Proton-pump inhibitor
| Proton-pump inhibitor | |
|---|---|
| Drug class | |
|
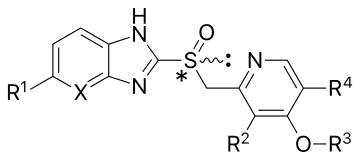
General structure of a proton-pump inhibitor | |
| Class identifiers | |
| Use | Reduction of gastric acid production |
| ATC code | A02BC |
| Mechanism of action | Enzyme inhibitor |
| Biological target | H+/K+ ATPase |
| Clinical data | |
| Drugs.com | Drug Classes |
| WebMD | MedicineNet |
| External links | |
| MeSH | D054328 |
| In Wikidata | |
Proton pump inhibitors (PPIs) are a group of drugs whose main action is a pronounced and long-lasting reduction of gastric acid production. Within the class of medications, there is no clear evidence that one agent works better than another.[1][2]
They are the most potent inhibitors of acid secretion available.[3] This group of drugs followed and largely superseded another group of medications with similar effects, but a different mode of action, called H2-receptor antagonists.
PPIs are among the most widely sold drugs in the world, and the first one, omeprazole, is on the WHO Model List of Essential Medicines.[4] The cost between different agents varies significantly.[1]
Medical uses
These drugs are used in the treatment of many conditions, such as:
- Dyspepsia[5][6]
- Peptic ulcer disease including after endoscopic treatment for bleeding[7]
- As part of Helicobacter pylori eradication therapy[8]
- Gastroesophageal reflux disease (GERD or GORD) including symptomatic endoscopy-negative reflux disease[9] and
- associated laryngopharyngeal reflux causing laryngitis[10] and chronic cough[11]
- Barrett's esophagus[12]
- Eosinophilic esophagitis[13]
- Stress gastritis and ulcer prevention in critical care[14]
- Gastrinomas and other conditions that cause hypersecretion of acid including Zollinger–Ellison syndrome (often 2–3x the regular dose is required)[15]
Specialty professional organizations recommend that people take the lowest effective PPI dose to achieve the desired therapeutic result when used to treat gastroesophageal reflux disease long-term.[16][17] In the United States, the Food and Drug Administration has advised that no more than three 14-day treatment courses should be used in one year.[18]
Despite their extensive use, the quality of the evidence supporting their use in some of these conditions is variable. The effectiveness of PPIs has not been demonstrated for every case. For example, although they reduce the incidence of esophageal adenocarcinoma in Barrett's oesophagus,[12] they do not change the length affected.[19]
Adverse effects
In general, proton pump inhibitors are well tolerated, and the incidence of short-term adverse effects is relatively low. Long-term use of PPIs has been less studied than short-term use, and the lack of data makes it difficult to make definitive statements.[20] The range and occurrence of adverse effects are similar for all of the PPIs, though they have been reported more frequently with omeprazole. This may be due to its longer availability and, hence, clinical experience.
Common adverse effects include headache, nausea, diarrhea, abdominal pain, fatigue, and dizziness.[21] Infrequent adverse effects include rash, itch, flatulence, constipation, anxiety, and depression. Also infrequently, PPI use may be associated with occurrence of myopathies, including the serious reaction rhabdomyolysis.[22]
Nutritional
Gastric acid is important for breakdown of food and release of micronutrients, and some studies have shown possibilities for interference with absorption of iron, calcium, magnesium, and vitamin B12.[23] With regard to iron and vitamin B12 the data are weak and several confounding factors have been identified.[20][23]
Low levels of magnesium can be found in people on PPI therapy and these can be reversed when they are switched to H2-receptor antagonist drugs.[20][24]
High dose and/or long-term use of PPIs carries a possible increased risk of bone fractures which was not found with short-term, low dose use; the FDA included a warning regarding this on PPI drug labels in 2010.[18]
Gastrointestinal
Some studies have shown a correlation between use of PPIs and Clostridium difficile infections. While the data are contradictory and controversial, the FDA had sufficient concern to include a warning about this adverse effect on the label of PPI drugs.[20] Concerns have also been raised about spontaneous bacterial peritonitis in older people taking PPIs and in people with irritable bowel syndrome taking PPIs; both types of infections arise in these populations due to underlying conditions and it is not clear if this is a class effect of PPIs.[20] PPIs may predispose an individual to developing small intestinal bacterial overgrowth or small intestinal fungal overgrowth.[25][26]
Long-term use of PPIs is associated with the development of benign polyps from fundic glands (which is distinct from fundic gland polyposis); these polyps do not cause cancer and resolve when PPIs are discontinued. There is no association between PPI use and cancer[20] or pre-cancer.[27] There is concern that use of PPIs may mask gastric cancers or other serious gastric problems and physicians should be aware of this effect.[20]
PPI use has also been associated with the development of microscopic colitis.[28]
There is also evidence that PPI use alters the composition of the bacterial populations inhabiting the gut.[29] Although the mechanisms by which PPIs cause these changes are yet to be determined they may have a role in the increased risk of bacterial infections with PPI use.
Cardiovascular
Associations of PPI use and cardiovascular events have also been widely studied but clear conclusions have not been made as these relative risks are confounded by other factors.[30][31] PPIs are commonly used in cardiovascular patients for gastric protection when aspirin is given for its antiplatelet actions.[30][32] An interaction between PPIs and the metabolism of the platelet inhibitor clopidogrel is known and this drug is also often used in patients with cardiac disease.[33][34]
One suggested mechanism for cardiovascular effects is because PPIs bind and inhibit dimethylargininase, the enzyme that degrades asymmetric dimethylarginine (ADMA), resulting in higher ADMA levels and a decrease in bioavailable nitric oxide.[35]
Other
Associations have been shown between PPI use and an increased risk of pneumonia, particularly in the 30 days after starting therapy, where it was found to be 50% higher in community use.[36][37] A primary research study using pharmacoepidemiological claims data analysis has reported an association between PPI use and the risk of developing dementia in people over the age of 75 (1.4x hazard ratio)[38] but this has not been examined in prospective studies. Inappropriate prescribing of PPIs in the elderly, including those with dementia, has been reported.[39] Weak associations with chronic kidney disease have been found (1.5x hazard ratio), but these low hazard ratios make it doubtful whether such associations are causal relationships.[40]
Mechanism of action

Proton pump inhibitors act by irreversibly blocking the hydrogen/potassium adenosine triphosphatase enzyme system (the H+/K+ ATPase, or, more commonly, the gastric proton pump) of the gastric parietal cells.[41] The proton pump is the terminal stage in gastric acid secretion, being directly responsible for secreting H+ ions into the gastric lumen, making it an ideal target for inhibiting acid secretion.
Targeting the terminal step in acid production, as well as the irreversible nature of the inhibition, results in a class of drugs that are significantly more effective than H2 antagonists and reduce gastric acid secretion by up to 99%.
Decreasing the acid in the stomach can aid the healing of duodenal ulcers and reduce the pain from indigestion and heartburn. Stomach acids are needed however to digest proteins, vitamin B12, calcium, and other nutrients. Too little stomach acid causes the condition hypochlorhydria.
The PPIs are given in an inactive form, which is neutrally charged (lipophilic) and readily crosses cell membranes into intracellular compartments (like the parietal cell canaliculus) with acidic environments. In an acid environment, the inactive drug is protonated and rearranges into its active form. As described above, the active form will covalently and irreversibly bind to the gastric proton pump, deactivating it.
Pharmacokinetics
The rate of omeprazole absorption is decreased by concomitant food intake. In addition, the absorption of lansoprazole and esomeprazole is decreased and delayed by food. It has been reported, however, that these pharmacokinetic effects have no significant impact on efficacy.[42][43]
PPIs have a half-life in human blood plasma of only 60–90 minutes, but because they covalently bind to the pump, the half-life of their inhibition of gastric acid secretion lasts an estimated 24 hours. Dissociation of the inhibitory complex is probably due to the effect of the endogenous antioxidant glutathione which leads to the release of omeprazole sulfide and reactivation of the enzyme.[44][45]
Examples
Medically used proton pump inhibitors:
- Omeprazole (OTC in the USA)
- Lansoprazole
- Dexlansoprazole
- Esomeprazole
- Pantoprazole
- Rabeprazole (also avaliable in combination with domperidone)).
- Ilaprazole (not FDA approved as of October 2013)
History
PPIs were developed in the 1980s with omeprazole being launched in 1988. Most of these drugs are benzimidazole derivatives, related to omeprazole, but imidazopyridine derivatives such as tenatoprazole have also been developed.[3] Potassium-competitive inhibitors such as revaprazan reversibly block the potassium-binding site of the proton pump, acting more quickly, but are not available in most countries.[46]
Cost
In British Columbia, Canada the cost of the PPIs varies significantly from 0.20 CAD to 2.38 CAD per dose while all agents in the class appear more or less equally effective.[1][2]
References
- 1 2 3 "[99] Comparative effectiveness of proton pump inhibitors | Therapeutics Initiative". 28 June 2016. Retrieved 14 July 2016.
- 1 2 Dean, Laura (1 October 2010). "Comparing Proton Pump Inhibitors". PubMed Health. Retrieved 16 July 2016.
- 1 2 Sachs, G.; Shin, J. M.; Howden, C. W. (2006). "Review article: The clinical pharmacology of proton pump inhibitors". Alimentary Pharmacology and Therapeutics. 23: 2–8. doi:10.1111/j.1365-2036.2006.02943.x. PMID 16700898.
- ↑ "WHO Model List of EssentialMedicines" (PDF). World Health Organization. October 2013. Retrieved 22 April 2014.
- ↑ Zajac, P; Holbrook, A; Super, ME; Vogt, M (March–April 2013). "An overview: Current clinical guidelines for the evaluation, diagnosis, treatment, and management of dyspepsia". Osteopathic Family Physician. 5 (2): 79–85. doi:10.1016/j.osfp.2012.10.005.
- ↑ Wang WH, Huang JQ, Zheng GF, Xia HH, Wong WM, Liu XG, et al. (2007). "Effects of proton-pump inhibitors on functional dyspepsia: a meta-analysis of randomized placebo-controlled trials". Clinical Gastroenterology and Hepatology. 5 (2): 178–85; quiz 140. doi:10.1016/j.cgh.2006.09.012. PMID 17174612.
- ↑ Sachar H, Vaidya K, Laine L (2014). "Intermittent vs continuous proton pump inhibitor therapy for high-risk bleeding ulcers: a systematic review and meta-analysis". JAMA Internal Medicine. 174 (11): 1755–62. doi:10.1001/jamainternmed.2014.4056. PMC 4415726
 . PMID 25201154.
. PMID 25201154. - ↑ Yuan Y, Ford AC, Khan KJ, Gisbert JP, Forman D, Leontiadis GI, et al. (2013). "Optimum duration of regimens for Helicobacter pylori eradication". Cochrane Database of Systematic Reviews. 12: CD008337. doi:10.1002/14651858.CD008337.pub2. PMID 24338763.
- ↑ Sigterman KE, van Pinxteren B, Bonis PA, Lau J, Numans ME (2013). "Short-term treatment with proton pump inhibitors, H2-receptor antagonists and prokinetics for gastro-oesophageal reflux disease-like symptoms and endoscopy negative reflux disease". Cochrane Database of Systematic Reviews. 5: CD002095. doi:10.1002/14651858.CD002095.pub5. PMID 23728637.
- ↑ Qadeer MA, Phillips CO, Lopez AR, Steward DL, Noordzij JP, Wo JM, et al. (2006). "Proton pump inhibitor therapy for suspected GERD-related chronic laryngitis: a meta-analysis of randomized controlled trials". The American Journal of Gastroenterology. 101 (11): 2646–54. doi:10.1111/j.1572-0241.2006.00844.x. PMID 17037995.
- ↑ Chang AB, Lasserson TJ, Kiljander TO, Connor FL, Gaffney JT, Garske LA (2006). "Systematic review and meta-analysis of randomised controlled trials of gastro-oesophageal reflux interventions for chronic cough associated with gastro-oesophageal reflux". The BMJ. 332 (7532): 11–7. doi:10.1136/bmj.38677.559005.55. PMC 1325125. PMID 16330475.
- 1 2 Singh S, Garg SK, Singh PP, Iyer PG, El-Serag HB (2014). "Acid-suppressive medications and risk of oesophageal adenocarcinoma in patients with Barrett's oesophagus: a systematic review and meta-analysis". Gut. 63 (8): 1229–37. doi:10.1136/gutjnl-2013-305997. PMC 4199831. PMID 24221456.
- ↑ Lucendo AJ, Arias Á, Molina-Infante J (2015). "Efficacy of Proton Pump Inhibitor Drugs for Inducing Clinical and Histological Remission in Patients with Symptomatic Esophageal Eosinophilia: A Systematic Review and Meta-Analysis". Clinical Gastroenterology and Hepatology. 14 (1): 13–22.e1. doi:10.1016/j.cgh.2015.07.041. PMID 26247167.
- ↑ Alhazzani W, Alenezi F, Jaeschke RZ, Moayyedi P, Cook DJ (2013). "Proton pump inhibitors versus histamine 2 receptor antagonists for stress ulcer prophylaxis in critically ill patients: a systematic review and meta-analysis". Critical Care Medicine. 41 (3): 693–705. doi:10.1097/CCM.0b013e3182758734. PMID 23318494.
- ↑ Epelboym I, Mazeh H (2014). "Zollinger-Ellison syndrome: classical considerations and current controversies". Oncologist. 19 (1): 44–50. doi:10.1634/theoncologist.2013-0369. PMC 3903066. PMID 24319020.
- ↑ "Five Things Physicians and Patients Should Question". American Gastroenterological Association.
- ↑ Kahrilas, Peter J.; Shaheen, Nicholas J.; Vaezi, Michael F.; Hiltz, SW; Black, E; Modlin, IM; Johnson, SP; Allen, J; Brill, JV (2008). "American Gastroenterological Association Medical Position Statement on the Management of Gastroesophageal Reflux Disease". Gastroenterology. 135 (4): 1383–1391, 1391.e1–5. doi:10.1053/j.gastro.2008.08.045. PMID 18789939.
- 1 2 "FDA Drug Safety Communication: Possible increased risk of fractures of the hip, wrist, and spine with the use of proton pump inhibitors". U S Food and Drug Administration. 23 March 2011. Retrieved 23 August 2015.
- ↑ Cooper, B. T.; Chapman, W.; Neumann, C. S.; Gearty, J. C. (2006). "Continuous treatment of Barrett's oesophagus patients with proton pump inhibitors up to 13 years: Observations on regression and cancer incidence". Alimentary Pharmacology and Therapeutics. 23 (6): 727–33. doi:10.1111/j.1365-2036.2006.02825.x. PMID 16556174.
- 1 2 3 4 5 6 7 Corleto VD; et al. (February 2014). "Proton pump inhibitor therapy and potential long-term harm". Current Opinion in Endocrinology, Diabetes and Obesity. 21 (1): 3–8. doi:10.1097/MED.0000000000000031. PMID 24310148.
- ↑ Rossi S, editor. Australian Medicines Handbook 2006. Adelaide: Australian Medicines Handbook; 2006. ISBN 0-9757919-2-3
- ↑ Clark, DW; Strandell J (June 2006). "Myopathy including polymyositis: a likely class adverse effect of proton pump inhibitors?". European Journal of Clinical Pharmacology. 62 (6): 473–479. doi:10.1007/s00228-006-0131-1. PMID 16758264.
- 1 2 Ito T, Jensen RT (2010). "Association of long-term proton pump inhibitor therapy with bone fractures and effects on absorption of calcium, vitamin B12, iron, and magnesium". Current Gastroenterology Reports. 12 (6): 448–57. doi:10.1007/s11894-010-0141-0. PMC 2974811. PMID 20882439.
- ↑ Park CH, Kim EH, Roh YH, Kim HY, Lee SK (2014). "The association between the use of proton pump inhibitors and the risk of hypomagnesemia: a systematic review and meta-analysis". PLoS ONE. 9 (11): e112558. doi:10.1371/journal.pone.0112558. PMC 4230950. PMID 25394217.
- ↑ Fujimori S (2015). "What are the effects of proton pump inhibitors on the small intestine?". World J. Gastroenterol. 21 (22): 6817–9. doi:10.3748/wjg.v21.i22.6817. PMC 4462721. PMID 26078557.
Generally, proton-pump inhibitors (PPIs) have great benefit for patients with acid related disease with less frequently occurring side effects. According to a recent report, PPIs provoke dysbiosis of the small intestinal bacterial flora, exacerbating nonsteroidal anti-inflammatory drug-induced small intestinal injury. Several meta-analyses and systematic reviews have reported that patients treated with PPIs, as well as post-gastrectomy patients, have a higher frequency of small intestinal bacterial overgrowth (SIBO) compared to patients who lack the aforementioned conditions. Furthermore, there is insufficient evidence that these conditions induce Clostridium difficile infection. At this time, PPI-induced dysbiosis is considered a type of SIBO.
- ↑ Erdogan A, Rao SS (April 2015). "Small intestinal fungal overgrowth". Curr Gastroenterol Rep. 17 (4): 16. doi:10.1007/s11894-015-0436-2. PMID 25786900.
Small intestinal fungal overgrowth (SIFO) is characterized by the presence of excessive number of fungal organisms in the small intestine associated with gastrointestinal (GI) symptoms. Candidiasis is known to cause GI symptoms particularly in immunocompromised patients or those receiving steroids or antibiotics. However, only recently, there is emerging literature that an overgrowth of fungus in the small intestine of non-immunocompromised subjects may cause unexplained GI symptoms. Two recent studies showed that 26 % (24/94) and 25.3 % (38/150) of a series of patients with unexplained GI symptoms had SIFO. The most common symptoms observed in these patients were belching, bloating, indigestion, nausea, diarrhea, and gas. The underlying mechanism(s) that predisposes to SIFO is unclear but small intestinal dysmotility and use of proton pump inhibitors has been implicated. However, further studies are needed; both to confirm these observations and to examine the clinical relevance of fungal overgrowth, both in healthy subjects and in patients with otherwise unexplained GI symptoms.
- ↑ Song, H; Zhu, J; Lu, D (2 December 2014). "Long-term proton pump inhibitor (PPI) use and the development of gastric pre-malignant lesions.". The Cochrane database of systematic reviews. 12: CD010623. doi:10.1002/14651858.CD010623.pub2. PMID 25464111.
- ↑ Münch A, Aust D, Bohr J, Bonderup O, Fernández Bañares F, Hjortswang H, et al. (2012). "Microscopic colitis: Current status, present and future challenges: statements of the European Microscopic Colitis Group". Journal of Crohn's and Colitis. 6 (9): 932–45. doi:10.1016/j.crohns.2012.05.014. PMID 22704658.
- ↑ Jackson, Matthew A.; Goodrich, Julia K.; Maxan, Maria-Emanuela; Freedberg, Daniel E.; Abrams, Julian A.; Poole, Angela C.; Sutter, Jessica L.; Welter, Daphne; Ley, Ruth E. (2015-12-30). "Proton pump inhibitors alter the composition of the gut microbiota". Gut. 65 (5): gutjnl–2015–310861. doi:10.1136/gutjnl-2015-310861. ISSN 1468-3288. PMC 4853574. PMID 26719299.
- 1 2 Agewall S, Cattaneo M, Collet JP, Andreotti F, Lip GY, Verheugt FW, et al. (2013). "Expert position paper on the use of proton pump inhibitors in patients with cardiovascular disease and antithrombotic therapy". European Heart Journal. 34 (23): 1708–13, 1713a–1713b. doi:10.1093/eurheartj/eht042. PMID 23425521.
- ↑ Melloni C, Washam JB, Jones WS, Halim SA, Hasselblad V, Mayer SB, et al. (2015). "Conflicting results between randomized trials and observational studies on the impact of proton pump inhibitors on cardiovascular events when coadministered with dual antiplatelet therapy: systematic review". Circulation: Cardiovascular Quality and Outcomes. 8 (1): 47–55. doi:10.1161/CIRCOUTCOMES.114.001177. PMID 25587094.
- ↑ Kwok CS, Nijjar RS, Loke YK (2011). "Effects of proton pump inhibitors on adverse gastrointestinal events in patients receiving clopidogrel: systematic review and meta-analysis". Drug Safety. 34 (1): 47–57. doi:10.2165/11584750-000000000-00000. PMID 21047145.
- ↑ Focks JJ, Brouwer MA, van Oijen MG, Lanas A, Bhatt DL, Verheugt FW (2013). "Concomitant use of clopidogrel and proton pump inhibitors: impact on platelet function and clinical outcome- a systematic review". Heart. 99 (8): 520–7. doi:10.1136/heartjnl-2012-302371. PMID 22851683.
- ↑ Cardoso RN, Benjo AM, DiNicolantonio JJ, Garcia DC, Macedo FY, El-Hayek G, et al. (2015). "Incidence of cardiovascular events and gastrointestinal bleeding in patients receiving clopidogrel with and without proton pump inhibitors: an updated meta-analysis". Open Heart. 2 (1): e000248. doi:10.1136/openhrt-2015-000248. PMC 4488889. PMID 26196021.
- ↑ Schepers E, Speer T, Bode-Böger SM, Fliser D, Kielstein JT (2014). "Dimethylarginines ADMA and SDMA: the real water-soluble small toxins?". Seminars in Nephrology. 34 (2): 97–105. doi:10.1016/j.semnephrol.2014.02.003. PMID 24780466. Retrieved 2015-06-11.
It also seems to be the pathophysiological link between the use of proton pump inhibitors and increased cardiovascular event rate because these drugs bind and inhibit DDAH, the enzyme that degrades ADMA, which results in higher ADMA levels and a decrease in bioavailable NO.
- ↑ Lambert AA, Lam JO, Paik JJ, Ugarte-Gil C, Drummond MB, Crowell TA (2015). "Risk of community-acquired pneumonia with outpatient proton-pump inhibitor therapy: a systematic review and meta-analysis". PLoS ONE. 10 (6): e0128004. doi:10.1371/journal.pone.0128004. PMC 4456166. PMID 26042842.
- ↑ Eom, CS; Jeon, CY; Lim, JW; Cho, EG; Park, SM; Lee, KS (22 February 2011). "Use of acid-suppressive drugs and risk of pneumonia: a systematic review and meta-analysis.". CMAJ : Canadian Medical Association. 183 (3): 310–9. doi:10.1503/cmaj.092129. PMC 3042441. PMID 21173070.
- ↑ Gomm W, von Holt K, Thomé F, Broich K, Maier W, Fink A, Doblhammer G, Haenisch B (2016). "Association of Proton Pump Inhibitors With Risk of Dementia: A Pharmacoepidemiological Claims Data Analysis". JAMA Neurology. 73 (4): 410–6. doi:10.1001/jamaneurol.2015.4791. PMID 26882076.
- ↑ Hamzat H, Sun H, Ford JC, Macleod J, Soiza RL, Mangoni AA (2012). "Inappropriate prescribing of proton pump inhibitors in older patients: effects of an educational strategy". Drugs & Aging. 29 (8): 681–90. doi:10.2165/11632700-000000000-00000. PMID 22775478.
- ↑ Kia L, Kahrilas PJ (2016). "Therapy: Risks associated with chronic PPI use - signal or noise?". Nature Reviews. Gastroenterology & Hepatology. 13: 253–4. doi:10.1038/nrgastro.2016.44. PMID 27006255.
- ↑ Sakai, Hideki; Fujii, Takuto; Takeguchi, Noriaki (2016). "Chapter 13. Proton-Potassium (H+/K+) ATPases: Properties and Roles in Health and Diseases". In Astrid, Sigel; Helmut, Sigel; Roland K.O., Sigel. The Alkali Metal Ions: Their Role in Life. Metal Ions in Life Sciences. 16. Springer. pp. 459–483. doi:10.1007/978-4-319-21756-7_13.
- ↑ AstraZeneca Pty Ltd. Nexium (Australian approved prescribing information). North Ryde: AstraZeneca; 2005.
- ↑ Wyeth Australia Pty Ltd. Zoton (Australian approved prescribing information). Baulkham Hills: Wyeth; 2004.
- ↑ Shin, Jai Moo; Munson, Keith; Vagin, Olga; Sachs, George (2008). "The gastric HK-ATPase: Structure, function, and inhibition". Pflügers Archiv – European Journal of Physiology. 457 (3): 609–22. doi:10.1007/s00424-008-0495-4. PMC 3079481. PMID 18536934.
- ↑ Carlsson, E; Lindberg, P. (2002). "Two of a kind". Chemistry in Britain. 38 (5): 42–5.
- ↑ Kim HK, Park SH, Cheung DY, Cho YS, Kim JI, Kim SS, et al. (2010). "Clinical trial: inhibitory effect of revaprazan on gastric acid secretion in healthy male subjects". Journal of Gastroenterology and Hepatology. 25 (10): 1618–25. doi:10.1111/j.1440-1746.2010.06408.x. PMID 20880169.
External links
| Wikimedia Commons has media related to Proton pump inhibitors. |