cavity, S. mutans is the primary causal agent and the pathogenic species responsible for dental caries (tooth decay or cavities) specifically in the initiation and development stages.
Dental plaque, typically the precursor to tooth decay, contains more than 600 different microorganisms, contributing to the oral cavity’s overall dynamic environment that frequently undergoes rapid changes in pH, nutrient availability, and oxygen tension. Dental plaque adheres to the teeth and consists of bacterial cells, while plaque is the biofilm on the surfaces of the teeth. Dental plaque and S. mutans is frequently exposed to "toxic compounds" from oral healthcare products, food additives, and tobacco.
While S. mutans grows in the biofilm, cells maintain a balance of metabolism that involves production and detoxification. Biofilm is an aggregate of microorganisms in which cells adhere to each other or a surface. Bacteria in the biofilm community can actually generate various toxic compounds that interfere with the growth of other competing bacteria.
S. mutans has over time developed strategies to successfully colonize and maintain a dominant presence in the oral cavity. The oral biofilm is continuously challenged by changes in the environmental conditions. In response to such changes, the bacterial community evolved with individual members and their specific functions to survive in the oral cavity. S. mutans has been able to evolve from nutrition-limiting conditions to protect itself in extreme conditions.[13] Streptococci represent 20% of the oral bacteria and actually determine the development of the biofilms. Although S. mutans can be antagonized by pioneer colonizers, once they become dominant in oral biofilms, dental caries can develop and thrive.[13]
Cariogenic potential
The causative agent of dental caries is associated with its ability to metabolize various sugars, form a robust biofilm, produce an abundant amount of lactic acid, and thrive in the acid environment it generates.[14]
Dental caries is a dental biofilm-related oral disease associated with increased consumption of dietary sugar and fermentable carbohydrates. When dental biofilms remain on tooth surfaces, along with frequent exposure to sugars, acidogenic bacteria (members of dental biofilms) will metabolize the sugars to organic acids. Persistence of this acidic condition encourages the proliferation of acidogenic and aciduric bacteria as a result of their ability to survive at a low-pH environment. The low-pH environment in the biofilm matrix erodes the surface of the teeth and begins the "initiation" of the dental caries.[14] If the adherence of S. mutans to the surface of teeth or the physiological ability (acidogenity and aciduricity) of S. mutans in dental biofilms can be reduced or eliminated, the acidification potential of dental biofilms and later cavity formations can be decreased.[14]
Susceptibility to disease varies between individuals and immunological mechanisms have been proposed to confer protection or susceptibility to the disease. These mechanisms have yet to be fully elucidated but it seems that while antigen presenting cells are activated by S. mutans in vitro, they fail to respond in vivo. Immunological tolerance to S. mutans at the mucosal surface may make individuals more prone to colonisation with S. mutans and therefore increase susceptibility to dental caries.[15]
In children
S. mutans is often acquired in the oral cavity subsequent to tooth eruption, but has also been detected in the oral cavity of predentate children. It is generally, but not exclusively, transmitted via vertical transmission from caregiver (generally the mother) to child.[16][17]
Cardiovascular disease
S. mutans is implicated in the pathogenesis of certain cardiovascular diseases, and is the most prevalent bacterial species detected in extirpated heart valve tissues, as well as in atheromatous plaques, with an incidence of 68.6% and 74.1%, respectively.[18]
Prevention and treatment
Practice of good oral hygiene including daily brushing, flossing and the use of appropriate mouthwash can significantly reduce the number of oral bacteria, including S. mutans and inhibit their proliferation. S. mutans often live in dental plaque, hence mechanical removal of plaque is an effective way of getting rid of them.[19] However, there are some remedies used in the treatment of oral bacterial infection, in conjunction with mechanical cleaning. These include Fluoride, which has a direct inhibitory effect on the enolase enzyme, as well as Chlorhexidine, which works presumably by interfering with bacterial adherence.
Other common preventative measures center on reducing sugar intake. One way this is done is with sugar replacements such as Xylitol, which cannot be metabolized into sugars which normally enhance S. mutans growth.[20][21] Various other natural remedies have been suggested or studied to a degree, including deglycyrrhizinated licorice root extract,[22][23] Tea tree oil,[24] Macelignan (found in nutmeg),[25] Curcuminoids (the main components of turmeric),[26] and eugenol (found in bay leaves, cinnamon leaves and cloves). Additionally various teas have been tested for activity against S. mutans and other dental benefits.[27] [28] [29][30][31] However, none of these remedies have been subject to clinical trials or are recommended by mainstream dental health groups to treat S. mutans.
Survival under stressful conditions
Conditions in the oral cavity are diverse and complex, frequently changing from one extreme to another. Thus, to survive in the oral cavity, S. mutans must tolerate rapidly harsh environmental fluctuations and exposure to various antimicrobial agents to survive.[13] Transformation is a bacterial adaptation involving the transfer of DNA from one bacterium to another through the surrounding medium. Transformation is a primitive form of sexual reproduction. For a bacterium to bind, take up, and recombine exogenous DNA into its chromosome, it must enter a special physiological state termed “competence”. In S. mutans, a peptide pheromone quorum-sensing signaling system controls genetic competence.[32] This system functions optimally when the S. mutans cells are in crowded biofilms.[33] S. mutans cells growing in a biofilm are transformed at a rate 10- to 600-fold higher than single cells growing under uncrowded conditions (planktonic cells).[32] Induction of competence appears to be an adaptation for repairing DNA damage caused by crowded, stressful conditions.[34]
Evolution
Three key traits have evolved in S. mutans and increased its virulence by enhancing its adaptability to the oral cavity: increased organic acid production, the capacity to form biofilms on the hard surfaces of teeth, and the ability to survive and thrive in a low pH environment.[35]
During its evolution, S. mutans acquired the ability to increase the amount of carbohydrates it could metabolize, and consequently more organic acid was produced as a byproduct.[36] This is significant in the formation of dental caries because increased acidity in the oral cavity amplifies the rate of demineralization of the tooth, which leads to carious lesions.[37] It is thought that the trait evolved in S. mutans via lateral gene transfer with another bacterial species present in the oral cavity. There are several genes, SMU.438 and SMU.1561, involved in carbohydrate metabolism that are up-regulated in S. mutans. These genes possibly originated from Lactococcus lactis and S. gallolyticus, respectively.[36]
Another instance of lateral gene transfer is responsible for S. mutans’ acquisition of the glucosyltransferase (GTF) gene, which allows the bacteria to produce polysaccharides from sucrose. These sticky polysaccharides are responsible for the bacteria’s ability to aggregate with one another and adhere to tooth enamel, i.e. to form biofilms. The GTF genes found in S. mutans most likely are derived from other anaerobic bacteria found in the oral cavity, such as Lactobacillus or Leuconostoc. Additionally, the GTF genes in S. mutans display homology with similar genes found in Lactobacillus and Leuconostoc. The common ancestral gene is believed to have been used for hydrolysis and linkage of carbohydrates.[38]
The third trait that evolved in S. mutans is its ability to not only survive, but also thrive in acidic conditions. This trait gives S. mutans a selective advantage over other members of the oral microbiota. As a result, S. mutans could outcompete other species, and occupy additional regions of the mouth, such as advanced dental plaques, which can be as acidic as pH 4.0.[37] Natural selection is most likely the primary evolutionary mechanisms responsible for this trait.
In discussing the evolution of S. mutans, it is imperative to include the role humans have played and the co-evolution that has occurred between the two species. As humans evolved anthropologically, the bacteria evolved biologically. It is widely accepted that the advent of agriculture in early human populations provided the conditions S. mutans needed to evolve into the virulent bacteria it is today. Agriculture introduced fermented foods, as well as more carbohydrate rich foods, into the diets of historic human populations. These new foods introduced new bacteria to the oral cavity and created new environmental conditions. For example, Lactobacillus or Leuconostoc are typically found in foods such as yogurt and wine. Also, consuming more carbohydrates increased the amount of sugars available to S. mutans for metabolism and lowered the pH of the oral cavity. This new acidic habitat would select for those bacteria that could survive and reproduce at a lower pH.[36]
Another significant change to the oral environment occurred during the Industrial Revolution. More efficient refinement and manufacturing of foodstuffs increased the availability and amount of sucrose consumed by humans. This provided S. mutans with more energy resources, and thus exacerbated an already rising rate of dental caries.[38] Refined sugar is pure sucrose, the only sugar that can be converted to sticky glucans, allowing bacteria to form a thick, strongly adhering plaque.[39]
See also
References
- 1 2 Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. ISBN 0-8385-8529-9.
- 1 2 Loesche WJ (1996). "Ch. 99: Microbiology of Dental Decay and Periodontal Disease". In Baron S; et al. Baron's Medical Microbiology (4th ed.). University of Texas Medical Branch. ISBN 0-9631172-1-1. PMID 21413316.
- ↑ Clarke, J. Kilian (1924). "On the Bacterial Factor in the Ætiology of Dental Caries". British Journal of Experimental Pathology. 5 (3): 141–7. PMC 2047899
 .
. - ↑ Newcastle University Dental School. "Streptococcus mutans and the mutans streptococci. In: The Oral Environment, online tutorial". Retrieved 2013-11-04.
- ↑ Nicolas, Guillaume G.; Lavoie, Marc C. (2011). "Streptococcus mutans et les streptocoques buccaux dans la plaque dentaire". Canadian Journal of Microbiology. 57 (1): 1–20. doi:10.1139/W10-095. PMID 21217792.
- ↑ Ikeda, T.; Sandham, H.J. (1971). "Prevalence of Streptococcus mutans on various tooth surfaces in negro children". Archives of Oral Biology. 16 (10): 1237–40. doi:10.1016/0003-9969(71)90053-7. PMID 5289682.
- ↑ Vinogradov AM, Winston M, Rupp CJ, Stoodley P; Winston; Rupp; Stoodley (2004). "Rheology of biofilms formed from the dental plaque pathogen Streptococcus mutans". Biofilms. 1: 49–56. doi:10.1017/S1479050503001078.
- ↑ http://blogs.discovermagazine.com/discoblog/2010/12/08/dental-researchers-to-mouth-bacteria-dont-get-too-attached/
- ↑ Madigan M, Martinko J (editors). (2005). Brock Biology of Microorganisms (11th ed.). Prentice Hall. ISBN 0-13-144329-1.
- ↑ Klein, J.P.; Scholler, M. (December 1998). "Recent Advances in the Development of a Streptococcus mutans Vaccine". European Journal of Epidemiology. 4 (4): 419–25. doi:10.1007/BF00146392. JSTOR 3521322. PMID 3060368.
- ↑ Hajishengallis G, Russell MW (2008). "Molecular Approaches to Vaccination against Oral Infections". Molecular Oral Microbiology. Caister Academic Press. ISBN 978-1-904455-24-0.
- ↑ Hoshino, T.; Fujiwara, T.; Kawabata, S. (2012). "Evolution of Cariogenic Character in Streptococcus mutans: Horizontal Transmission of Glycosyl Hydrolase Family 70 Genes". Scientific Reports. 2: 518–525. doi:10.1038/srep00518.
- 1 2 3 Biswas, S; Biswas, I (2011). "Role of VltAB, an ABC transporter complex, in viologen tolerance in Streptococcus mutans". Antimicrobial Agents and Chemotherapy. 55 (4): 1460–9. doi:10.1128/AAC.01094-10. PMC 3067168. PMID 21282456.
- 1 2 3 Argimón, S; Caufield, PW (2011). "Distribution of putative virulence genes in Streptococcus mutans strains does not correlate with caries experience". Journal of clinical microbiology. 49 (3): 984–92. doi:10.1128/JCM.01993-10. PMC 3067729. PMID 21209168.
- ↑ Butcher, JP; Malcolm, J; Benson, RA; Deng, DM; Brewer, JM; Garside, P; Culshaw, S (2011). "Effects of Streptococcus mutans on dendritic cell activation and function". Journal of dental research. 90 (10): 1221–7. doi:10.1177/0022034511412970. PMID 21690565.
- ↑ Berkowitz, RJ (2006). "Mutans streptococci: acquisition and transmission". Pediatric dentistry. 28 (2): 106–9; discussion 192–8. PMID 16708784.
- ↑ da Silva Bastos Vde, A; Freitas-Fernandes, LB; Fidalgo, TK; Martins, C; Mattos, CT; de Souza, IP; Maia, LC (February 2015). "Mother-to-child transmission of Streptococcus mutans: a systematic review and meta-analysis.". Journal of dentistry. 43 (2): 181–91. doi:10.1016/j.jdent.2014.12.001. PMID 25486222.
- ↑ Nakano, K; Inaba, H; Nomura, R; Nemoto, H; Takeda, M; Yoshioka, H; Matsue, H; Takahashi, T; et al. (2006). "Detection of cariogenic Streptococcus mutans in extirpated heart valve and atheromatous plaque specimens". Journal of clinical microbiology. 44 (9): 3313–7. doi:10.1128/JCM.00377-06. PMC 1594668. PMID 16954266.
- ↑ Finkelstein, P; Yost, KG; Grossman, E (1990). "Mechanical devices versus antimicrobial rinses in plaque and gingivitis reduction". Clinical preventive dentistry. 12 (3): 8–11. PMID 2083478.
- ↑ Ly, KA; Milgrom, P; Rothen, M (2006). "Xylitol, sweeteners, and dental caries". Pediatric Dentistry. 28 (2): 154–63. PMID 16708791.
- ↑ Heinsohn, Torben (2013). "Welchen Einfluss haben Xylit-haltige Kaugummis auf die Mundflora? Entwicklung eines quantitativen Testes zum Nachweis von Streptococcus mutans auf Basis der "Real-time"-quantitativen Polymerase-Kettenreaktion" [Xylitol-containing chewing gum and the oral bacterial flora. Development of a Quantitative Test for Streptococcus mutans on the Basis of the Real-time Quantitative Polymerase Chain Reaction] (PDF). Junge Wissenschaft (Young Researcher) (in German). 97: 18–30. Retrieved 23 January 2015.
- ↑ Ahn, S; Cho, E; Kim, H; Park, S; Lim, Y; Kook, J (December 2012). "The antimicrobial effects of deglycyrrhizinated licorice root extract on Streptococcus mutans UA159 in both planktonic and biofilm cultures". Anaerobe. 18 (6): 590–596. doi:10.1016/j.anaerobe.2012.10.005. ISSN 1075-9964. PMID 23123832. Retrieved 13 March 2014.
- ↑ Hu, Chu-hong; He, Jian; Eckert, Randal; Wu, Xiao-yang; Li, Li-na; Tian, Yan; Lux, Renate; Shuffer, Justin A; Gelman, Faina; Mentes, Janet; Spackman, Sue; Bauer, Janet; Anderson, Maxwell H; Shi, Wen‐yuan (2011). "Development and evaluation of a safe and effective sugar-free herbal lollipop that kills cavity-causing bacteria". International journal of oral science. 3 (1): 13–20. doi:10.4248/IJOS11005. PMID 21449211.
- ↑ Carson, CF; Hammer, KA; Riley, TV (2006). "Melaleuca alternifolia (Tea Tree) oil: A review of antimicrobial and other medicinal properties". Clinical Microbiology Reviews. 19 (1): 50–62. doi:10.1128/CMR.19.1.50-62.2006. PMC 1360273. PMID 16418522.
- ↑ Yanti; Rukayadi, Y; Kim, KH; Hwang, JK (2008). "In vitro anti-biofilm activity of macelignan isolated from Myristica fragrans Houtt. Against oral primary colonizer bacteria". Phytotherapy research : PTR. 22 (3): 308–12. doi:10.1002/ptr.2312. PMID 17926328.
- ↑ Pandit, Santosh; Kim, Hye-Jin; Kim, Jeong-Eun; Jeon, Jae-Gyu (2011). "Separation of an effective fraction from turmeric against Streptococcus mutans biofilms by the comparison of curcuminoid content and anti-acidogenic activity". Food Chemistry. 126 (4): 1565–70. doi:10.1016/j.foodchem.2010.12.005.
- ↑ Subramaniam, P.; Eswara, U.; Maheshwar Reddy, K. R. (Jan–Feb 2012). "Effect of different types of tea on Streptococcus mutans: an in vitro study". Indian J Dent Res. 23 (1): 43–8. doi:10.4103/0970-9290.99037. PMID 22842248.
- ↑ Wahhida, Shumi; Aktar, Hossain; Dong-June, Park; Sungsu, Park (September 2014). "Inhibitory effects of green tea polyphenol epigallocatechin gallate (EGCG) on exopolysaccharide production by Streptococcus mutans under microfluidic conditions". BioChip Journal. 8 (3): 179–186. doi:10.1007/s13206-014-8304-y.
- ↑ Sangameshwar, M.; Vanishree, M.; Surekha, R.; Santosh, Hunasgi; Anila, K.; Vardendra, Manvikar (Jan–Mar 2014). "Effect of Green Tea on Salivary Ph and Streptococcus Mutans Count in Healthy Individuals". International Journal of Oral and Maxillofacial Pathology. 5 (1): 13–16. ISSN 2231-2250.
- ↑ Hala Awadalla; et al. (December 2009). "A pilot study of the role of green tea use on oral health". International Journal of Dental Hygiene. 9 (2): 110–116. doi:10.1111/j.1601-5037.2009.00440.x.
- ↑ Stauder, Monica; Papetti, Adele; Daglia, Maria; Vezzulli, Luigi; Gazzani, Gabriella; Varaldo, Pietro E.; Pruzzo, Carla (2010). "Inhibitory Activity by Barley Coffee Components Towards Streptococcus Mutans Biofilm". Current Microbiology. 61 (5): 417–21. doi:10.1007/s00284-010-9630-5. PMID 20361189.
- 1 2 Li YH, Lau PC, Lee JH, Ellen RP, Cvitkovitch DG; Lau; Lee; Ellen; Cvitkovitch (February 2001). "Natural genetic transformation of Streptococcus mutans growing in biofilms". J. Bacteriol. 183 (3): 897–908. doi:10.1128/JB.183.3.897-908.2001. PMC 94956. PMID 11208787.
- ↑ Aspiras MB, Ellen RP, Cvitkovitch DG; Ellen; Cvitkovitch (September 2004). "ComX activity of Streptococcus mutans growing in biofilms". FEMS Microbiol. Lett. 238 (1): 167–74. doi:10.1016/j.femsle.2004.07.032. PMID 15336418.
- ↑ Michod RE, Bernstein H, Nedelcu AM; Bernstein; Nedelcu (May 2008). "Adaptive value of sex in microbial pathogens". Infect. Genet. Evol. 8 (3): 267–85. doi:10.1016/j.meegid.2008.01.002. PMID 18295550. as PDF
- ↑ Banas, J. A.; Miller, J. D.; Fuschino, M. E.; Hazlett, K. R. O.; Toyofuku, W.; Porter, K. A.; Florczyk, M. A.; McDonough, K. A.; Michalek, S. M. (2007). "Evidence that accumulation of mutants in a biofilm reflects natural selection rather than stress-induced adaptive mutation". Applied and Environmental Microbiology. 73 (1): 357–361. doi:10.1128/aem.02014-06.
- 1 2 3 Cornejo, O. E.; Lefébure, T.; Bitar, P.D. Pavinski; Lang, P.; Richards, V. P.; Eilertson, K.; Do, T.; Beighton, D.; Zeng, L.; Ahn, S. J.; Burne, R. A.; Siepel, A.; Bustamante, C. D.; Stanhope, M. J. (2012). "Evolutionary and population genomics of the cavity causing bacteria Streptococcus mutans". Mol. Biol. Evol. 30 (4): 881–893. doi:10.1093/molbev/mss278.
- 1 2 Takahashi, N.; Nyvad, B. (2010). "The role of bacteria in the caries process: Ecological perspectives". Journal of Dental Research. 90 (3): 294–303. doi:10.1177/0022034510379602.
- 1 2 Hoshino, T.; Fujiwara, T.; Kawabata, S. (2012). "Evolution of cariogenic character in Streptococcus mutans: Horizontal transmission of glycosyl hydrolase family 70 genes". Scientific Reports. 2: 518–524. doi:10.1038/srep00518.
- ↑ Darlington, W. (August 1979). Metabolism of sucrose by Stepococcus sanguis 804 (NCTC 10904) and its relevance to the oral environment (Ph.D Thesis). University of Glasgow.
External links
- MCHoralhealth.org
- Type strain of Streptococcus mutans at BacDive - the Bacterial Diversity Metadatabase