Lumbar spinal stenosis
| Lumbar spinal stenosis | |
|---|---|
 | |
| Lumbar vertebra showing central stenosis and lateral recess stenosis. | |
| Classification and external resources | |
| Specialty | Orthopedics |
| ICD-10 | M48.0 |
| ICD-9-CM | 723.0-724.0 |
| DiseasesDB | 31116 |
| MeSH | D013130 |
Lumbar spinal stenosis (LSS) is a medical condition in which the spinal canal narrows and compresses the spinal cord and nerves at the level of the lumbar vertebra. This is usually due to the common occurrence of spinal degeneration that occurs with aging. It can also sometimes be caused by spinal disc herniation, osteoporosis or a tumor. In the cervical (neck) and lumbar (low back) region it can be a congenital condition to varying degrees.
It is also a common symptom for those who suffer from various skeletal dysplasias such as with pseudoachondroplasia and achondroplasia at an early age.
Spinal stenosis may affect the cervical or thoracic region in which case it is known as cervical spinal stenosis or thoracic spinal stenosis. In some cases, it may be present in all three places in the same patient. Lumbar spinal stenosis results in low back pain as well as pain or abnormal sensations in the legs, thighs, feet or buttocks, or loss of bladder and bowel control.
Signs and symptoms
Understanding the meaning of signs and symptoms for the clinical syndrome of lumbar stenosis requires an understanding of what the syndrome is, and the prevalence of the condition. A recent review on lumbar stenosis in the Journal of the American Medical Association's "Rational Clinical Examination Series"[1] emphasized that the syndrome can be considered when lower extremity pain occurs in combination with back pain. This syndrome occurs in 12% of older community dwelling men[2] and up to 21% of those in retirement communities.[3]
The leg symptoms in lumbar spinal stenosis (LSS) are similar to those found with vascular claudication, giving rise to the term pseudoclaudication.[4] These symptoms include pain, weakness, and tingling of the legs,[4] which may radiate down the leg to the feet.[5] Additional symptoms in the legs may be fatigue, heaviness, weakness, a sensation of tingling, pricking, or numbness and leg cramps, as well as bladder symptoms.[5] Symptoms are most commonly bilateral and symmetrical, but they may be unilateral; leg pain is usually more troubling than back pain.[5]
Pseudoclaudication, now referred to as neurogenic claudication, typically worsen with standing or walking and improve with sitting. The occurrence is often related to posture and lumbar extension. Lying on the side is often more comfortable than lying flat, since it permits greater lumbar flexion. Vascular claudication can resemble spinal stenosis, and some individuals experience unilateral or bilateral symptoms radiating down the legs rather than true claudication.[6]
The first symptoms of stenosis include bouts of low back or neck pain. After a few months or years, this may progress to claudication. The pain may be radicular, following the classic neurologic pathways. This occurs as the spinal nerves or spinal cord become increasingly trapped in a smaller space within the canal. It can be difficult to determine whether pain in the elderly is caused by lack of blood supply or stenosis; testing can usually differentiate between them but patients can have both vascular disease in the legs and spinal stenosis.
Among people with lower extremity pain in combination with back pain, lumbar stenosis as the cause is two times more likely in those older than 70 years of age while those younger than 60 years it is 0.40 as likely. The character of the pain is also useful. When the discomfort does not occur while seated, the likelihood of LSS increases considerably around 7.4 times. Other features increasing the likelihood of lumbar stenosis are improvement in symptoms on bending forward 6.4 times, pain that occurs in both buttocks or legs 6.3 times, and the presence of neurogenic claudication 3.7 times.[1] Alternately, the absence of neurogenic claudication makes lumbar stenosis much less likely as the explanation for the pain.[7]
Causes
Spinal stenosis may be congenital (rarely) or acquired (degenerative), overlapping changes normally seen in the aging spine.[5][6]
Degenerative spondylolisthesis
Forward displacement of a proximal vertebra in relation to its adjacent vertebra in association with an intact neural arch, and in the presence of degenerative changes is known as degenerative spondylolisthesis.[8][9] Degenerative spondylolisthesis narrows the spinal canal and symptoms of spinal stenosis are common. Of these, neural claudication is most common. Any forward slipping of one vertebra on another can cause spinal stenosis by narrowing the canal. If this forward slipping narrows the canal sufficiently, and impinges on the contents of the spinal column, it is spinal stenosis by definition. If there are associated symptoms of narrowing, the diagnosis of spinal stenosis is confirmed. With increasing age, the occurrence of degenerative spondylolisthesis becomes more common. The most common spondylolisthesis occurs with slipping of L4 on L5. Frymoyer showed that spondylolisthesis with canal stenosis is more common in diabetic women who have undergone oophorectomy (removal of ovaries). The cause of symptoms in the legs can be difficult to determine. A peripheral neuropathy secondary to diabetes can have the same symptoms as spinal stenosis.[10]
Ankylosing spondylitis
 Drawing of a lumbar disc herniation which can cause a localized stenosis. Thoracic discs though rare are similar.
Drawing of a lumbar disc herniation which can cause a localized stenosis. Thoracic discs though rare are similar. L5 S1 Spondylolisthesis Grade II with forward slipping of L5 on S1 <50%.
L5 S1 Spondylolisthesis Grade II with forward slipping of L5 on S1 <50%. Lumbar spine showing advanced ankylosing spondylitis which can lead to spinal stenosis.
Lumbar spine showing advanced ankylosing spondylitis which can lead to spinal stenosis.
Diagnosis
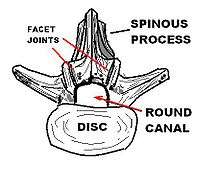
The diagnosis is based on clinical findings.[6] Some patients can have a narrowed canal without symptoms, and do not require therapy. Stenosis can occur as either central stenosis (the narrowing of the entire canal) or foraminal stenosis (the narrowing of the foramen through which the nerve root exits the spinal canal). Severe narrowing of the lateral portion of the canal is called “lateral recess stenosis". The ligamentum flavum (yellow ligament), an important structural component intimately adjacent to the posterior portion of the dural sac (nerve sac) can become thickened and cause stenosis. The articular facets, also in the posterior portion of the bony spine can become thickened and enlarged causing stenosis. These changes are often called “trophic changes” or “facet trophism” in radiology reports. As the canal becomes smaller, resembling a triangular shape, it is called a "trefoil" canal.
The normal lumbar central canal has a midsagittal diameter (front to back) greater than 13 mm., with an area of 1.45 square cm. Relative stenosis is said to exist when the anterior-posterior canal diameter measures between 10 and 13 mm. Absolute stenosis of the lumbar canal exists anatomically when the anterior-posterior measurement is 10 mm. or less.[11][12][13]
Plain x-rays of the lumbar or cervical spine may or may not show spinal stenosis. The definitive diagnosis is established by either CT (computerized tomography) or MRI scanning. Identifying the presence of a narrowed canal makes the diagnosis of spinal stenosis.[14][15][16]
Bicycle test of van Gelderen
In 1977, Dyck and Doyle reported on the bicycle test of van Gelderen.[17] The bicycle test is a simple procedure in which the patient is asked to pedal on a stationary bicycle. If the symptoms are caused by peripheral vascular disease, the patient will experience claudication, a sensation of not getting enough blood to the legs; if the symptoms are caused by lumbar stenosis, symptoms will be relieved when the patient is leaning forward while bicycling. Although diagnostic progress has been made with newer technical advances, the bicycle test remains an inexpensive and easy way to distinguish between claudication caused by vascular disease and spinal stenosis. Dyck and Doyle wrote in their 1977 article:
The authors describe a simple clinical adjunct to the routine neurological examination of patients with intermittent cauda equina compression syndrome. The "bicycle test" helps exclude intermittent claudication due to vascular insufficiency and frequently confirms the relationship of posture to radicular pain.
Magnetic resonance imaging
MRI is the preferred method of diagnosing and evaluating spinal stenosis of all areas of the spine, including cervical, thoracic and lumbar.[18][19] MRI is useful to diagnose cervical spondylotic myelopathy (degenerative arthritis of the cervical spine with associated damage to the spinal cord).[20] The finding of degeneration of the cervical spinal cord on MRI can be ominous; the condition is called myelomalacia or cord degeneration. It is seen as an increased signal on the MRI. In myelopathy (pathology of the spinal cord) from degenerative changes, the findings are usually permanent and decompressive laminectomy will not reverse the pathology. Surgery can stop the progression of the condition. In cases where the MRI changes are due to Vitamin B-12 deficiency, a brighter prospect for recovery can be expected.[21][22][23]
Establishing the diagnosis
The detection of spinal stenosis in the cervical, thoracic or lumbar spine confirms only the anatomic presence of a stenotic condition. This may or may not correlate with the diagnosis of spinal stenosis which is based on clinical findings of radiculopathy, neurogenic claudication, weakness, bowel and bladder dysfunction, spasticity, motor weakness, hyperreflexia and muscular atrophy. These findings, taken from the history and physical examination of the patient (along with the anatomic demonstration of stenosis with an MRI or CT scan), establish the diagnosis.[24]
Management
Nonoperative therapies and laminectomy are the standard treatment for LSS;[25] A trial of conservative treatment is typically recommended.[6] Individuals are generally advised to avoid stressing the lower back, particularly with the spine extended. A physical therapy program to provide core strengthening and aerobic conditioning may be recommended.[6] Overall scientific evidence is inconclusive on whether conservative approach or a surgical treatment is better for lumbar spinal stenosis.[26]
Medication
The evidence for the use of medical interventions for lumbar spinal stenosis is poor.[27] Injectable but not nasal calcitonin may be useful for short term pain relief.[27] Epidural blocks may also transiently decrease pain, but there is no evidence of long-term effect.[27] Adding steroids to these injections does not improve the result;[27][28] the use of epidural steroid injections (ESIs) is controversial and evidence of their efficacy is contradictory.[6]
Non-steroidal anti-inflammatory drugs (NSAIDs), muscle relaxants and opioid analgesics are often used to treat low back pain, but evidence of their efficacy is lacking.[6]
Surgery
Surgery appears to lead to better outcomes if there are ongoing symptoms after three to six months of conservative treatment.[29] Laminectomy is the most effective of the surgical treatments.[25] In those who worsen despite conservative treatments surgery leads to improvement in 60–70% of cases.[6] Another procedure using an interspinous distraction device known as X-STOP was less effective and more expensive when more than one spinal level is repaired.[25] Both surgical procedures are more expensive than medical management.[25]
Another surgical treatment option is an interlaminar implant called coflex®, which is a non-fusion U-shaped device that is placed between two bones in the lower back that maintains motion in the spine and keeps the spine stable after a lumbar decompressive surgery. The U-shaped device maintains height between the bones in the spine so nerves can exit freely and extend to lower extremities.[30]
Prognosis
Most people with mild to moderate symptoms do not get worse.[6] While many improve in the short term after surgery this improvement decreases somewhat with time.[6] A number of factors present before surgery are able to predict the outcome after surgery, with people with depression, cardiovascular disease and scoliosis doing in general worse while those with more severe stenosis beforehand and better overall health doing better.[5]
The natural evolution of disc disease and degeneration leads to stiffening of the intervertebral joint. This leads to osteophyte formation—a bony overgrowth about the joint. This process is called spondylosis, and is part of the normal aging of the spine. This has been seen in studies of normal and diseased spines. Degenerative changes begin to occur without symptoms as early as age 25–30 years. It is not uncommon for people to experience at least one severe case of low back pain by the age of 35 years. This can be expected to improve and become less prevalent as the individual develops osteophyte formation around the discs.[31]
In the US workers' compensation system, once the threshold of two major spinal surgeries is reached, the vast majority of workers will never return to any form of gainful employment. Beyond two spinal surgeries, any more are likely to make the patient worse, not better. Very few studies in the worldwide surgical literature actually document return to work after spinal surgery, or lack thereof.[32]
History
A description of LSS was published by Sachs and Frankel in 1900,[33] but the first clinical description of LSS is usually attributed to the Dutch neurosurgeon Henk Verbiest, whose report appeared in 1954.[5][6][34]
Spinal stenosis began to be recognized as an impairing condition in the 1960s and 1970s. Porter and colleagues discovered that individuals who experience back pain and other symptoms are likely to have smaller spinal canals than those who are asymptomatic.[35] Rothman reported that a normal sized lumbar canal is rarely encountered in persons with either disc disease or those requiring a de-roofing (laminectomy) procedure.[31]
During the 1970s and 1980s, many case reports showed successful surgical treatment rates, but these were based on subjective assessment by surgeons.[6] In 1992, Johnsson, Rosén and Udén described the natural history of LSS, with different conclusions about prognosis and treatment: "70% of patients reported no significant change in symptoms, 15% showed significant improvement, whereas 15% showed some deterioration.[36] The investigators concluded that observation is a reasonable treatment option for lumbar stenosis and that significant neurologic deterioration is rare."[6]
Society and culture
United States
Under rules promulgated by Titles II and XVI of the United States Social Security Act, spinal stenosis is recognized as a disabling condition under Listing 1.04 C. The listing states: "Lumbar spinal stenosis resulting in pseudoclaudication, established by findings on appropriate medically acceptable imaging, manifested by chronic nonradicular pain and weakness, and resulting in inability to ambulate effectively, as defined in 1.00B2b."[37] The regulation is written specifically for lumbar stenosis;[38] inclusion of cervical stenosis requires either a meet or equal depending on the idiosyncrasy of the trier of fact in federal disability hearings.
References
- 1 2 Suri P, Rainville J, Kalichman L, Katz JN (December 2010). "Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis?". JAMA. 304 (23): 2628–36. doi:10.1001/jama.2010.1833. PMC 3260477
 . PMID 21156951.
. PMID 21156951. - ↑ Vogt MT, Cawthon PM, Kang JD, Donaldson WF, Cauley JA, Nevitt MC (June 2006). "Prevalence of symptoms of cervical and lumbar stenosis among participants in the Osteoporotic Fractures in Men Study". Spine. 31 (13): 1445–51. doi:10.1097/01.brs.0000219875.19688.a6. PMID 16741453.
- ↑ Hicks GE, Gaines JM, Shardell M, Simonsick EM (September 2008). "Associations of back and leg pain with health status and functional capacity of older adults: findings from the retirement community back pain study". Arthritis Rheum. 59 (9): 1306–13. doi:10.1002/art.24006. PMID 18759261.
- 1 2 Englund J (January 2007). "Lumbar spinal stenosis". Curr Sports Med Rep. 6 (1): 50–5. doi:10.1007/s11932-007-0012-0. PMID 17212913.
- 1 2 3 4 5 6 Genevay S, Atlas SJ (April 2010). "Lumbar spinal stenosis". Best Pract Res Clin Rheumatol. 24 (2): 253–65. doi:10.1016/j.berh.2009.11.001. PMC 2841052. PMID 20227646.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 Djurasovic M, Glassman SD, Carreon LY, Dimar JR (April 2010). "Contemporary management of symptomatic lumbar spinal stenosis". Orthop. Clin. North Am. 41 (2): 183–91. doi:10.1016/j.ocl.2009.12.003. PMID 20399357.
- ↑ Konno S, Hayashino Y, Fukuhara S, et al. (2007). "Development of a clinical diagnosis support tool to identify patients with lumbar spinal stenosis". Eur Spine J. 16 (11): 1951–1957. doi:10.1007/s00586-007-0402-2. PMC 2223350. PMID 17549525.
- ↑ Takahashi K, Kitahara H, Yamagata M, et al. (November 1990). "Long-term results of anterior interbody fusion for treatment of degenerative spondylolisthesis". Spine. 15 (11): 1211–5. doi:10.1097/00007632-199011010-00022. PMID 2267618.
- ↑ Wiltse LL, Newman PH, Macnab I (June 1976). "Classification of spondylolisis and spondylolisthesis". Clin. Orthop. Relat. Res. (117): 23–9. doi:10.1097/00003086-197606000-00003. PMID 1277669.
- ↑ Frymoyer JW (January 1994). "Degenerative Spondylolisthesis: Diagnosis and Treatment". J Am Acad Orthop Surg. 2 (1): 9–15. PMID 10708989.
- ↑ Ullrich CG, Binet EF, Sanecki MG, Kieffer SA (January 1980). "Quantitative assessment of the lumbar spinal canal by computed tomography". Radiology. 134 (1): 137–43. doi:10.1148/radiology.134.1.7350593. PMID 7350593.
- ↑ Verbiest H (1966). Orthop. Clin. North Am. 6: 177-96
- ↑ Eisenstein S (May 1977). "The morphometry and pathological anatomy of the lumbar spine in South African negroes and caucasoids with specific reference to spinal stenosis". J Bone Joint Surg Br. 59 (2): 173–80. PMID 873978.
- ↑ Lane JM, Gardner MJ, Lin JT, van der Meulen MC, Myers E (October 2003). "The aging spine: new technologies and therapeutics for the osteoporotic spine". Eur Spine J. 12 Suppl 2: S147–54. doi:10.1007/s00586-003-0636-6. PMC 3591818. PMID 14534849.
- ↑ Benoist M (October 2003). "Natural history of the aging spine". Eur Spine J. 12 Suppl 2: S86–9. doi:10.1007/s00586-003-0593-0. PMC 3591827. PMID 12961079.
- ↑ Szpalski M, Gunzburg R (October 2003). "Lumbar spinal stenosis in the elderly: an overview". Eur Spine J. 12 Suppl 2: S170–5. doi:10.1007/s00586-003-0612-1. PMC 3591819. PMID 13680315.
- ↑ Dyck P, Doyle JB (May 1977). ""Bicycle test" of van Gelderen in diagnosis of intermittent cauda equina compression syndrome. Case report". J. Neurosurg. 46 (5): 667–70. doi:10.3171/jns.1977.46.5.0667. PMID 845655.
- ↑ Sheehan NJ (June 2010). "Magnetic resonance imaging for low back pain: indications and limitations". Postgrad Med J. 86 (1016): 374–8. doi:10.1136/ard.2009.110973. PMID 20547606.
- ↑ Cousins JP, Haughton VM (January 2009). "Magnetic resonance imaging of the spine". J Am Acad Orthop Surg. 17 (1): 22–30. PMID 19136424.
- ↑ Tracy JA, Bartleson JD (May 2010). "Cervical spondylotic myelopathy". Neurologist. 16 (3): 176–87. doi:10.1097/NRL.0b013e3181da3a29. PMID 20445427.
- ↑ Kiers L, Desmond P (January 1999). "Magnetic resonance imaging in subacute combined degeneration of the spinal cord". J Clin Neurosci. 6 (1): 49–50. doi:10.1016/S0967-5868(99)90604-5. PMID 18639123.
- ↑ Rimbot A, Juglard R, Stéphant E, et al. (March 2004). "[Subacute combined degeneration of the spinal cord: contribution of MRI]". J Radiol (in French). 85 (3): 326–8. doi:10.1016/S0221-0363(04)97586-5. PMID 15192526.
- ↑ Srikanth SG, Jayakumar PN, Vasudev MK, Taly AB, Chandrashekar HS (September 2002). "MRI in subacute combined degeneration of spinal cord: a case report and review of literature". Neurol India. 50 (3): 310–2. PMID 12391459.
- ↑ "Back Pain | Lower Back Pain | Sciatica | Boulder Neurological Associates". Retrieved 2014-08-27.
- 1 2 3 4 Burnett MG, Stein SC, Bartels RH (July 2010). "Cost-effectiveness of current treatment strategies for lumbar spinal stenosis: nonsurgical care, laminectomy, and X-STOP". J Neurosurg Spine. 13 (1): 39–46. doi:10.3171/2010.3.SPINE09552. PMID 20594016.
- ↑ Zaina, F; Tomkins-Lane, C; Carragee, E; Negrini, S (29 January 2016). "Surgical versus non-surgical treatment for lumbar spinal stenosis.". The Cochrane database of systematic reviews. 1: CD010264. doi:10.1002/14651858.CD010264.pub2. PMID 26824399.
- 1 2 3 4 Tran de QH, Duong S, Finlayson RJ (July 2010). "Lumbar spinal stenosis: a brief review of the nonsurgical management". Can J Anaesth. 57 (7): 694–703. doi:10.1007/s12630-010-9315-3. PMID 20428988.
- ↑ Parr AT, Diwan S, Abdi S (2009). "Lumbar interlaminar epidural injections in managing chronic low back and lower extremity pain: a systematic review". Pain Physician. 12 (1): 163–88. PMID 19165302.
- ↑ Kovacs FM, Urrútia G, Alarcón JD (September 2011). "Surgery versus conservative treatment for symptomatic lumbar spinal stenosis: a systematic review of randomized controlled trials". Spine. 36 (20): E1335–51. doi:10.1097/BRS.0b013e31820c97b1. PMID 21311394.
- ↑ http://www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm327502.htm
- 1 2 Rothman Rh; Semeone FA, eds. (1982). The Spine. Philadelphia: Saunders. p. 518. ISBN 0-7216-7718-5.
- ↑ Waddell G, Kummel EG, Lotto WN, Graham JD, Hall H, McCulloch JA (March 1979). "Failed lumbar disc surgery and repeat surgery following industrial injuries". J Bone Joint Surg Am. 61 (2): 201–7. PMID 422604.
- ↑ Sachs B, Frankel V (1900). "Progressive and kyphotic rigidity of the spine". J Nerv Ment Dis. 27: 1–15. doi:10.1097/00005053-190001000-00001.
- ↑ Verbiest H (May 1954). "A radicular syndrome from developmental narrowing of the lumbar vertebral canal" (PDF). J Bone Joint Surg Br. 36–B (2): 230–7. PMID 13163105.
- ↑ Porter RW, Hibbert CS, Wicks M (November 1978). "The spinal canal in symptomatic lumbar disc lesions". J Bone Joint Surg Br. 60–B (4): 485–7. PMID 711794.
- ↑ Johnsson KE, Rosén I, Udén A (June 1992). "The natural course of lumbar spinal stenosis". Clin. Orthop. Relat. Res. (279): 82–6. PMID 1534726.
- ↑ "Disability programs". US Social Security Administration. September 2008. Retrieved December 26, 2010.
- ↑ "Disability Evaluation Under Social Security" (PDF). US Social Security Administration. January 2003. Retrieved December 26, 2010.
External links
- "Diseases and conditions:Spinal stenosis". The Mayo Clinic. 2008-03-11. Retrieved 2008-11-12.