Pneumococcal conjugate vaccine
| Vaccine description | |
|---|---|
| Target disease | Streptococcus pneumoniae |
| Type | Conjugate vaccine |
| Clinical data | |
| AHFS/Drugs.com | Micromedex Detailed Consumer Information |
| MedlinePlus | a607021 |
| ATC code | J07AL02 (WHO) |
| Legal status | |
| Legal status |
|
| Identifiers | |
| ChemSpider | none |
| | |
Pneumococcal conjugate vaccine (PCV) is a pneumococcal vaccine and a conjugate vaccine used to protect infants, young children, and adults against disease caused by the bacterium Streptococcus pneumoniae (the pneumococcus). There are currently three types of PCV available on the global market, which go by the brand names: Prevnar (called Prevenar in some countries), Synflorix and Prevnar 13.
- Prevnar (PCV7) is a heptavalent vaccine, meaning that it contains the cell capsule sugars of seven serotypes of the bacteria S. pneumoniae (4, 6B, 9V, 14, 18C, 19F and 23F), conjugated with diphtheria proteins. It was manufactured by Wyeth (which has since been acquired by Pfizer).[1] In the United States, vaccination with Prevnar is recommended for all children younger than 2 years, and for unvaccinated children between 24 and 59 months old who are at high risk for pneumococcal infections.[2]
- Synflorix (PCV10) is produced by GlaxoSmithKline. It is a decavalent vaccine, meaning that it contains ten serotypes of pneumococcus (1, 4, 5, 6B, 7F, 9V, 14, 18C, 19F and 23F) which are conjugated to a carrier protein. Synflorix received a positive opinion from the European Medicines Agency for use in the European Union in January 2009[3] and GSK received European Commission authorization to market Synflorix in March 2009.[4]
- Prevnar 13 (PCV13) is produced by Pfizer. It is a tridecavalent vaccine, meaning that it contains thirteen serotypes of pneumococcus (1, 3, 4, 5, 6A, 6B, 7F, 9V, 14, 18C, 19A, 19F and 23F) which are conjugated to diphtheria carrier protein. Prevnar 13 was approved by the U.S. Food and Drug Administration on February 24, 2010.[5] After waiting for the outcome of a trial underway in the Netherlands, the Centers for Disease Control and Prevention (CDC) recommended the vaccine for adults over age 65 in August 2014.[6]
Production technique
Prevnar

The original Prevnar was produced from the seven most prevalent strains of S. pneumoniae bacteria in the US. The bacterial capsule sugars, a characteristic of these pathogens, are linked to CRM197, a nontoxic recombinant variant of diphtheria toxin (Corynebacterium diphtheriae).
The vaccine's polysaccharide sugars are grown separately in soy peptone broths. Through reductive amination, the sugars are directly conjugated to the protein carrier CRM197 to form the glycoconjugate. CRM197 is grown in C. diphtheriae strain C7 in a medium of casamino acids and yeast extracts.[7]
The original seven-valent formulation contains serotypes 4, 6B, 9V, 14, 18C, 19F, and 23F, and results in a 98% probability of protection against these strains, which caused 80% of the pneumococcal disease in infants in the US. In 2010, Pfizer introduced Prevnar 13, which contains six additional strains (i.e., 1, 3, 5, 6A, 19A and 7F), which protect against the majority of the remaining pneumococcal infections.[8]
Synflorix
Synflorix contains antigen from ten pneumococcal serotypes: the seven that are contained in Prevnar, plus serotypes 1, 5, and 7F.
Schedule of vaccination
As with all immunizations, whether it is available or required, and under what circumstances, varies according to the decisions made by local public health agencies.
Children under the age of two years fail to mount an adequate response to the 23-valent adult vaccine, and so the 7-valent Pneumococcal Conjugated Vaccine (PCV) (e.g. Prevnar) is used. Whilst this covers only seven strains out of more than ninety strains, these seven strains cause 80% to 90% of cases of severe pneumococcal disease, and it is considered to be nearly 100% effective against these strains.[9]
United Kingdom
The UK childhood vaccination schedule consists of a primary course of two doses at 2 and 4 months of age with a final third dose aged 13 months.[10]
Children at special risk (e.g., sickle cell disease and asplenia) require as full protection as can be achieved using the 7-valent conjugated vaccine, with the more extensive 23-valent vaccine given after the second year of life:
| Age | 2–6 months | 7–11 months | 12–23 months |
| Conjugated vaccine | 3 × monthly dose | 2 × monthly dose | 2 doses, 2 months apart |
| Further dose in second year of life | |||
| 23-valent vaccine | Then after 2nd birthday single dose of 23-valent | ||
United States
In 2001, the Centers for Disease Control (CDC), upon advice from its Advisory Committee on Immunization Practices, recommended the vaccine be administered to every infant and young child in the US. The resulting demand outstripped production, creating shortages not resolved until 2004. All children, according to current US vaccination schedules, should receive four doses, at two months, four months, six months, and again between one year and fifteen months of age.
Efficacy
Prevnar-7 is designed to stop seven of about ninety pneumococcal serotypes which have the potential to cause invasive pneumococcal disease (IPD). In 2010, a 13-valent vaccine was introduced. Each year, IPD kills approximately one million children worldwide. Since approval, Prevnar's efficacy in preventing IPD has been documented by a number of epidemiologic studies.[12][13][14] There is evidence that other people in the same household as a vaccinee also become relatively protected.[15] In fact, there is evidence that routine childhood vaccination reduces the burden of pneumococcal disease in adults and especially high-risk adults, such as those living with HIV/AIDS.[16]
The vaccine is, however, primarily developed for the U.S. and European epidemiological situation, and therefore it has only a limited coverage of serotypes causing serious pneumococcal infections in most developing countries.[17]
Evidence supporting addition to routine vaccination schedules
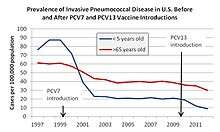
After introduction of the pneumococcal conjugate vaccine in 2000, several studies described a decrease in invasive pneumococcal disease in the United States. One year after its introduction, a group of investigators found a 69% drop in the rate of invasive disease in those of less than two years of age.[12] By 2004, all-cause pneumonia admission rates had declined by 39% (95% CI 22–52) and rates of hospitalizations for pneumococcal meningitis decreased by 66% (95% CI 56.3-73.5) in children younger than 2.[18][19]
Interestingly, rates of invasive pneumococcal disease among adults have also declined since the introduction of the vaccine.[12][19]
Vaccination in low-income countries
Pneumococcal disease is the leading vaccine-preventable killer of young children worldwide, according to the World Health Organization (WHO). It killed more than 500,000 children younger than five years of age in 2008 alone.[20] Approximately ninety percent of these deaths occur in the developing world.[20] Historically 15–20 years pass before a new vaccine reaches one quarter of the population of the developing world.[21]
Pneumococcal vaccines Accelerated Development and Introduction Plan (PneumoADIP) was a GAVI Alliance (GAVI) funded project to accelerate the introduction of pneumococcal vaccinations into low-income countries through partnerships between countries, donors, academia, international organizations and industry. GAVI continues this work and as of March 2013, 25 GAVI-eligible and supported countries have introduced the pneumococcal conjugate vaccine. Further, 15 additional GAVI countries have plans to introduce the vaccine into their national immunization program and 23 additional countries have approved GAVI support to introduce the vaccine.[22]
Sales
Prevnar was among Wyeth's top revenue producers, with sales in 2005 of $1.5 billion, up 43 percent from 2004.[23]
See also
References
- ↑ "Pneumococcal 7-valent Conjugate Vaccine (Diphtheria CRM197 Protein)". Wyeth. 2006.
- ↑ "American Academy of Pediatrics. Committee on Infectious Diseases. Policy statement: recommendations for the prevention of pneumococcal infections, including the use of pneumococcal conjugate vaccine (Prevnar), pneumococcal polysaccharide vaccine, and antibiotic prophylaxis". Pediatrics. 106 (2 Pt 1): 362–6. 2000. doi:10.1542/peds.106.2.362. PMID 10920169.
- ↑ EMEA Document
- ↑ GSK Release
- ↑ http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201758.htm[]
- ↑ "Advisory Committee on Immunization Practices Votes to Recommend Pfizer's Prevnar 13® Vaccine in Adults Aged 65 Years and Older - MarketWatch".
- ↑ http://www.rxlist.com/cgi/generic/prevnar.htm
- ↑ Centers for Disease Control and Prevention (CDC) (March 2010). "Licensure of a 13-valent pneumococcal conjugate vaccine (PCV13) and recommendations for use among children — Advisory Committee on Immunization Practices (ACIP), 2010". MMWR Morb. Mortal. Wkly. Rep. 59 (9): 258–61. PMID 20224542.
- ↑ Childhood Pneumococcal Disease - information on the disease and the Prevnar vaccine, from the Victoria State (Australia) government. Includes possible side effects.
- 1 2 "Chapter 25: Pneumococcal" (PDF). Immunisation against infectious disease - 'The Green Book' (PDF). Department of Health (UK). 2006.
- ↑ "CDC - ABCs: Surveillance Reports main page - Active Bacterial Core surveillance".
- 1 2 3 Whitney CG, Farley MM, Hadler J, et al. (May 2003). "Decline in invasive pneumococcal disease after the introduction of protein-polysaccharide conjugate vaccine". The New England Journal of Medicine. 348 (18): 1737–46. doi:10.1056/NEJMoa022823. PMID 12724479.
- ↑ Poehling KA, Talbot TR, Griffin MR, et al. (April 2006). "Invasive pneumococcal disease among infants before and after introduction of pneumococcal conjugate vaccine". JAMA: the Journal of the American Medical Association. 295 (14): 1668–74. doi:10.1001/jama.295.14.1668. PMID 16609088.
- ↑ Whitney CG, Pilishvili T, Farley MM, et al. (October 2006). "Effectiveness of seven-valent pneumococcal conjugate vaccine against invasive pneumococcal disease: a matched case-control study". Lancet. 368 (9546): 1495–502. doi:10.1016/S0140-6736(06)69637-2. PMID 17071283.
- ↑ Millar EV, Watt JP, Bronsdon MA, et al. (2008). "Indirect effect of 7‐valent pneumococcal conjugate vaccine on pneumococcal colonization among unvaccinated household members". Clin Infect Dis. 47 (8): 989–996. doi:10.1086/591966. PMID 18781875.
- ↑ Siemieniuk, Reed A.C.; Gregson, Dan B.; Gill, M. John (Nov 2011). "The persisting burden of invasive pneumococcal disease in HIV patients: an observational cohort study". BMC Infectious Diseases. 11: 314. doi:10.1186/1471-2334-11-314. PMC 3226630
 . PMID 22078162. Cite uses deprecated parameter
. PMID 22078162. Cite uses deprecated parameter |coauthors=(help) - ↑ Barocchi MA, Censini S, Rappuoli R (2007). "Vaccines in the era of genomics: the pneumococcal challenge". Vaccine. 25 (16): 2963–73. doi:10.1016/j.vaccine.2007.01.065. PMID 17324490.
- ↑ Grijalva CG, Nuorti JP, Arbogast PG, Martin SW, Edwards KM, Griffin MR (April 2007). "Decline in pneumonia admissions after routine childhood immunisation with pneumococcal conjugate vaccine in the USA: a time-series analysis". Lancet. 369 (9568): 1179–86. doi:10.1016/S0140-6736(07)60564-9. PMID 17416262.
- 1 2 Tsai CJ, Griffin MR, Nuorti JP, Grijalva CG (June 2008). "Changing epidemiology of pneumococcal meningitis after the introduction of pneumococcal conjugate vaccine in the United States". Clinical Infectious Diseases. 46 (11): 1664–72. doi:10.1086/587897. PMID 18433334.
- 1 2 O'Brien KL, Wolfson LJ, Watt JP, et al. (2009). "Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates". Lancet. 374 (9693): 893–902. doi:10.1016/S0140-6736(09)61204-6. PMID 19748398.
- ↑ PneumoADIP | Need for PneumoADIP
- ↑ Johns Hopkins Bloomberg School of Public Health, International Vaccine Access Center (2013). "VIMS Report: Global vaccine introduction" (PDF).
- ↑ Wyeth Annual report