Compliance (medicine)
In medicine, compliance (also adherence, capacitance) describes the degree to which a patient correctly follows medical advice. Most commonly, it refers to medication or drug compliance, but it can also apply to other situations such as medical device use, self care, self-directed exercises, or therapy sessions. Both the patient and the health-care provider affect compliance, and a positive physician-patient relationship is the most important factor in improving compliance,[1] although the high cost of prescription medication also plays a major role.[2]
Compliance is commonly confused with concordance, which is the process by which a patient and clinician make decisions together about treatment.[3]
Worldwide, non-compliance is a major obstacle to the effective delivery of health care. Estimates from the World Health Organization (2003) indicate that only about 50% of patients with chronic diseases living in developed countries follow treatment recommendations.[1] In particular, low rates of adherence to therapies for asthma, diabetes, and hypertension are thought to contribute substantially to the human and economic burden of those conditions.[1] Compliance rates may be overestimated in the medical literature, as compliance is often high in the setting of a formal clinical trial but drops off in a "real-world" setting.[4]
Major barriers to compliance are thought to include the complexity of modern medication regimens, poor "health literacy" and lack of comprehension of treatment benefits, the occurrence of undiscussed side effects, the cost of prescription medicine, and poor communication or lack of trust between the patient and his or her health-care provider.[5][6][7] Efforts to improve compliance have been aimed at simplifying medication packaging, providing effective medication reminders, improving patient education, and limiting the number of medications prescribed simultaneously.
Terminology
An estimated half of those for whom treatment regimens are prescribed do not follow them as directed.[1] Until recently, this was termed "non-compliance", which was sometimes regarded as meaning that not following the directions for treatment was due to irrational behavior or willful ignoring of instructions. Today, health care professionals more commonly use the term "adherence" to a regimen rather than "compliance", because this term is thought to reflect better the diverse reasons for patients not following treatment directions in part or in full.[6][8] Additionally, the term adherence includes the ability of the patient to take medications as prescribed by their physician with regards to the correct drug, dose, route, timing, and frequency.[9] It is noted that compliance may only refer to passively following orders.[10] However, the preferred terminology remains a matter of debate.[11][12] In some cases, concordance is used to refer specifically to patient adherence to a treatment regimen that is designed collaboratively by the patient with the physician, to differentiate it from adherence to a physician-only prescribed treatment regimen.[13][14] Despite the ongoing debate, adherence is the preferred term for the World Health Organization,[1] The American Pharmacists Association,[5] and the U.S. National Institutes of Health Adherence Research Network.[15]
Concordance also refers to a current UK NHS initiative to involve the patient in the treatment process to improve compliance.[16] In this context, the patient is informed about their condition and treatment options. They are involved with the treatment team in the decision as to which course of action to take, and partially responsible for monitoring and reporting back to the team. Compliance with treatment can be improved by:
- Selecting treatments in a way that minimizes side-effects, and discussing management of side effects
- Prescribing the minimum number of different medications
- Simplifying dosage regimen by selecting a drug or using a sustained release preparation that requires as few doses per day as possible[17]
- Having open discussions around medication options, and alternatives if the first option is not tolerated
Societal impact
A WHO study estimates that only 50% of patients suffering from chronic diseases in developed countries follow treatment recommendations.[1] The figures are even lower in respect to adherence rates for preventative therapies, and can be as low as 28% in developed countries. citation neededThis may affect patient health, and affect the wider society when it causes complications from chronic diseases, formation of resistant infections, or untreated psychiatric illness.
Compliance rates during closely monitored studies are usually far higher than in later real-world situations. For example, one study reported a 97% compliance rate at the beginning of treatment with statins, but only about 50% of patients were still compliant after six months.[4]
The experience of Patient Connect Service Limited in the UK is that medicines prescribed for preventative purposes are especially likely not to be taken as prescribed;[18] perhaps because people do not feel immediately threatened or, in the case of symptomless conditions such as raised cholesterol levels (hypercholesterolaemia) and raised blood pressure (systemic hypertension), feel no obvious benefits at the time of taking the medicines As patients are asymptomatic, they may not see a need to take medication.
Some figures are available from the UK on non-compliance:
- up to 90% of diabetes patients do not take their medication well enough to benefit from that medication.
- 33-50% of some cancer patients take less of their anti-cancer medicine than required.
- only 75% of patients with coronary heart disease (CHD) take sufficient medicine for it to be effective.
- Up to 75% of hypertensive patients do not adhere to their medicine.
- 41-59% of mentally ill patients take their medication infrequently or not at all.[19]
- 33% of patients with schizophrenia don’t take their medicine at all, and 33% are poorly adherent.[20]
- Less than 27% of depressed patients adhere to their medication.[21]
In the UK, it has been estimated that if CHD patients adhered to their medication, each year 40,000 to 50,000 fewer people would have a stroke and 25,000 would not have a heart attack.
The financial cost to the UK National Health Service (NHS), and thus to society, is also high:
- CHD costs the NHS in excess of £2 billion on medicines; 50% of which is wasted through poor understanding and poor adherence.
- Economic studies consistently show that the costs incurred with poorly controlled asthma are higher than those for a well-controlled patient with the same severity of disease. For severe asthma, it has been estimated that the savings produced by optimal control would be around 45% of the total medical costs.[22]
Compliance issues
Health literacy
Cost and poor understanding of the directions for the treatment (referred to as 'health literacy') are major barriers to completing treatments.[23][24][25] There is robust evidence for a correlation between education and physical health. Poor educational attainment is a key factor in the cycle of health inequalities.[26][27][28]
Educational qualifications help to determine an individual’s position in the labour market, their level of income and therefore their access to resources.
Literacy
One in five adults has a long-standing illness or disability. In 2003, a national study for the UK Department of Health, more than one-third of people with poor or very poor health had literary skills of Entry Level 3 or below.[29]
Low levels of literacy and numeracy were found in 2003 to be associated with socio-economic deprivation. Adults in more deprived areas, such as the North East of England, performed at a lower level than those in less deprived areas such as the South East. Local authority tenants and those in poor health were particularly likely to lack basic skills.[30]
A 2000 analysis of over 100 UK local education authority areas found educational attainment at 15–16 years of age to be strongly associated with coronary heart disease and subsequent infant mortality.[31]
One fifth of UK adults in 1999 (nearly seven million people) had problems with basic skills, especially functional literacy and functional numeracy, making it impossible for them to effectively take medication, read labels, follow drug regimes, and find out more. This was described as:
The ability to read, write and speak in English, and to use mathematics at a level necessary to function at work and in society in general.— Moser Report (1999)
A study of the relationship of literacy to asthma knowledge revealed that 31% of asthma patients with a reading level of a ten-year-old knew they needed to see the doctors even when they were not having an asthma attack, compared to 93% with a high school graduate reading level.
Cost
In the U.S, the National Report Card on Adherence rates Americans with chronic medical conditions with a grade C+ on adherence to their medication[32] and this contributes to an estimated cost of $290 Billion annually.[33] Increase in patient medication cost share was found to be associated with low adherence to medication.[34] The United States is among the countries with the highest prices of prescription drugs which is one of factors leading to the high healthcare costs. This is mainly attributed to the government's lack of ability to negotiate lower prices with monopolies in the pharmaceutical industry especially with the brand name drugs.[35] In order to manage the medication costs, many patients on long term therapies fail to fill their prescription or skip or reduce doses. According to the Kaiser Family Foundation survey in 2015, approximately three quarters (73%) of the public think the drug prices are unreasonable and blame pharmaceutical companies for setting prices so high.[36] In the same report, half of the public reported that they are taking prescription drugs and “quarter (25%) of those currently taking prescription medicine report they or a family member have not filled a prescription in the past 12 months due to cost, and 18 percent report cutting pills in half or skipping doses”.[36] In comparison to Canada, only 8% of adults reported to have skipped their doses or not filling their prescriptions due to the cost of their prescribed medications.[37]
Age
Both young and elderly status are associated with non-adherence.
The elderly often have multiple health conditions, and around half of all NHS medicines are prescribed for people over retirement age, despite representing only about 20% of the UK population.[38][39] The recent National Service Framework on the care of older people highlighted the importance of taking and effectively managing medicines in this population. However, elderly individuals may face challenges, including multiple medications with frequent dosing, and potentially decreased dexterity or cognitive functioning. Patient knowledge is a concern that has been observed.
Cline et al. identified several gaps in knowledge about medication in elderly patients discharged from hospital.[40] Despite receiving written and verbal information, 27% of older people discharged after heart failure were classed as non-adherent within 30 days. Half the patients surveyed could not recall the dose of their medication and nearly two-thirds did not know what time of day to take them. A 2001 study by Barat et al. evaluated the medical knowledge and factors of adherence in a population of 75-year-olds living at home. They found that 40% of elderly patients do not know the purpose of their regimen and only 20% knew the consequences of non-adherence.[41] Comprehension, polypharmacy, living arrangement, multiple doctors, and use of compliance aids was correlated with adherence. A conservative estimate says 10% of all hospital admissions are through patients not managing their medication .
Adherence factors in children with various conditions have been studied. Asthma is a disease where self-management compliance is critical. Co-morbidites have been noted that affect outcomes; electronic monitoring may help.[42] Social factors of treatment adherence have been studied in the context of children and adolescent psychiatric disorders:
- Young people who felt supported by their family and doctor, and had good motivation, were more likely to comply.[43]
- Young adults may stop taking their medication in order to fit in with their friends, or because they lack insight of their illness.[43]
- Those who did not feel their condition to be a threat to their social well-being were eight times more likely to comply than those who perceived it as such a threat.[44][45]
- Non-adherence is often encountered among children and young adults; young males are relatively poor at adherence.[46][47]
Ethnicity
People of different ethnic backgrounds have unique adherence issues through literacy, physiology, culture or poverty. There are few published studies on adherence in medicine taking in ethnic minority communities. Ethnicity and culture influence some health-determining behaviour, such as participation in screening programmes and attendance at follow-up appointments.[48][49]
Prieto et al [50] also emphasised the influence that ethnic and cultural factors can have on adherence. They pointed out that groups differ in their attitudes, values and beliefs about health and illness. This view could affect adherence, particularly with preventive treatments and medication for asymptomatic conditions. Additionally, some cultures fatalistically attribute their good or poor health to their god(s), and attach less importance to self-care than others.
Measures of adherence may need to be modified for different ethnic or cultural groups. In some cases, it may be advisable to assess patients from a cultural perspective before making decisions about their individual treatment.
Prescription fill rates
While a health care provider visit with a patient may result in the patient leaving with a prescription for medication, not all patients will fill the prescription at a pharmacy. In the U.S., 20-30% of prescriptions are never filled at the pharmacy.[51][52] There are many reasons patients do not fill prescriptions including the cost of the medication,[2][5] doubting the need for medication, or preference for self-care measures other than medication.[53][54] Cost may be a barrier to prescription drug adherence, but convenience, side effects and lack of demonstrated benefit are also significant factors to a complex situation. A US nationwide survey of 1,010 adults in 2001 found that 22% chose not to fill prescriptions because of the price, which is similar to the 20-30% overall rate of unfilled prescriptions.[2] However, analysis by health insurers suggest that patient co-payment requirements can be reduced to $0 with little or no improvement in long-term adherence rates.
Prescription medical claims records are commonly used to estimate medication adherence based on fill rate. Patients are routinely defined as being 'Adherent Patients' if the amount of medication furnished to the patient is at least 80% based on days supply of medication divided by the number of days patient should be consuming the medication. This quantity is defined as the medication possession ratio (MPR). However, recent work by several investigators has suggested that MPR of 90% or above may be a better threshold for deeming consumption as 'Adherent'.[55]
Medication Possession Ratio
There are two forms of MPR that can be calculated, fixed and variable.[56] The calculation of either is relatively straightforward, for Variable MPR (VMPR) it is calculated as the number of days supply divided by the number of elapsed days including the last prescription.

For the Fixed MPD (FMPT) the calculation is similar but the denominator is the number of days in a year whilst the numerator is constrained to be the number of days supply within the year that the patient has been prescribed.

For medication in tablet form it is relatively straightforward to calculate the number of days supply based on a prescription. Some medications are less straightforward though because a prescription of a given number of doses may have a variable number of days supply because the number of doses to be taken per-day varies, for example with preventative corticosteroid inhalers prescribed for asthma where the number of inhalations to be taken daily may vary between individuals based on the severity of the disease.
Course completion
Once started, patients seldom follow treatment regimens as directed, and seldom complete the course of treatment.[5][6] In respect of hypertension, 50% of patients completely drop out of care within a year of diagnosis.[57] Persistence with first-line single antihypertensive drugs is extremely low during the first year of treatment.[58] As far as lipid-lowering treatment is concerned, only one third of patients are compliant with at least 90% of their treatment.[59]
As mentioned previously, the World Health Organization (WHO) has estimates that only 50% of people complete long-term therapy for chronic illnesses as they were prescribed, which puts patient health at risk.[60] For example, statin compliance drops to between 25-40% after two years of treatment, with patients taking statins for what they perceive to be preventative reasons being unusually poor compliers.[61]
A wide variety of packaging approaches have been proposed to help patients complete prescribed treatments. These approaches include formats that increase the ease of remembering the dosage regimen as well as different labels for increasing patient understanding of directions.[62][63] For example, medications are sometimes packed with reminder systems for the day and/or time of the week to take the medicine.[62] With the objective to support patient adherence to medicinal therapy, a not-for-profit organization called the Healthcare Compliance Packaging Council of Europe (HCPC-Europe) was set up between the pharmaceutical industry, the packaging industry and representatives of European patients organizations. The mission of HCPC-Europe is to assist and to educate the healthcare sector in the improvement of patient compliance through the use of packaging solutions. A variety of packaging solutions have been developed by this collaboration to aid in patient compliance.
The failure to complete treatment regimens as prescribed has significant negative health impacts worldwide.[1] Examples of the rate and consequences of non-compliance for selected medical disorders is as follows:
Asthma
Asthma non-compliance (28-70% worldwide) increase the risk of severe asthma attacks requiring preventable ER visits and hospitalizations.
Compliance issues with Asthma can be caused by a variety of reasons including: difficult inhaler use, side effects of medications, and cost of the treatment.[64]
Since Asthma is an ongoing disease and patients may go through periods where they do not have symptoms, this can interfere with proper use of steroid inhalers. Steroid inhalers need to be taken on a daily basis even if the patient is feeling well. The only time that it is allowable to stop taking a steroid inhaler is with a doctor's approval.[65]
Cancer
200,000 new cases of cancer are diagnosed each year in the UK. One in three adults in the UK will develop cancer that can be life-threatening, and 120,000 people will be killed by their cancer each year. This accounts for 25% of all deaths in the UK. However:
- 90% of cancer pain can be effectively treated, yet only 40% of patients adhere to their medicines due to poor understanding.
The reasons for non-adherence have been given by patients as follows:
- The poor quality of information available to them about their treatment.
- A lack of knowledge as to how to raise concerns whilst on medication.
- Concerns about unwanted effects.
- Issues about remembering to take medication.
Partridge et al (2002) [66] identified evidence to show that adherence rates in cancer treatment are variable, and sometimes surprisingly poor. The following table is a summary of their findings:
| Type of Cancer | Measure of non-Adherence | Definition of non-Adherence | Rate of Non-Adherence |
|---|---|---|---|
| Haematological malignancies | Serum levels of drug metabolites | Serum levels below expected threshold | 83% |
| Breast Cancer | Self-report | Taking less than 90% of prescribed medicine | 47% |
| Leukemia or non Hodgkin's lymphoma | Level of drug metabolite in urine | Level lower than expected | 33% |
| Leukemia, Hodgkin's disease, non Hodgkin's | Self-report and parent report | More than one missed dose per month | 35% |
| Lymphoma, other malignancies | Serum bioassay | Not described | |
| Hodgkin's disease, acute lymphocytic leukemia (ALL) | Biological markers | Level lower than expected | 50% |
| ALL | Level of drug metabolite in urine | Level lower than expected | 42% |
| ALL | Level of drug metabolites in blood | Level lower than expected | 10% |
| ALL | Level of drug metabolites in blood | Level lower than expected | 2% |
- Medication event monitoring system - a medication dispenser containing a microchip that records when the container is opened and from Partridge et al (2002)
Other trials evaluating Tamoxifen as a preventative agent have shown dropout rates of around one-third:
- 36% in the Royal Marsden Tamoxifen Chemoprevention Study.[67]
- 29% in the National Surgical Adjuvant Breast and Bowel Project.[68]
According to correspondence in the Lancet in March 1999,[69] the "Adherence in the International Breast Cancer Intervention Study" (evaluating the effect of a daily dose of Tamoxifen for five years in ‘at risk’ women aged 35–70 years) was:
- 90% after one year
- 83% after two years
- 74% after four years
Coronary heart disease
In one study, patients who did not adhere to beta-blocker therapy were found to be 4.5 times more likely to have complications of coronary heart disease than those who do comply.
Diabetes
- Diabetes non-compliance (98% in US) is the principal cause of complications related to diabetes including nerve damage and kidney failure.
- Among patients with Type 2 Diabetes, adherence is found in less than one-third of those prescribed sulphonylureas and/or metformin. Patients taking both drugs achieve only 13% adherence.[70]
Hypertension
- Hypertension non-compliance (93% in US, 70% in UK) is the main cause of uncontrolled hypertension-associated heart attack and stroke.
- In respect of anti-hypertensive therapy, only about 50% take at least 80% of their prescribed medications.[71]
Health and disease management
Asthma
To help manage adherence in asthma patients, the most important factors in improving compliance included patient education, motivational interviewing, and setting goals of therapy. Explaining the differences between the types of inhalers and telling patients that steroid inhalers will need to be taken every day can help to improve adherence in this population.[72]
Diabetes
Patients with diabetes are at high risk of developing coronary heart disease and usually have related conditions that make their treatment regimens even more complex. These related conditions, such as hypertension, obesity and depression are also characterised by poor rates of adherence, and therefore exacerbate treatment outcomes.[73][74]
Hypertension
As a result of poor compliance, 75% of patients with a diagnosis of hypertension do not achieve optimum blood-pressure control.
Schizophrenia
There is a clear correlation between adherence with medication regimens and factors such as: relapse rates; hospitalisation rates; re-hospitalisation rates; incidence of serious unwanted events, including suicides; assaults or severe violence.
Non-adherent schizophrenic patients are over three times more likely to relapse than patients who take their medication. [75]
Stroke
Survivors of stroke or heart attack frequently have disability and worse health:
- 15-50% of stroke patients suffer with major depression.
- 20% will go on to develop dementia as a result of the stroke.
- Faecal incontinence is common after a severe stroke, bringing stress to both the individual and the family.
- 5% will have untreatable severe pain, that dominates their life.
Improving compliance rates
Patients' adherence with their medication is poor across all chronic diseases, including coronary heart disease, mental health, diabetes and cancer. This poor adherence results in significant increase in illness, disability, symptoms and even death.
Care in choice of medicine by the prescribing physician, along with and the provision of greater information to the patient can improve compliance. For example, patients taking typical antipsychotics tend to experience more severe side-effects, and also receive less information about their illness, medicines and side-effects.[76] They were naturally more likely to be non-compliant than those receiving atypicals.
The role of health care providers
Health care providers play a great role in improving adherence issues. Providers can improve patient interactions through motivational interviewing and active listening.[77]
Health care providers should work with patients to devise a plan that is meaningful for the patient’s needs. A relationship that offers trust, cooperation, and mutual responsibility can greatly improve the connection between provider and patient for a positive impact.[10]
Technology
As more patient cohorts become adept at using technology in their daily lives, it will become easier to integrate technology into patient care and compliance. Already there are multiple opportunities to use technology to boost patient compliance rates, and make it easier for patients to become involved in their own care. As part of the push to encourage implementation of electronic health records in hospitals and private practices, the US government has set "meaningful use" objectives and benchmarks. One such objective is the use of a patient portal, through which patients can securely view lab reports, request prescription refills, and ask questions of their providers - all of which can increase patient compliance with care plans.
Another medium to boost compliance is mobile technology. Both physicians and patients are using tablets, smartphones, and other devices in increasing numbers, all of which can be equipped with any number of medical apps to help with patient monitoring and compliance. Text-message reminders are increasingly being used to help with patient compliance; studies show that daily text messages sent to remind patients to take their medication have improved compliance rates and patient health - especially in younger patients with chronic illnesses such as diabetes, and young women who take contraceptives. [78] [79]
As telemedicine technology improves, physicians will have better capabilities to remotely monitor patients in real-time and to communicate recommendations and medication adjustments as the situation demands, rather than waiting until the next office visit. Telemedicine using personal mobile devices, such as smartphones, will become increasingly important for monitoring patients with chronic conditions such as cardiovascular disease and diabetes.[80]
Medication Event Monitoring Systems, in the form of smart medicine bottle tops (MEMS or eCAP), smart pharmacy vials (eCAP or NantHealth's GlowCap) or smart blister packages (Med-ic or Cerepak) are frequently used in clinical trial and other applications where exact compliance data are required. Such systems usually work without any patient input, and record the time and date the bottle or vial was accessed, or the medication removed from a blister package. The data can be read via proprietary readers, or NFC enabled devices, such as smartphones or tablets. There is evidence that the use of such devices can help improve e.g. control of hypertension.[81]
There have been a number of initiatives involving "real time" adherence monitoring. What "real time" means is debatable. A "talking pill" or one which can communicate its status on an ongoing real time basis is not feasible. In all cases, the medication taking event is represented in a system by proxy. For instance, the time a trace was broken on a package when a dose cavity was accessed. In this case there is no proof that the medication was a) removed or b) ingested. Proof of ingestion and the time staying of it is in and by itself a difficult task to accomplish. While sounding most useful and technically feasible, it has not been meeting with much success to-date. Even the most cutting-edge ingestion based product, Proteus' Helio, requires the ingestion of a non-active second dose enabled with a transmitting function. Again, it doesn't prove ingestion of the active dose at all. It is debatable how much acceptance this type of ingested sensor will have with the general public. At the moment, a prescription is required just to receive a sensor system.
In most parts of the world, medication is dispensed in blister packaging. It is relatively simple to equip blister packages with printed conductive trace grids. These grids are then connected to an electronic module (Such as Med-ic Electronic Compliance Monitor by Information Mediary Corp.). The electronic monitor records the time a trace has been broken and can then transmit this information to an NFC smart phone or even be GSM enabled to transmit the information immediately if a suitable data network is available. A more reasonable solution at the moment would be to connect the package to a hub, handheld device, tablet or smart watch via low power BlueTooth. In this case the package data would be sent whenever the medication blister is in close proximity to the bluetooth receiver. It avoids the huge effort required to equip every single blister with a SIM module and expensive monthly data subscription.
The question of real time is not solved by simply generating data which is based on a proxy of ingestion. If such data isn't being parsed and used in an effective fashion to assist patients, caregivers and medical professionals with adherence management, then it is not a useful application of expensive resources. It can be argued that the highest and best use of technologies such as smart blister packages, are in stratifying patient groups into good compliers and poor compliers. In this case, the poor compliers maybe coached more intensively, and the good compliers have a continued incentive to remain adherent. Real time in this case might be achieved by sending a regular series of SMS, frequency depending on their adherence status, and requesting them to upload their NFC sensor data through their handheld or wrist worn device.
There appears to be as much confusion about smart adherence technology as there is whenever a new technology comes on stream. Overzealous journalists tend to confuse science fiction with reality. Marketers and PR departments over promise and engineering and product departments under deliver. In the end, if a fair balance isn't struck between a feasible cost effective solution and unrealistic expectations derived from over confident presentations, the entire field of smart adherence monitoring is in danger of being ignored.
For the time being, the most applicable field of endeavour for smart adherence management is in clinical trials. This is also where most of the existing devices are being used at the moment.
Patient information
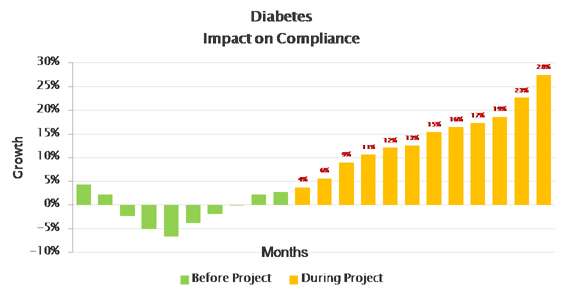
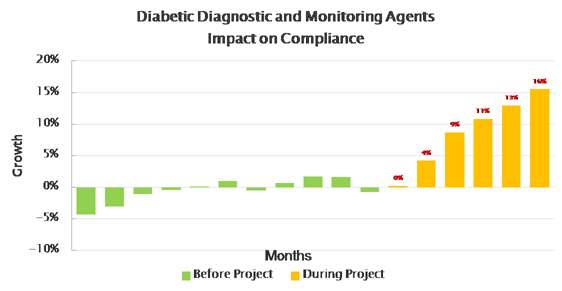
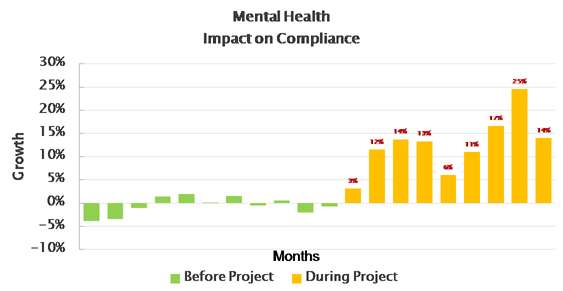
In the UK millions of patients are given information at the point of dispensing to help them better understand their medicines, with measurable impact on patient compliance.
In the UK, a literature service and its pharmacy partners have together completed a 200,000 patient study into the effect of pharmacists providing to patients the information that patients want. The results of the survey show that where a pharmacist talks through the leaflet given to the patient, then there is an increase in adherence by between 16% and 33% within three months.[82]
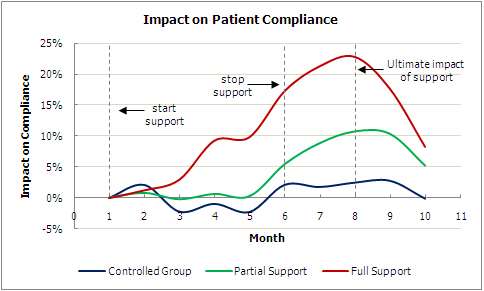
Since then, millions of patients have been supported, and had measurable impact across the following therapy areas:

See also
References
- 1 2 3 4 5 6 7 World Health Organization (2003). Adherence to long-term therapies: evidence for action (PDF). Geneva: World Health Organisation. ISBN 92-4-154599-2.
- 1 2 3 "Out-of-pocket costs may be a substantial barrier to prescription drug compliance" (PDF). Harris Interactive. Retrieved May 12, 2010.
- ↑ "Medicines concordance (involving patients in decisions about prescribed medicines)". National Institute for Health and Clinical Excellence. 3 March 2008.
- 1 2 "Patient Compliance with statins". Bandolier. 2004.
- 1 2 3 4 "Enhancing Patient Adherence: Proceedings of the Pinnacle Roundtable Discussion". APA Highlights Newsletter. October 2004.
- 1 2 3 Ngoh LN (2009). "Health literacy: a barrier to pharmacist-patient communication and medication adherence". J Am Pharm Assoc (2003). 49 (5): e132–46; quiz e147–9. doi:10.1331/JAPhA.2009.07075. PMID 19748861.
- ↑ Elliott RA, Marriott JL (2009). "Standardised assessment of patients' capacity to manage medications: a systematic review of published instruments". BMC Geriatr. 9: 27. doi:10.1186/1471-2318-9-27. PMC 2719637
 . PMID 19594913.
. PMID 19594913. - ↑ Tilson HH (2004). "Adherence or compliance? Changes in terminology". Annals of Pharmacotherapy. 38 (1): 161–2. doi:10.1345/aph.1D207. PMID 14742813.
- ↑ Viswanathan M, Golin CE, Jones CD, Ashok M, Blalock S, Wines RCM, Coker-Schwimmer EJL, Grodensky CA, Rosen DL, Yuen A, Sista P, Lohr KN. Medication Adherence Interventions: Comparative Effectiveness. Closing the Quality Gap: Revisiting the State of the Science. Evidence Report No. 208. (Prepared by RTI International–University of North Carolina Evidence-based Practice Center under Contract No. 290-2007-10056-I.) AHRQ Publication No. 12-E010-EF. Rockville, MD: Agency for Healthcare Research and Quality. September 2012. www.effectivehealthcare.ahrq.gov/reports/final.cfm.
- 1 2 Rifaat Nizar; Abdel-Hady Elham; Hasan Ali A. "The golden factor in adherence to inhaled corticosteroid in asthma patients". Egyptian Journal of Chest Diseases and Tuberculosis. 62 (3): 371–376. doi:10.1016/j.ejcdt.2013.07.010.
- ↑ Osterberg L, Blaschke T (2005). "Adherence to Medication". N Engl J Med. 353 (5): 487–97. doi:10.1056/NEJMra050100. PMID 16079372.
- ↑ Aronson JK (2007). "Compliance, concordance, adherence". Br J Clin Pharmacol. 63 (4): 383–4. doi:10.1111/j.1365-2125.2007.02893.x. PMC 2203247. PMID 17378797.
- ↑ Bell JS, Airaksinen MS, Lyles A, Chen TF, Aslani P (2007). "Concordance is not synonymous with compliance or adherence". Br J Clin Pharmacol. 64 (5): 710–1. doi:10.1111/j.1365-2125.2007.02971_1.x. PMC 2203263. PMID 17875196.
- ↑ US NIH Office of Behavior and Social Sciences Research (2008). "Framework for adherence research and translation: a blueprint for the next ten years" (PDF).
- ↑ Office of Behavior and Social Sciences Research. "Adherence Research Network". U.S. National Institutes of Health. Retrieved 12 May 2010.
- ↑ Marinker and Shaw (15 February 2003). "Not to be taken as directed - Putting concordance for taking medicines into practice". BMJ. 326 (7385): 348–9. doi:10.1136/bmj.326.7385.348.
- ↑ "Dosing and compliance?". Bandolier. 117. Figure 1. November 2003.
- ↑ "Home page". Patient Connect. Retrieved 12 July 2013.
- ↑ Dolder CR, Lacro JP, Leckband S, Jeste DV (2003). "Interventions to improve antipsychotic medication adherence: Review of recent literature". Journal of Clinical Psychopharmacology. 23 (4): 389–399. doi:10.1097/01.jcp.0000085413.08426.41. PMID 12920416.
- ↑ Oehl M, Hummer M, Fleischhacker WW (2000). "Adherence with antipsychotic treatment". Acta Psychiatrica Scaninavia. 102 (Suppl. 407): 83–86. doi:10.1034/j.1600-0447.2000.00016.x.
- ↑ Colom F, Vieta E, Martinez-Aran A, Reinares M, Benabarre A, Gasto C (2000). "Clinical factors associated with treatment non-adherence in euthymic bipolar patients". Journal of Clinical Psychiatry. 61 (8): 549–555. doi:10.4088/JCP.v61n0802. PMID 10982196.
- ↑ GINA Project (Global Initiative for Asthma) 2002.
- ↑ "Enhancing Patient Adherence: Proceedings of the Pinnacle Roundtable Discussion". APA Highlights Newsletter. October 2004.
- ↑ Ngoh LN (2003). "Health literacy: a barrier to pharmacist-patient communication and medication adherence". J Am Pharm Assoc. 49 (5): e132–46; quiz e147–9. doi:10.1331/JAPhA.2009.07075. PMID 19748861.
- ↑ Elliott RA, Marriott JL (2009). "Standardised assessment of patients' capacity to manage medications: a systematic review of published instruments". BMC Geriatr. 9: 27. doi:10.1186/1471-2318-9-27. PMC 2719637. PMID 19594913.
- ↑ Donald Acheson (1998). Independent inquiry into inequalities in health (Report).
- ↑ Tackling health inequalities (Report). HM Government. 2002.
- ↑ Park DC, Hertzog C, Leventhal H, Morrell RW, Leventhal E, Birchmore D, Martin M, Bennett J (1999). "Medication adherence in rheumatoid arthritis patients: older is wiser". Journal of the American Geriatric Society. 47 (2): 172–183.
- ↑ Williams J, Clemens S, Oleinikova K, Tarvin K (2003). "The skills for life survey. A national needs and impact survey of literacy, numeracy and ICT skills". London: Department for Education and Skills
- ↑ Williams J, Clemens S, Oleinikova K, Tarvin K (2003). "The skills for life survey. A national needs and impact survey of literacy, numeracy and ICT skills". London: Department for Education and Skills.
- ↑ "Cross-cutting government review, Tackling health inequalities". Department of Health and Treasury. 2000
- ↑ National Medical Report Card, 2013 Report
- ↑ Thinking Outside the Pillbox: A System-wide Approach to Improving Patient Adherence for Chronic Disease.” NEHI. 2009
- ↑ Eaddy MT, Cook CL, O’Day K, Burch SP, Cantrell CR. How Patient Cost-Sharing Trends Affect Adherence and Outcomes: A Literature Review. Pharmacy and Therapeutics. 2012;37(1):45-55
- ↑ Kesselheim AS, Avorn J, Sarpatwari A. The High Cost of Prescription Drugs in the United States Origins and Prospects for Reform. JAMA. 2016;316(8):858-871. doi:10.1001/jama.2016.11237
- 1 2 Kaiser Family Foundation: Poll Finds Nearly Three Quarters of Americans Say Prescription Drug Costs Are Unreasonable, and Most Blame Drug Makers Rather Than Insurers for the Problem
- ↑ Kennedy, Jae; Morgan, Steve. "Cost-related prescription nonadherence in the united states and Canada: A system-level comparison using the 2007 international health policy survey in seven countries". Clinical Therapeutics. 31(1): 213–219. doi:10.1016/j.clinthera.2009.01.006
- ↑ UK Department of Health (2001): National Service Framework for Older People, London.
- ↑ UK Office of Health Economics (2000): Compendium of Health Statistics, 12th Edition, London.
- ↑ Cline CM, Bjorck-Linne AK, Israelsson BY, Willenheimer RB, Erhardt LR (1999). "Non-adherence and knowledge of prescribed medication in elderly patients with heart failure". European Journal of Heart Failure. 1 (2): 145–149. doi:10.1016/S1388-9842(99)00014-8. PMID 10937924.
- ↑ Barat I, Andreasen F, Damsgaard EM (2001). "Drug therapy in the elderly: what doctors believe and patients actually do". British Journal of Clinical Pharmacology. 51 (6): 615–622. doi:10.1046/j.0306-5251.2001.01401.x. PMC 2014493. PMID 11422022.
- ↑ "Exploring the impact of elevated depressive symptoms on the ability of a tailored asthma intervention to improve medication adherence among urban adolescents with asthma.". Allergy Asthma Clin Immunol. 9: 45. Nov 2013. doi:10.1186/1710-1492-9-45. PMID 24479403.
- 1 2 "An Approach to Maximizing Treatment Adherence of Children and Adolescents with Psychotic Disorders and Major Mood Disorders". Can Child Adolesc Psychiatr Rev. 14: 106–13. Nov 2005. PMC 2553227. PMID 19030524.
- ↑ Mitchell WG, Scheier LM, Baker SA (2000). "Adherence to treatment in children with epilepsy: who follows 'doctor's orders'?". Epilepsia. 41 (12): 1616–25. doi:10.1111/j.1499-1654.2000.001616.x. PMID 11114221.
- ↑ Otero S, Hodes M (2000). "Maternal expressed emotion and treatment Adherence of children with epilepsy". Dev Med child Neurol. 42 (9): 604–8. doi:10.1017/S0012162200001134. PMID 11034453.
- ↑ Dolder CR, Lacro JP, Dunn LB, Jeste DV (2002). "Antipsychotic medication adherence: Is there a difference between typical and atypical agents?". American Journal of Psychiatry. 159 (1): 103–108. doi:10.1176/appi.ajp.159.1.103. PMID 11772697.
- ↑ Nosé M, Barbui C, Gray R, Tansella M (2003). "Clinical interventions for treatment non-adherence in psychosis: meta-analysis". British Journal of Psychiatry. 183 (3): 197–206. doi:10.1192/bjp.183.3.197. PMID 12948991.
- ↑ Courtenay WH, McCreary DR, Merighi JR (2002). "Gender and ethnic differences in health beliefs and behaviours". Journal of Health Psychology. 7 (3): 219–231. doi:10.1177/1359105302007003216. PMID 22114246.
- ↑ Meyerowitz BE, Richardson J, Hudson S, Leedham B (1998). "Ethnicity and cancer outcomes: behavioural and psychosocial considerations". Psychological Bulletin. 123 (1): 47–70. doi:10.1037/0033-2909.123.1.47. PMID 9461853.
- ↑ Prieto LR, Miller DS, Gayowski T, Marino IR (1997). "Multicultural issues in organ transplantation: the influence of patients' cultural perspectives on adherence with treatment". Clinical Transplantation. 11 (6): 529–535. PMID 9408680.
- ↑ Fischer MA, Stedman MR, Lii J, et al. (April 2010). "Primary medication non-adherence: analysis of 195,930 electronic prescriptions". J Gen Intern Med. 25 (4): 284–90. doi:10.1007/s11606-010-1253-9. PMC 2842539. PMID 20131023.
- ↑ Norton M (2010). "Many patients may not fill their prescriptions". Reuters Health. Retrieved May 12, 2010.
- ↑ Shah NR, Hirsch AG, Zacker C, Taylor S, Wood GC, Stewart WF (February 2009). "Factors associated with first-fill adherence rates for diabetic medications: a cohort study". J Gen Intern Med. 24 (2): 233–7. doi:10.1007/s11606-008-0870-z. PMC 2629003. PMID 19093157.
- ↑ Shah NR, Hirsch AG, Zacker C, et al. (April 2009). "Predictors of first-fill adherence for patients with hypertension". Am. J. Hypertens. 22 (4): 392–6. doi:10.1038/ajh.2008.367. PMC 2693322. PMID 19180061.
- ↑ Watanabe JH, Bounthavong M, Chen T. Revisiting the medication possession ratio threshold for adherence in lipid management. Curr Med Res Opin. 2013 Mar;29(3):175-80. doi: 10.1185/03007995.2013.766164. Epub 2013 Feb 1. PubMed PMID 23320610.
- ↑ Kozma CM, Dickson M, Phillips AL, Meletiche D (2013). "Medication possession ratio: implications of using fixed and variable observation periods in assessing adherence with disease-modifying drugs in patients with multiple sclerosis". Patient Prefer Adherence. 7: 509–516. doi:10.2147/PPA.S40736.
- ↑ Mapes RE (1977). "Physicians' drug innovation and relinquishment". Social Science & Medicine. 11 (11–13): 619–24. doi:10.1016/0037-7856(77)90044-0.
- ↑ Mazzaglia G, Mantovani LG, Sturkenboom M, Filippi A, Trifiro G, Cricelli C, Brignoli O, Caputi AP (November 2005). "Patterns of persistence with antihypertensive medications in newly diagnosed hypertensive patients in Italy: a retrospective cohort study in primary care". Hypertens. 23 (11): 2093–100.
- ↑ Sung JC; et al. (Oct 1998). "Factors affecting patient compliance with antihyperlipidemic medications in an HMO population". Am J Manag Care. 4 (10): 1421–30. PMID 10338735.
- ↑ World Health Organization (2003). Adherence to long-term therapies: evidence for action (PDF). Geneva: World Health Organisation. ISBN 92-4-154599-2.
- ↑ Jackevicius CA; et al. (2002). "Adherence with statin therapy in elderly patients with and without acute coronary syndromes". JAMA. 288 (4): 462–467. doi:10.1001/jama.288.4.462. PMID 12132976.
- 1 2 Heneghan CJ, Glasziou P, Perera R (2006). Heneghan CJ, ed. "Reminder packaging for improving adherence to self-administered long-term medications". Cochrane Database Syst Rev (1): CD005025. doi:10.1002/14651858.CD005025.pub2. PMID 16437510.
- ↑ Shrank W, Avorn J, Rolon C, Shekelle P (May 2007). "Effect of content and format of prescription drug labels on readability, understanding, and medication use: a systematic review". Annals of Pharmacotherapy. 41 (5): 783–801. doi:10.1345/aph.1H582. PMID 17426075.
- ↑ Bender BG, Bender SE (2005). "Patient-identified barriers to asthma treatment adherence: responses to interviews, focus groups, and questionnaires". Immunol Allergy Clin North Am. 25: 107–130. doi:10.1016/j.iac.2004.09.005.
- ↑ http://www.asthma.partners.org/newfiles/inhaledsteroids.html
- ↑ Partridge AH, Avorn J, Wang PS, Winer EP (2002). "Adherence to therapy with oral antineoplastic agents". Journal of the National Cancer Institute. 94 (9): 652–61. doi:10.1093/jnci/94.9.652. PMID 11983753.
- ↑ Powels T, Eeles R, Ashley S, et al. (1998). "Interim analysis of the incidence of breast cancer in the Royal Marsden Hospital Tamoxifen randomized chemoprevention trial". Lancet. 352 (9122): 98–101. doi:10.1016/S0140-6736(98)85012-5. PMID 9672274.
- ↑ Fisher B, Costantino JP, Wickerham DL, et al. (1998). "Tamoxifen for prevention of breast cancer: report of the National Surgical Adjuvant Breast and Bowel Projects P-1 Study". Journal of the National Cancer Institute. 90 (18): 1371–88. doi:10.1093/jnci/90.18.1371. PMID 9747868.
- ↑ Cuzick J, Edwards R (1999). "Drop-outs in Tamoxifen prevention trials". Lancet. 353 (9156): 930. doi:10.1016/S0140-6736(05)75043-1.
- ↑ Donnan PT, MacDonald TM, Morris AD (2002). "Adherence to prescribed oral hypoglyacaemic medication in a population of patients with Type 2 diabetes: a retrospective cohort study". Diabetic Medicine. 19 (4): 279–84. doi:10.1046/j.1464-5491.2002.00689.x. PMID 11942998.
- ↑ David l; et al. (1975). "Randomised clinical trial of strategies for improving medication compliance in primary hypertension". Lancet. 305 (7918): 1205–7. doi:10.1016/S0140-6736(75)92192-3. PMID 48832.
- ↑ Walker L.; Cluley S.; Fabbri L. (2000). "Improving patient compliance with asthma therapy". Respiratory Medicine. 94 (1): 2–9. doi:10.1053/rmed.1999.0667.
- ↑ Lustman PJ, Griffiths LS, Clouse RE (1997). "Depression in adults with diabetes". Seminars in Clinical Neuropsychiatry. 2 (1): 15–23. doi:10.1053/SCNP00200015. PMID 10320439.
- ↑ Ciechanowski PS, Katon WJ, Russo JE (2000). "Depression and diabetes: impact of depression symptoms pn adherence, function, and costs". Archives of Internal Medicine. 27 (21): 3278–85. doi:10.1001/archinte.160.21.3278.
- ↑ Fenton WS, Blyler CR, Heinssen RK (1997). "Determinants of medication adherence in schizophrenia: empirical and clinical findings". Schizophrenia Bulletin. 23 (4): 637–51. doi:10.1093/schbul/23.4.637. PMID 9366000.
- ↑ Hogman G, Sandamas G. A question of choice National Schizophrenia Fellowship. (2000)
- ↑ Stefanacci, Richard G., DO, MGH, MBA, AGSF, CMD, and Scott Guerin, PhD. "Why Medication Adherence Matters To Patients, Payers, Providers." Managed Care Jan. 2013. Accessed Nov 2, 2014
- ↑ Kurt Ullman, "Texting boosts OC compliance" MedPage Today, January 2012.
- ↑ Adherely, "Existing Technologies" video verification tool for medical adherence in pharmaceutical clinical trials., January 2012.
- ↑ Marisa Torrieri, "Patient compliance: technology tools for physicians" Physicians Practice, September 2012.
- ↑ Santschi, V; Chiolero, A; Burnier, M (Nov 2009). "Electronic monitors of drug adherence: tools to make rational therapeutic decisions.". Journal of Hypertension. 27 (11): 2294–5; author reply 2295. doi:10.1097/hjh.0b013e328332a501. PMID 20724871.
- ↑ http://icarehealthit.com/wp-content/uploads/2013/03/White-Paper-Care-Coordination-and-Coaching.pdf
External links
- Adherence to long-term therapies, a report from the World Health Organization
- Ten hurdles to patient adherence
- Application for monitoring therapy compliance
- Technology report on NFC enabled smart medication packages