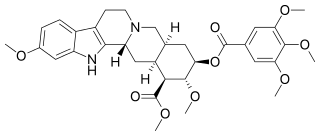
Reserpine
 | |
| Clinical data | |
|---|---|
| AHFS/Drugs.com | Consumer Drug Information |
| MedlinePlus | a601107 |
| License data | |
| Pregnancy category |
|
| Routes of administration | Oral |
| ATC code | C02AA02 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 50% |
| Metabolism | gut/liver |
| Biological half-life |
phase 1 = 4.5h, phase 2 = 271h, average = 33h |
| Excretion | 62% feces / 8% urine |
| Identifiers | |
| |
| CAS Number |
50-55-5 |
| PubChem (CID) | 5770 |
| IUPHAR/BPS | 4823 |
| DrugBank |
DB00206 |
| ChemSpider |
5566 |
| UNII |
8B1QWR724A |
| KEGG |
D00197 |
| ChEBI |
CHEBI:28487 |
| ChEMBL |
CHEMBL772 |
| ECHA InfoCard | 100.000.044 |
| Chemical and physical data | |
| Formula | C33H40N2O9 |
| Molar mass | 608.68 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
| (verify) | |
Reserpine (also known by trade names Raudixin, Serpalan, Serpasil) is an indole alkaloid,[1] antipsychotic, and antihypertensive drug that has been used for the control of high blood pressure and for the relief of psychotic symptoms, although because of the development of better drugs for these purposes and because of its numerous side-effects, it is rarely used today.[2] The antihypertensive actions of reserpine are a result of its ability to deplete catecholamines (among other monoamine neurotransmitters) from peripheral sympathetic nerve endings. These substances are normally involved in controlling heart rate, force of cardiac contraction and peripheral vascular resistance.[3]
Reserpine-mediated depletion of monoamine neurotransmitters in the synapses is often cited as evidence to the theory that depletion of the monoamine neurotransmitters causes subsequent depression in humans (c.f. monoamine hypothesis). However, this claim is not without controversy. The reserpine-induced depression is considered by some researchers to be a myth, while others claim that teas made out of the plant roots containing reserpine have a calming, sedative action that can actually be considered antidepressant.[4] Notably, reserpine was the first compound shown to be an effective antidepressant in a randomized placebo-controlled trial.[5]
Moreover, reserpine has a peripheral action in many parts of the body, resulting in a preponderance of the effects of the cholinergic part of the autonomous nervous system on the GI tract, smooth muscles, blood vessels, etc.
Mechanism of action
Reserpine irreversibly blocks the vesicular monoamine transporter (VMAT).[6] This normally transports free intracellular norepinephrine, serotonin, and dopamine in the presynaptic nerve terminal into presynaptic vesicles for subsequent release into the synaptic cleft ("exocytosis"). Unprotected neurotransmitters are metabolized by MAO (as well as by COMT) in the cytoplasm and consequently never excite the post-synaptic cell.
It may take the body days to weeks to replenish the depleted VMAT, so reserpine's effects are long-lasting.
This depletion of dopamine can lead to drug-induced parkinsonism.[7]
Biosynthetic pathway
Tryptophan is the starting material in the biosynthetic pathway of reserpine, and is converted to tryptamine by tryptophan decarboxylase enzyme. Tryptamine is combined with secologanin in the presence of strictosidine synthetase enzyme and yields strictosidine. Various enzymatic conversion reactions lead to the synthesis of reserpine from strictosidine.[8]
History
Reserpine was isolated in 1952 from the dried root of Rauwolfia serpentina (Indian snakeroot),[9] which had been known as Sarpagandha and had been used for centuries in India for the treatment of insanity, as well as fever and snakebites[2] — Mahatma Gandhi used it as a tranquilizer.[10] It was first used in the United States by Robert Wallace Wilkins in 1950. Its molecular structure was elucidated in 1953 and natural configuration published in 1955.[11] It was introduced in 1954, two years after chlorpromazine.[12] The first total synthesis was accomplished by R. B. Woodward in 1958.[11]
Reserpine almost irreversibly blocks the uptake (and storage) of norepinephrine (i.e. noradrenaline) and dopamine into synaptic vesicles by inhibiting the Vesicular Monoamine Transporters (VMAT).# [13]
Reserpine has been discontinued in the UK for some years due to its numerous interactions and side effects.
Reserpine was also highly influential in promoting the thought of a biogenic amine hypothesis of depression — see Everett & Tolman, 1959.
Uses today
Reserpine is one of the few antihypertensive medications that have been shown in randomized controlled trials to reduce mortality: The Hypertension Detection and Follow-up Program,[14] the Veterans Administration Cooperative Study Group in Anti-hypertensive Agents,[15] and the Systolic Hypertension in the Elderly Program.[16]
Reserpine is rarely used in the management of hypertension today.[17] Reserpine is listed as an option by the JNC 7.[18] Reserpine is a second-line adjunct agent for patients who are uncontrolled on a diuretic when cost is an issue.[19]
It is also used to treat symptoms of dyskinesia in patients suffering from Huntington's disease.[20]
In some countries reserpine is still available as part of combination drugs for the treatment of hypertension, in most cases they contain also a diuretic and/or a vasodilator like hydralazine. These combinations are currently regarded as second choice drugs. The daily dose of reserpine in antihypertensive treatment is as low as 0.1 to 0.25 mg. The use of reserpine as an antipsychotic drug had been nearly completely abandoned, but more recently it made a comeback as adjunctive treatment, in combination with other antipsychotics, so that more refractory patients get dopamine blockade from the other antipsychotic, and dopamine depletion from reserpine. Doses for this kind of adjunctive goal can be kept low, resulting in better tolerability. Originally, doses of 0.5 mg to 40 mg daily were used to treat psychotic diseases. Doses in excess of 3 mg daily often required use of an anticholinergic drug to combat excessive cholinergic activity in many parts of the body as well as parkinsonism. For adjunctive treatment, doses are typically kept at or below 0.25 mg twice a day. Reserpine may be used as a sedative for horses.
Another frequent use of reserpine is in the field of mass spectrometry where it is widely used as a reference standard owing to its availability, ease of ionization under electrospray conditions and stability in solution.
Reserpine is used as a long-acting tranquilizer to subdue excitable or difficult horses and has been used illicitly for the sedation of show horses, for-sale horses, and in other circumstances where a "quieter" horse might be desired.[21]
Reserpine is no longer available in the United Kingdom however it is still available in the United States
Side effects
At doses of less than 0.2 mg/day, reserpine has few side effects, the most common of which is nasal congestion.[22]
There has been much concern about reserpine causing depression leading to suicide. However, this was reported in uncontrolled studies using doses averaging 0.5 mg per day.[23][24]
Reserpine can cause: nasal congestion, nausea, vomiting, weight gain, gastric intolerance, gastric ulceration (due to increased cholinergic activity in gastric tissue and impaired mucosal quality), stomach cramps and diarrhea are noted. The drug causes hypotension and bradycardia and may worsen asthma. Congested nose and erectile dysfunction are other consequences of alpha-blockade.[25] Depression can occur at any dose and may be severe enough to lead to suicide. Other central effects are a high incidence of drowsiness, dizziness, and nightmares. Parkinsonism occurs in a dose dependent manner. General weakness or fatigue is quite often encountered. High dose studies in rodents found reserpine to cause fibroadenoma of the breast and malignant tumors of the seminal vesicles among others. Early suggestions that reserpine causes breast cancer in women (risk approximately doubled) were not confirmed. It may also cause hyperprolactinemia.[25]
Reserpine passes into breast milk and is harmful to breast-fed infants, and should therefore be avoided during breastfeeding if possible.[26]
It also produces a dangerous decline in blood pressure at doses needed for treatment.[27]
References
- ↑ "Indole Alkaloids" Major Types Of Chemical Compounds In Plants & Animals Part II: Phenolic Compounds, Glycosides & Alkaloids. Wayne's Word: An On-Line Textbook of Natural History. 2005.
- 1 2 The Columbia Encyclopedia, Sixth Edition. Copyright © 2001-05 Columbia University Press.
- ↑ Forney, Barbara. Reserpine for Veterinary Use Wedgewood Pharmacy. 2001-2002.
- ↑ Baumeister, A. A.; Hawkins, M. F.; Uzelac, S. M. (2003). "The Myth of Reserpine-Induced Depression: Role in the Historical Development of the Monoamine Hypothesis". Journal of the History of the Neurosciences. 12 (2): 207–220. doi:10.1076/jhin.12.2.207.15535. PMID 12953623.
- ↑ Davies D. L.; Shepherd M. (1955). "Reserpine in the Treatment of Anxious and Depressed Patients". The Lancet. 269: 117–20.
- ↑ Henry, J.; Scherman, D. (1989). "Radioligands of the vesicular monoamine transporter and their use as markers of monoamine storage vesicles". Biochemical Pharmacology. 38 (15): 2395–2404. doi:10.1016/0006-2952(89)90082-8. PMID 2667522.
- ↑ Barcelos, R. C. S.; Benvegnú, D. M.; Boufleur, N.; Pase, C.; Teixeira, A. L. M.; Reckziegel, P. C.; Emanuelli, T.; Da Rocha, J. O. B. T.; Bürger, M. E. (2010). "Short Term Dietary Fish Oil Supplementation Improves Motor Deficiencies Related to Reserpine-Induced Parkinsonism in Rats". Lipids. 46 (2): 143–149. doi:10.1007/s11745-010-3514-0. PMID 21161603.
- ↑ Ramawat et al, 1999.Ramawat KG; Rachnana Sharma; Suri SS. Ramawat, KG.; Merillon, JM., eds. Medicinal Plants in Biotechnology- Secondary metabolites 2nd edition 2007. Oxford and IBH, India. pp. 66–367. ISBN 978-1-57808-428-9.
- ↑ Rauwolfia Dorlands Medical Dictionary. Merck Source. 2002.
- ↑ Pills for Mental Illness?, TIME Magazine, November 8, 1954
- 1 2 Nicolaou, K. C.; E. J. Sorensen (1996). Classics in Total Synthesis. Weinheim, Germany: VCH. p. 55. ISBN 3-527-29284-5.
- ↑ López-Muñoz F, Bhatara VS, Alamo C, Cuenca E (2004). "[Historical approach to reserpine discovery and its introduction in psychiatry]". Actas Esp Psiquiatr. 32: 387–95. PMID 15529229.
- ↑ Schuldiner S.; et al. (1993). "Reserpine binding to a vesicular amine transporter expressed in Chinese hamster ovary fibroblasts". J. Biol. Chem. 268 (1): 29–34. PMID 8416935.
- ↑ , (1979). "Five-year findings of the hypertension detection and follow-up program. I. Reduction in mortality of persons with high blood pressure, including mild hypertension. Hypertension Detection and Follow-up Program Cooperative Group". JAMA. 242 (23): 2562–71. doi:10.1001/jama.242.23.2562. PMID 490882. full text at OVID
- ↑ , (1967). "Effects of treatment on morbidity in hypertension. Results in patients with diastolic blood pressures averaging 115 through 129 mm Hg". JAMA. 202 (11): 1028–34. doi:10.1001/jama.202.11.1028. PMID 4862069.
- ↑ , (1991). "Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). SHEP Cooperative Research Group". JAMA. 265 (24): 3255–64. doi:10.1001/jama.265.24.3255. PMID 2046107.
- ↑ Shamon SD, Perez MI (2009). "Blood pressure lowering efficacy of reserpine for primary hypertension". Cochrane Database of Systematic Reviews. 4: CD007655. doi:10.1002/14651858.CD007655.pub2.
- ↑ Chobanian AV, Bakris GL, Black HR, et al. (2003). "The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report". JAMA. 289 (19): 2560–72. doi:10.1001/jama.289.19.2560. PMID 12748199. summary
- ↑ Moser M (1987). ""Cost containment" in the management of hypertension". Ann. Intern. Med. 107 (1): 107–9. doi:10.7326/0003-4819-107-1-107. PMID 3592424.
- ↑ Shen, Howard (2008). Illustrated Pharmacology Memory Cards: PharMnemonics. Minireview. p. 11. ISBN 1-59541-101-1.
- ↑ Forney B. Reserpine for veterinary use. Available at http://www.wedgewoodpetrx.com/learning-center/professional-monographs/reserpine-for-veterinary-use.html.
- ↑ Curb JD, Schneider K, Taylor JO, Maxwell M, Shulman N (1988). "Antihypertensive drug side effects in the Hypertension Detection and Follow-up Program". Hypertension. 11 (3 Pt 2): II51–5. doi:10.1161/01.hyp.11.3_pt_2.ii51. PMID 3350594.
- ↑ QUETSCH RM, ACHOR RW, LITIN EM, FAUCETT RL (1959). "Depressive reactions in hypertensive patients; a comparison of those treated with Rauwolfia and those receiving no specific antihypertensive treatment". Circulation. 19 (3): 366–75. doi:10.1161/01.cir.19.3.366. PMID 13629798.
- ↑ Lemieux G, Davignon A, Genest J (1956). "Depressive states during Rauwolfia therapy for arterial hypertension; a report of 30 cases". Canadian Medical Association Journal. 74 (7): 522–6. PMC 1823144
 . PMID 13304797.
. PMID 13304797. - 1 2 AJ Giannini,HR Black. Psychiatric, Psychogenic, and Somatopsychic Disorders Handbook. Garden City,NY. Medical Examination Publishing, 1978. Pg. 233. ISBN 0-87488-596-5.
- ↑ kidsgrowth.org --> Drugs and Other Substances in Breast Milk Retrieved on June 19, 2009
- ↑ Pinel, John P.J. (2011). Biopsychology (8th ed.). Boston: Allyn & Bacon. p. 469. ISBN 978-0205832569.
External links
- NLM Hazardous Substances Databank – Reserpine
- PubChem Substance Summary: Reserpine National Center for Biotechnology Information.
- The Stork Synthesis of (−)-Reserpine