Muscle atrophy
| Muscle atrophy | |
|---|---|
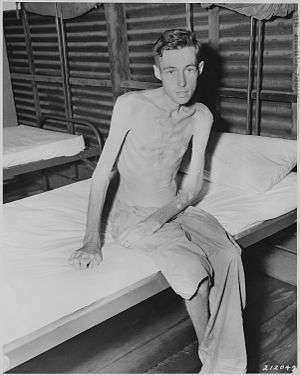 | |
| Prisoner of war exhibiting muscle loss as a result of malnutrition | |
| Classification and external resources | |
| Specialty | rheumatology, neurology |
| ICD-10 | M62.5 |
| ICD-9-CM | 728.2 |
| DiseasesDB | 29472 |
| MedlinePlus | 003188 |
| MeSH | D009133 |
Muscle atrophy is defined as a decrease in the mass of the muscle; it can be a partial or complete wasting away of muscle, and is most commonly experienced when persons suffer temporary disabling circumstances such as being restricted in movement and/or confined to bed as when hospitalized. When a muscle atrophies, this leads to muscle weakness, since the ability to exert force is related to mass. Modern medicine's understanding of the quick onset of muscle atrophy is a major factor behind the practice of getting hospitalized patients out of bed and moving about as active as possible as soon as is feasible, despite sutures, wounds, broken bones and pain.
Muscle atrophy results from a co-morbidity of several common diseases, including cancer, AIDS, congestive heart failure, COPD (chronic obstructive pulmonary disease), renal failure, and severe burns; patients who have "cachexia" in these disease settings have a poor prognosis. Moreover, starvation eventually leads to muscle atrophy.
Disuse of the muscles, such as when muscle tissue is immobilized for even a few days of unuse – when the patient has a primary injury such as an immobilized broken bone (set in a cast or immobilized in traction), for example – will also lead rapidly to disuse atrophy. Minimizing such occurrences as soon as possible is a primary mission of occupational and physical therapists employed within hospitals working in co-ordination with orthopedic surgeons.
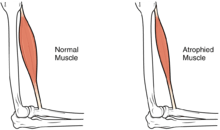
Neurogenic atrophy, which has a similar effect, is muscle atrophy resulting from damage to the nerve which stimulates the muscle, causing a shriveling around otherwise healthy limbs. Also, time in a circa zero g environment without exercise will lead to atrophy. This is partially due to the smaller amount of exertion needed to move about, and the fact that muscles are not used to maintain posture. In a similar effect, patients with a broken leg joint undergoing as little as three weeks of traction can lose enough back and buttocks muscle mass and strength as to have difficulty sitting without assistance, and experience pain, stress and burning even after a very short ten-minute exposure, when such positioning is contrived during recovery.
Signs and symptoms
Muscular atrophy decreases qualities of life as the sufferer becomes unable to perform certain tasks or worsen the risks of accidents while performing those (like walking). Muscular atrophy increases the risks of falling in conditions such as IBM (inclusion body myositis). Muscular atrophy affects a high number of the elderly.
Causes
There are many diseases and conditions which cause a decrease in muscle mass, known as atrophy, including: inactivity, as seen when a cast is put on a limb, or upon extended bedrest (which can occur during a prolonged illness); cachexia - which is a syndrome that is a co-morbidity of cancer and congestive heart failure; chronic obstructive pulmonary disease; burns, liver failure, etc., and the wasting Dejerine-Sottas syndrome (HMSN Type III). Glucocorticoids, a class of medications used to treat allergic and other inflammatory conditions can induce muscle atrophy by increasing break-down of muscle proteins.[1] Other syndromes or conditions which can induce skeletal muscle atrophy are liver disease, and starvation.
Pathophysiology
Muscle atrophy occurs by a change in the normal balance between protein synthesis and protein degradation. During atrophy, there is a down-regulation of protein synthesis pathways, and an activation of protein degradation.[2] The particular protein degradation pathway which seems to be responsible for much of the muscle loss seen in a muscle undergoing atrophy is the ATP-dependent ubiquitin/proteasome pathway. In this system, particular proteins are targeted for destruction by the ligation of at least four copies of a small peptide called ubiquitin onto a substrate protein. When a substrate is thus "poly-ubiquitinated", it is targeted for destruction by the proteasome. Particular enzymes in the ubiquitin/proteasome pathway allow ubiquitination to be directed to some proteins but not others - specificity is gained by coupling targeted proteins to an "E3 ubiquitin ligase". Each E3 ubiquitin ligase binds to a particular set of substrates, causing their ubiquitination.
Diagnosis
Quantification
A CT scan can distinguish muscle tissue from other tissues and thereby estimate the amount of muscle tissue in the body.
Fast loss of muscle tissue (relative to normal turnover), can be approximated by the amount of urea in the urine. The equivalent nitrogen content (in gram) of urea (in mmol) can be estimated by the conversion factor 0.028 g/mmol.[3] Furthermore, 1 gram of nitrogen is roughly equivalent to 6 gram of protein, and 1 gram of protein is roughly equivalent to 4 gram of muscle tissue. Subsequently, in situations such as muscle wasting, 1 mmol of excessive urea in the urine (as measured by urine volume in litres multiplied by urea concentration in mmol/l) roughly corresponds to a muscle loss of 0.67 gram.
Differential diagnosis
During aging, there is a gradual decrease in the ability to maintain skeletal muscle function and mass. This condition is called "sarcopenia". The exact cause of sarcopenia is unknown, but it may be due to a combination of the gradual failure in the "satellite cells" which help to regenerate skeletal muscle fibers, and a decrease in sensitivity to or the availability of critical secreted growth factors which are necessary to maintain muscle mass and satellite cell survival.
In addition to the simple loss of muscle mass (atrophy), or the age-related decrease in muscle function (sarcopenia), there are other diseases which may be caused by structural defects in the muscle (muscular dystrophy), or by inflammatory reactions in the body directed against muscle (the myopathies).
Treatment
Muscle atrophy can be opposed by the signaling pathways which induce muscle hypertrophy, or an increase in muscle size. Therefore, one way in which exercise induces an increase in muscle mass is to downregulate the pathways which have the opposite effect.
β-hydroxy β-methylbutyrate (HMB), a metabolite of leucine which is sold as a dietary supplement, has demonstrated efficacy in preventing the loss of muscle mass in several muscle wasting conditions in humans, particularly sarcopenia.[4][5][6] A growing body of evidence supports the efficacy of HMB as a treatment for reducing, or even reversing, the loss of muscle mass, muscle function, and muscle strength in hypercatabolic disease states such as cancer cachexia;[7][8][9] consequently, as of June 2016 it is recommended that both the prevention and treatment of sarcopenia and muscle wasting in general include supplementation with HMB, regular resistance exercise, and consumption of a high-protein diet.[7][8] Based upon a meta-analysis of seven randomized controlled trials that was published in 2015, HMB supplementation has efficacy as a treatment for preserving lean muscle mass in older adults.[note 1][6] More research is needed to determine the precise effects of HMB on muscle strength and function in this age group.[6]
Since the absence of muscle-building amino acids can contribute to muscle wasting (that which is torn down must be rebuilt with like material), amino acid therapy may be helpful for regenerating damaged or atrophied muscle tissue. The branched-chain amino acids or BCAAs (leucine, isoleucine, and valine) are critical to this process, in addition to lysine and other amino acids.
In severe cases of muscular atrophy, the use of an anabolic steroid such as methandrostenolone may be administered to patients as a potential treatment. A novel class of drugs, called SARM (selective androgen receptor modulators) are being investigated with promising results. They would have fewer side-effects, while still promoting muscle and bone tissue growth and regeneration. These claims are, however, yet to be confirmed in larger clinical trials.
One important rehabilitation tool for muscle atrophy includes the use of functional electrical stimulation to stimulate the muscles. This has seen a large amount of success in the rehabilitation of paraplegic patients.[10]
Hibernation
Inactivity and starvation in mammals lead to atrophy of skeletal muscle, accompanied by a smaller number and size of the muscle cells as well as lower protein content.[11] In humans, prolonged periods of immobilization, as in the cases of bed rest or astronauts flying in space, are known to result in muscle weakening and atrophy. Such consequences are also noted in small hibernating mammals like the golden-mantled ground squirrels and brown bats.[12]
Bears are an exception to this rule; species in the family Ursidae are famous for their ability to survive unfavorable environmental conditions of low temperatures and limited nutrition availability during winter by means of hibernation. During that time, bears go through a series of physiological, morphological and behavioral changes.[13] Their ability to maintain skeletal muscle number and size at time of disuse is of significant importance.
During hibernation, bears spend four to seven months of inactivity and anorexia without undergoing muscle atrophy and protein loss.[12] There are a few known factors that contribute to the sustaining of muscle tissue. During the summer period, bears take advantage of the nutrition availability and accumulate muscle protein. The protein balance at time of dormancy is also maintained by lower levels of protein breakdown during the winter time.[12] At times of immobility, muscle wasting in bears is also suppressed by a proteolytic inhibitor that is released in circulation.[11] Another factor that contributes to the sustaining of muscle strength in hibernating bears is the occurrence of periodic voluntary contractions and involuntary contractions from shivering during torpor.[14] The three to four daily episodes of muscle activity are responsible for the maintenance of muscle strength and responsiveness in bears during hibernation.[14]
See also
- Brown atrophy of the heart
- Effect of spaceflight on the human body
- Muscle weakness
- Muscular dystrophy
- Myotonic dystrophy
- Sarcopenia
- Journal of Cachexia, Sarcopenia and Muscle
Notes
- ↑ The estimated standard mean difference effect size for the increase in muscle mass in the HMB treatment groups relative to controls was 0.352 kilograms (0.78 lb) with a 95% confidence interval of 0.11–0.594 kilograms (0.24–1.31 lb).[6] The studies included in the meta-analysis had durations of 2–12 months and the majority of studies lasted 2–3 months.[6]
References
- ↑ Seene T (July 1994). "Turnover of skeletal muscle contractile proteins in glucocorticoid myopathy". J. Steroid Biochem. Mol. Biol. 50 (1–2): 1–4. doi:10.1016/0960-0760(94)90165-1. PMID 8049126.
- ↑ Sandri M. 2008. Signaling in Muscle Atrophy and Hypertrophy. Physiology 23: 160-170.
- ↑ Section 1.9.2 (page 76) in: Jacki Bishop; Thomas, Briony (2007). Manual of Dietetic Practice. Wiley-Blackwell. ISBN 1-4051-3525-5.
- ↑ Phillips SM (July 2015). "Nutritional supplements in support of resistance exercise to counter age-related sarcopenia". Adv. Nutr. 6 (4): 452–460. doi:10.3945/an.115.008367. PMC 4496741
 . PMID 26178029.
. PMID 26178029. - ↑ Brioche T, Pagano AF, Py G, Chopard A (April 2016). "Muscle wasting and aging: Experimental models, fatty infiltrations, and prevention". Mol. Aspects Med. doi:10.1016/j.mam.2016.04.006. PMID 27106402.
In conclusion, HMB treatment clearly appears to be a safe potent strategy against sarcopenia, and more generally against muscle wasting, because HMB improves muscle mass, muscle strength, and physical performance. It seems that HMB is able to act on three of the four major mechanisms involved in muscle deconditioning (protein turnover, apoptosis, and the regenerative process), whereas it is hypothesized to strongly affect the fourth (mitochondrial dynamics and functions). Moreover, HMB is cheap (~30– 50 US dollars per month at 3 g per day) and may prevent osteopenia (Bruckbauer and Zemel, 2013; Tatara, 2009; Tatara et al., 2007, 2008, 2012) and decrease cardiovascular risks (Nissen et al., 2000). For all these reasons, HMB should be routinely used in muscle-wasting conditions especially in aged people.
- 1 2 3 4 5 Wu H, Xia Y, Jiang J, Du H, Guo X, Liu X, Li C, Huang G, Niu K (September 2015). "Effect of beta-hydroxy-beta-methylbutyrate supplementation on muscle loss in older adults: a systematic review and meta-analysis". Arch. Gerontol. Geriatr. 61 (2): 168–175. doi:10.1016/j.archger.2015.06.020. PMID 26169182.
RESULTS: A total of seven randomized controlled trials were included, in which 147 older adults received HMB intervention and 140 were assigned to control groups. The meta-analysis showed greater muscle mass gain in the intervention groups compared with the control groups (standard mean difference=0.352kg; 95% confidence interval: 0.11, 0.594; Z value=2.85; P=0.004). There were no significant fat mass changes between intervention and control groups (standard mean difference=-0.08kg; 95% confidence interval: -0.32, 0.159; Z value=0.66; P=0.511).
CONCLUSION: Beta-hydroxy-beta-methylbutyrate supplementation contributed to preservation of muscle mass in older adults. HMB supplementation may be useful in the prevention of muscle atrophy induced by bed rest or other factors. Further studies are needed to determine the precise effects of HMB on muscle strength and physical function in older adults. - 1 2 Brioche T, Pagano AF, Py G, Chopard A (April 2016). "Muscle wasting and aging: Experimental models, fatty infiltrations, and prevention". Mol. Aspects Med. doi:10.1016/j.mam.2016.04.006. PMID 27106402.
In conclusion, HMB treatment clearly appears to be a safe potent strategy against sarcopenia, and more generally against muscle wasting, because HMB improves muscle mass, muscle strength, and physical performance. It seems that HMB is able to act on three of the four major mechanisms involved in muscle deconditioning (protein turnover, apoptosis, and the regenerative process), whereas it is hypothesized to strongly affect the fourth (mitochondrial dynamics and functions). Moreover, HMB is cheap (~30– 50 US dollars per month at 3 g per day) and may prevent osteopenia (Bruckbauer and Zemel, 2013; Tatara, 2009; Tatara et al., 2007, 2008, 2012) and decrease cardiovascular risks (Nissen et al., 2000). For all these reasons, HMB should be routinely used in muscle-wasting conditions especially in aged people. ... 3 g of CaHMB taken three times a day (1 g each time) is the optimal posology, which allows for continual bioavailability of HMB in the body (Wilson et al., 2013).
- 1 2 Argilés JM, Campos N, Lopez-Pedrosa JM, Rueda R, Rodriguez-Mañas L (June 2016). "Skeletal Muscle Regulates Metabolism via Interorgan Crosstalk: Roles in Health and Disease". J. Am. Med. Dir. Assoc. doi:10.1016/j.jamda.2016.04.019. PMID 27324808.
Studies suggest dietary protein and leucine or its metabolite b-hydroxy b-methylbutyrate (HMB) can improve muscle function, in turn improving functional performance. ... These have identified the leucine metabolite β-hydroxy β-methylbutyrate (HMB) as a potent stimulator of protein synthesis as well as an inhibitor of protein breakdown in the extreme case of cachexia.65, 72, 76, 77, 78, 79, 80, 81, 82, 83, 84 A growing body of evidence suggests HMB may help slow, or even reverse, the muscle loss experienced in sarcopenia and improve measures of muscle strength.44, 65, 72, 76, 77, 78, 79, 80, 81, 82, 83, 84 However, dietary leucine does not provide a large amount of HMB: only a small portion, as little as 5%, of catabolized leucine is metabolized into HMB.85 Thus, although dietary leucine itself can lead to a modest stimulation of protein synthesis by producing a small amount of HMB, direct ingestion of HMB more potently affects such signaling, resulting in demonstrable muscle mass accretion.71, 80 Indeed, a vast number of studies have found that supplementation of HMB to the diet may reverse some of the muscle loss seen in sarcopenia and in hypercatabolic disease.65, 72, 83, 86, 87 The overall treatment of muscle atrophy should include dietary supplementation with HMB, although the optimal dosage for each condition is still under investigation.68 ...
Figure 4: Treatments for sarcopenia. It is currently recommended that patients at risk of or suffering from sarcopenia consume a diet high in protein, engage in resistance exercise, and take supplements of the leucine metabolite HMB. - ↑ Mullin GE (February 2014). "Nutrition supplements for athletes: potential application to malnutrition". Nutr. Clin. Pract. 29 (1): 146–147. doi:10.1177/0884533613516130. PMID 24336486.
There are a number of nutrition products on the market that are touted to improve sports performance. HMB appears to be the most promising and to have clinical applications to improve muscle mass and function. Continued research using this nutraceutical to prevent and/or improve malnutrition in the setting of muscle wasting is warranted.
- ↑ D.Zhang et al., Functional Electrical Stimulation in Rehabilitation Engineering: A survey, Nenyang technological University, Singapore
- 1 2 Fuster G, Busquets S, Almendro V, López-Soriano FJ, Argilés JM; Busquets; Almendro; López-Soriano; Argilés (2007). "Antiproteolytic effects of plasma from hibernating bears: a new approach for muscle wasting therapy?". Clin Nutr. 26 (5): 658–61. doi:10.1016/j.clnu.2007.07.003. PMID 17904252.
- 1 2 3 Lohuis TD, Harlow HJ, Beck TD; Harlow; Beck (2007). "Hibernating black bears (Ursus americanus) experience skeletal muscle protein balance during winter anorexia". Comp. Biochem. Physiol. B, Biochem. Mol. Biol. 147 (1): 20–8. doi:10.1016/j.cbpb.2006.12.020. PMID 17307375.
- ↑ Carey HV, Andrews MT, Martin SL; Andrews; Martin (2003). "Mammalian hibernation: cellular and molecular responses to depressed metabolism and low temperature". Physiol. Rev. 83 (4): 1153–81. doi:10.1152/physrev.00008.2003 (inactive 2015-01-09). PMID 14506303.
- 1 2 Harlow, H. J.; Lohuis, T.; Anderson-Sprecher, R. C.; Beck, T. D I. (2004). "Body Surface Temperature Of Hibernating Black Bears May Be Related To Periodic Muscle Activity". Journal of Mammalogy. 85 (3): 414–419. doi:10.1644/1545-1542(2004)085<0414:BSTOHB>2.0.CO;2. ISSN 1545-1542.
{kind=link}
External links
- Muscular atrophy at the US National Library of Medicine Medical Subject Headings (MeSH)