Spinal cord stimulator
| Spinal cord stimulator | |
|---|---|
| Intervention | |
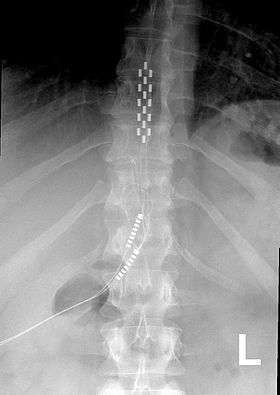 Anterior view X-ray of a spinal cord stimulator (SCS) implanted in the thoracic spine |
A spinal cord stimulator is a device used to exert pulsed electrical signals to the spinal cord to control chronic pain. Further applications are in motor disorders. The lumbar spinal cord is a preferred target for the control of spinal spasticity[1][2] or augmentation of standing and stepping capabilities.[3][4][5][6] Spinal cord stimulation (SCS), in the simplest form, consists of stimulating electrodes, implanted in the epidural space, an electrical pulse generator, implanted in the lower abdominal area or gluteal region, conducting wires connecting the electrodes to the generator, and the generator remote control. SCS has notable analgesic properties and, at the present, is used mostly in the treatment of failed back surgery syndrome, complex regional pain syndrome and refractory pain due to ischemia.
Medical uses
The most common use of SCS is failed back surgery syndrome (FBSS) in the United States and peripheral ischemic pain in Europe.
FBSS, classified as mixed pain syndrome (neuropathic and nociceptive), is the persistent or recurrent pain, mainly involving the lower back and/or legs after successful spinal surgery. It affects about 40% of patients who undergo spinal surgeries. Several studies showed overall efficacy of the SCS for FBSS.[7][8][9][10][11]
SCS is also indicated in the treatment of inoperable ischemic limb pain.[12] Furthermore, this technique is studied in various applications. For instance, it has been shown to modulate the function of sympathetic nervous system and increase norepinephrine release in refractory angina pectoris,[13] decreasing the probability of angina attack. SCS units have been used to treat patients with frequent migraines. The electrodes are implanted in the bilateral suboccipital region.[14] See[15] and[16] for a more complete list and references of further applications.
Advantages and disadvantages
SCS is analgesia on demand. It is a useful option when other forms of therapy fail. It reduces pain medication and side effects. It is effective in about 50–70% cases. It is an invasive procedure, so it can have associated complications such as infection, bleeding, and dural puncture. It has the risk of disconnection or equipment failure.[15]
SCS interaction with diathermy, pacemakers, MRI and therapeutic ultrasound can result in unexpected changes in stimulation, serious patient injury or death. It can also lead to failure of the device.[15]
Complications
Complications with SCS range from simple easily correctable problems to devastating paralysis, nerve injury and death. However, in a 7-year follow-up, the overall complication rate was 5-18%. The most common complications include lead migration, lead breakage, and infection. Other complications include haematomas (subcutaneous or epidural), cerebrospinal fluid (CSF) leak, post dural puncture headache, discomfort at pulse generator site, seroma and transient paraplegia. Hardware-related complications such as electrode migration, fractured electrodes, and rotation of pulse generator are also reported.[16]
Mechanism of action
The neurophysiologic mechanisms of action of spinal cord stimulation are not completely understood. Linderoth and others[17][18] have noted that the mechanism of analgesia when SCS is applied in neuropathic pain states may be very different from that involved in analgesia due to limb ischemia. In neuropathic pain states, experimental evidence show that SCS alters the local neurochemistry in dorsal horn, suppressing the hyperexcitability of the neurons. Specifically, there is some evidence for increased levels of GABA release, serotonin, and perhaps suppression of levels of some excitatory amino acids, including glutamate and aspartate. In the case of ischemic pain, analgesia seems to derive from restoration of the oxygen demand supply.[16] This effect could be mediated by inhibition of the sympathetic system, although vasodilation is another possibility. It is also probable that a combination of the two above mentioned mechanisms is involved.[15]
Technical consideration
Equipment
SCS, in simplest form, consists of a pulse generator with its remote controls, implanted stimulating electrodes and conducting wires connecting the electrodes to the generator.[15]
Generator
The generator, implanted subcutaneously, could be a complete pulse generator module with its own battery or only a radio frequency (RF) receiver. The former case, usually called implantable pulse generator or IPG, has a battery of its own and could come with rechargeable battery which can be charged externally via a wireless power charger so that it does not need to be replaced surgically when it loses charge.
The RF receiver on the other hand is externally driven by a transmitter from which it gets its power and pulses. This external transmitter has a battery which can be easily replaced. RF receivers have traditionally been used for patients who require high power settings that would quickly deplete a primary-cell IPG.[15]
The patient is also provided with a remote control to turn on and off the stimulator, and depending on the device and the surgeon’s preference, can change the programming of the stimulation patterns. The surgeon has a programming device that could be used to modify a wide range of stimulation settings of the RF generator.[15]
Various current, voltage and waveforms configurations are possible. SC stimulators come in constant current, variable voltage or constant voltage, variable current.[15]
Electrodes
The electrodes, which consist of an array of leads, could be percutaneous type or paddle type. Percutaneous electrodes are easier to insert in comparison with paddle type, which are inserted via incision over spinal cord and laminectomy.[16]

Insertion procedures and techniques
SCS procedure involves careful placement of electrodes in the epidural space, a trial period (which takes between 5–7 days), and, if the results of pain relieving was satisfactory in the trial period, anchoring the electrodes to the interspinal ligaments, positioning and implantation of the pulse generator, tunneling and connection of the connecting wires, programming the system for the special pattern of stimulation and performing required postoperative cares.[15]
Selecting the level of stimulation
The representation of the dermatomal level in the dorsal columns of the spinal cord is much higher than the corresponding vertebral level. For instance, the sweet spot for sciatic pain (dermatomal level L5/S1) is around T10 nerve.[15] See dermatome and Spinal cord segments.
Electrodes selection
For the SCS to be effective, the area of paresthesia must overlap the area of pain. Selection of leads depends on which arrangement will give the best paresthesia coverage to the painful area.
Generator implant
The IPG or the RF unit is usually implanted in the lower abdominal area or in the posterior superior gluteal region. It should be in a location that patients can access with their dominant hand for adjustment of their settings with the patient-held remote control. The decision to use a fully implantable IPG or an RF unit depends on several considerations. If the patient’s pain pattern requires the use of many electrodes with high power settings, an RF unit should be used. The IPG battery life will largely depend on the power settings utilized, but the newer IPG units will generally last several years at average power settings.[15]

Programming
Programming involves selecting the electrode stimulating configuration, adjusting the amplitude, width and frequency of electrical pulses. Amplitude indicates the intensity of stimulation. This is delivered in milliamperes or volts depending on the system used. Lower voltage or current is chosen for peripheral nerves and paddle leads. Pulse width usually varies from 100 to 400 us. Widening the pulse width will also broaden the area of paraesthesia. Frequency of pulse wave is usually between 20 and 120 hertz. It is an individual preference: some patients choose low frequency beating sensation whereas others prefer high frequency buzzing.[15]
Selection of lowest possible setting on all parameters is important in conserving battery life in non-rechargeable models of SCS. Cycling of stimulation is also employed to save battery life. Changing of stimulator program may have to be undertaken during the course of therapy and follow-up.[15]
Patient selection
Appropriate patients for neurostimulation implants must meet the following criteria: the patient has a diagnosis amenable to this therapy, the patient has failed conservative therapy, significant psychological issues have been ruled out, and a trial has demonstrated pain relief. A trial period of stimulation over a period of 5–7 days should follow the psychiatric evaluation to demonstrate its effectiveness. This part of the protocol is important because of the cost of the equipment and the invasive nature of the procedure. The trial is considered successful if the patient achieves more than a 50% reduction in pain.[16]
History
Electrotherapy of pain by neurostimulation began shortly after Melzack and Wall proposed the gate control theory in 1965.[19] This theory proposed that nerves carrying painful peripheral stimuli and nerves carrying touch and vibratory sensation both terminate in the dorsal horn (the gate) of spinal cord. It was hypothesized that input to the latter could be manipulated to “close the gate” to the former. As an application of the gate control theory, Shealy et al. implanted the first spinal cord stimulator device directly on the dorsal column for the treatment of chronic pain[20] and in 1971, Shimogi and colleagues first reported the analgesic properties of epidural spinal cord stimulation.[21] Since then this technique has undergone numerous technical and clinical developments.[16]
At this time neurostimulation for the treatment of pain is used with nerve stimulation, spinal cord stimulation, deep brain stimulation, and motor cortex stimulation.
Cost effectiveness
The cost effectiveness of spinal cord stimulation in the treatment of chronic back pain was evaluated by Kumar and colleagues in 2002.[22] They examined 104 patients with failed back surgery syndrome. Of the 104 patients, 60 were implanted with a spinal cord stimulator. Both groups were monitored over a period of five years. The stimulation group annual cost was $29,000 versus $38,000 in the other group. 15% returned to work in the stimulation group versus 0% in the other group. The higher costs in the nonstimulator group were in the categories of medications, emergency center visits, x-rays, and ongoing physician visits. See also[23] for another study of cost effectiveness. See[16] for list of such studies on cost effectiveness in various applications of SCS.
Research
SCS is finding its way to be applied to Parkinson’s disease.[24][25] Recently, a case study demonstrated the first successful result of this technique in a patient with Parkinson's disease.[26] More complex and power efficient microprocessor based equipment increasing the battery life could be developed. Closed loop bio-feedback systems which communicate and record neural responses following spinal cord stimulation could be applied and utilized[27] In the future, it might be possible to combine SCS with implanted drug delivery systems to produce synergistic effects minimizing side effects and complications. Strong evidence is still lacking for SCS which may emerge in near future following robust research studies complimenting the rapid technological advances that is taking place in the field of SCS.[15]
See also
References
- ↑ Dimitrijevic, MM; Dimitrijevic, MR; Illis, LS; Nakajima, K; Sharkey, PC; Sherwood, AM (Spring 1986). "Spinal cord stimulation for the control of spasticity in patients with chronic spinal cord injury: I. Clinical observations.". Central nervous system trauma : journal of the American Paralysis Association. 3 (2): 129–44. PMID 3490312.
- ↑ Pinter, MM; Gerstenbrand, F; Dimitrijevic, MR (September 2000). "Epidural electrical stimulation of posterior structures of the human lumbosacral cord: 3. Control Of spasticity.". Spinal Cord. 38 (9): 524–31. doi:10.1038/sj.sc.3101040. PMID 11035472.
- ↑ Dimitrijevic, MR, Kakulas, B, McKay, WB, Vrbova, G. Restorative neurology of spinal cord injury. New York: Oxford University Press. ISBN 978-0-19-974650-7.
- ↑ Harkema, S; Gerasimenko, Y; Hodes, J; Burdick, J; Angeli, C; Chen, Y; Ferreira, C; Willhite, A; Rejc, E; Grossman, RG; Edgerton, VR (Jun 4, 2011). "Effect of epidural stimulation of the lumbosacral spinal cord on voluntary movement, standing, and assisted stepping after motor complete paraplegia: a case study.". Lancet. 377 (9781): 1938–47. doi:10.1016/S0140-6736(11)60547-3. PMC 3154251
 . PMID 21601270.
. PMID 21601270. - ↑ Minassian, K; Hofstoetter, U; Tansey, K; Mayr, W (June 2012). "Neuromodulation of lower limb motor control in restorative neurology.". Clinical neurology and neurosurgery. 114 (5): 489–97. doi:10.1016/j.clineuro.2012.03.013. PMC 3341569. PMID 22464657.
- ↑ "Vienna Program for Movement Recovery". Retrieved 13 November 2012.
- ↑ Kumar, K., Taylor. R.S., Jacques, L., et al. (2008). "The effects of spinal cord stimulation in neuropathic pain are sustained: a 24-month follow-up of the prospective randomized controlled multicenter trial of the effectiveness of spinal cord stimulation" Neurosurgery 63(4), 762–770.
- ↑ North, R.B., Kidd, D.H., and Piantadosi, S. (1995). "Spinal cord stimulation versus reoperation for failed back surgery syndrome: a prospective, randomized study design". Acta Neurochir. Suppl.,64, 106–108.
- ↑ Barolat, G., Oakley, J., Law, J., et al. (2001). "Epidural spinal cord stimulation with a multiple electrode paddle lead is effective in treating low back pain". Neuromodulation, 2, 59–66.
- ↑ Turner, J.A., Loeser, J.D., and Bell, K.G. (1995). "Spinal cord stimulation for chronic low back pain: a systematic literature synthesis" Neurosurgery 37(6), 1088–1095.
- ↑ North, R. and Wetzel, T. (2002). "Spinal cord stimulation for chronic pain of spinal origin" Spine 22, 2584–2591.
- ↑ Amann, W., Berg, P., Gersbach, P., Gamain, J., Raphael, J.H., Ubbink, D.T. (2003). "Spinal cord stimulation in the treatment of nonreconstructable stable critical leg ischaemia: results of the European Peripheral Vascular Disease Outcome Study (SCSEPOS) ". Eur J Vasc Endovasc Surg. 26, 280–286.
- ↑ Taylor, R.S., De Vries, J., Buchser, E., et al. (2009). "Spinal cord stimulation in the treatment of refractory angina: systematic review and meta-analysis of randomised controlled trials". BMC Cardiovasc Disord, 9(13).
- ↑ Matharu MS, Bartsch T, Ward N, Frackowiak RS, Weiner R, Goadsby PJ (2004). "Central neuromodulation in chronic migraine patients with suboccipital stimulators: a PET study". Brain. 127 (Pt 1): 220–30. doi:10.1093/brain/awh022. PMID 14607792.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Kunnumpurath S., Srinivasagopalan, R., Vadivelu, N. (2009). Spinal cord stimulation: Principles of past, present and future practice: A review. Journal of Clinical Monitoring and Computing, 23, 333-339.
- 1 2 3 4 5 6 7 Dilorenzo, D. J.; and Bronzino, J. D. (2008). Neuroengineering. CRC Press. Chapter 7. ISBN 978-0-8493-8174-4
- ↑ Linderoth, B. and Foreman, R. (1999) "Physiology of spinal cord stimulation: review and update". Neuromodulation, 3, 150–164.
- ↑ Oakley, J. and Prager, J. (2002). "Spinal cord stimulation: mechanism of action" Spine 27, 2574–2583.
- ↑ Melzack, R., and Wall, P.D. (1965). Pain mechanisms: a new theory" Science 150:971–979.
- ↑ Shealy, C.N., Mortimer, J.T., and Resnick, J. Electrical inhibition of pain by stimulation of the dorsal columns: Preliminary reports. J. Int. Anesth. Res. Soc, 46:489–491, 1967.
- ↑ Shimoji K, Higashi H, Kano T, Asai S, Morioka T. Electrical management of intractable pain. (1971) Masui (The Japanese journal of anesthesiology), 20: 444–447.
- ↑ Kumar, K., Malik, S., and Demeria, D. (2002). "Treatment of chronic pain with spinal cord stimulation versus alternative therapies: cost-effectiveness analysis" Neurosurgery 51(1), 106–115.
- ↑ Bell, G. and North, R. (1997). "Cost-effectiveness analysis of spinal cord stimulation in treatment of failed back surgery syndrome". J. Pain Symptom Manage., 13 (5), 285–296.
- ↑ Fuentes, R., Petersson, P., Siesser, W. B., Caron, M. G., & Nicolelis, M. A. L. (2009). Spinal Cord Stimulation Restores Locomotion in Animal Models of Parkinson's Disease" Science 323(5921), 1578-1582.
- ↑ Spinal Cord Stimulator Sparks Hope for Parkinson's Disease – Duke University
- ↑ Fénelon G, Goujon C, Gurruchaga JM, Cesaro P, Jarraya B, Palfi S, Lefaucheur JP. (2011). Spinal cord stimulation for chronic pain improved motor function in a patient with Parkinson's disease. Parkinsonism & Related Disorders (In Press)
- ↑ Nam, Y., Brown, E.A., Ross, J.D., et al. (2009) "A retrofitted neural recording system with a novel stimulation IC to monitor early neural responses from a stimulating electrode". J Neurosci Methods. 178(1), 99–102.
Further reading
- Zhou, David and Greenbaum, Elias. (2009). Implantable Neural Prostheses 1: Devices and Applications. Springer. pp. ISBN 978-0-387-77260-8.
- Sakas, Damianos, Simpson, Brian. (2007). Operative Neuromodulation: Volume 2: Neural Networks Surgery. Springer. pp. 333–428. ISBN 978-3-211-33080-7
- North, R.B. (2008). "Neural interface devices: spinal cord stimulation technology". Proceedings of the IEEE. 96, 1108-19.
- Mailis-Gagnon A, Furlan AD, Sandoval JA, Taylor R (2004). Mailis-Gagnon, Angela, ed. "Cochrane Database of Systematic Reviews". Cochrane Database Syst Rev (3): CD003783. doi:10.1002/14651858.CD003783.pub2. PMID 15266501.
|chapter=ignored (help) - North RB, Kidd DH, Farrokhi F, Piantadosi SA (2005). "Spinal cord stimulation versus repeated lumbosacral spine surgery for chronic pain: a randomized, controlled trial". Neurosurgery. 56 (1): 98–106; discussion 106–7. doi:10.1227/01.NEU.0000144311.88383.EF. PMID 15617591.
- Levy, Carol Jay, A PAINED LIFE, a chronic pain journey, Xlibris, Phila, 2003. This book describes chronic pain patient's struggle with and fight against chronic pain. The book includes author's experience with dorsal column stimulator implant.