Horner's syndrome
| Horner's syndrome | |
|---|---|
| Synonyms | Bernard-Horner syndrome, oculosympathetic palsy |
 | |
| Left-sided Horner's syndrome | |
| Classification and external resources | |
| Specialty | neurology |
| ICD-10 | G90.2 |
| ICD-9-CM | 337.9 |
| OMIM | 143000 |
| DiseasesDB | 6014 |
| MedlinePlus | 000708 |
| eMedicine | med/1029 oph/336 |
| Patient UK | Horner's syndrome |
| MeSH | D006732 |
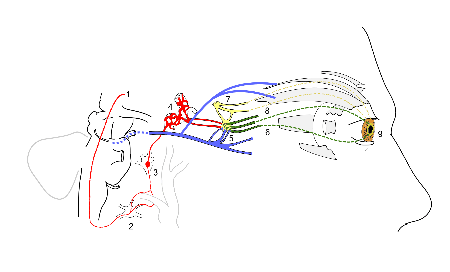
Horner's syndrome is a combination of symptoms that arises when a group of nerves known as the sympathetic trunk is damaged. The signs and symptoms occur on the same side as the lesion of the sympathetic trunk. It is characterized by miosis (a constricted pupil), partial ptosis (a weak, droopy eyelid), apparent anhidrosis (decreased sweating), with or without enophthalmos (inset eyeball).
The nerves of the sympathetic trunk arise from the spinal cord in the chest, and from there ascend to the neck and face. The nerves are part of the sympathetic nervous system, a part of the autonomic (or involuntary) nervous system. Once the syndrome has been recognized, medical imaging and response to particular eye drops may be required to identify the location of the problem and the underlying cause.[1]
Signs and symptoms
Signs that are found in patients on the affected side of the face include
- partial ptosis[1]
- upside-down ptosis (slight elevation of the lower lid)
- anhidrosis
- miosis
- pseudoenophthalmos (the impression that the eye is sunken, caused by a narrow palpebral aperture)
- pupillary dilation lag
- loss of ciliospinal reflex
- bloodshot conjunctiva, depending on the site of lesion.
- unilateral straight hair (in congenital Horner's syndrome); the hair on the affected side may be straight in some cases.
- heterochromia iridum (in congenital Horner's syndrome)
Interruption of sympathetic pathways leads to several implications. It inactivates the dilator muscle and thereby produces miosis. It inactivates the superior tarsal muscle which produces ptosis. It inactivates the orbitalis muscle which produces the effect of enophthalmos. It also reduces sweat secretion in the face.
Sometimes there is flushing on the affected side of the face due to dilation of blood vessels under the skin. The pupil's light reflex is maintained as this is controlled via the parasympathetic nervous system.
In children, Horner's syndrome sometimes leads to heterochromia, a difference in eye color between the two eyes.[1] This happens because a lack of sympathetic stimulation in childhood interferes with melanin pigmentation of the melanocytes in the superficial stroma of the iris.
In veterinary medicine, signs can include partial closure of the third eyelid, or nictitating membrane.
Causes
Horner syndrome is acquired as a result of disease, but may also be congenital (inborn, associated with heterochromatic iris) or iatrogenic (caused by medical treatment). Although most causes are relatively benign, Horner syndrome may reflect serious disease in the neck or chest (such as a Pancoast tumor (tumor in the apex of the lung) or thyrocervical venous dilatation).
Causes can be divided according to the presence and location of anhidrosis:
- Central (anhidrosis of face, arm and trunk)
- Preganglionic (anhidrosis of face)
- Cervical rib traction on stellate ganglion
- Thyroid carcinoma
- Thyroidectomy
- Goiter
- Bronchogenic carcinoma of the superior fissure (Pancoast tumor) on apex of lung
- Klumpke paralysis
- Trauma - base of neck, usually blunt trauma, sometimes surgery.
- As a complication of tube thoracostomy
- Thoracic aortic aneurysm
- Postganglionic (no anhidrosis)
- Cluster headache - combination termed Horton's headache
- An episode of Horner's syndrome may occur during a migraine attack and be relieved afterwards[2]
- Carotid artery dissection/carotid artery aneurysm
- Cavernous sinus thrombosis
- Middle ear infection
- Sympathectomy
- Nerve blocks, such as cervical plexus block, stellate ganglion or interscalene block
Pathophysiology
Horner syndrome is due to a deficiency of sympathetic activity. The site of lesion to the sympathetic outflow is on the ipsilateral side of the symptoms. The following are examples of conditions that cause the clinical appearance of Horner's syndrome:
- First-order neuron disorder: Central lesions that involve the hypothalamospinal tract (e.g. transection of the cervical spinal cord).
- Second-order neuron disorder: Preganglionic lesions (e.g. compression of the sympathetic chain by a lung tumor) that releases acetylcholine.
- Third-order neuron disorder: Postganglionic lesions at the level of the internal carotid artery (e.g. a tumor in the cavernous sinus or a carotid artery dissection) that releases norepinephrine.
- Partial Horner's syndrome: In case of a third-neuron disorder, anhidrosis is limited to the middle part of the forehead or can be absent, resulting in a partial Horner's syndrome.[3]
If someone has impaired sweating above the waist affecting only one side of the body, yet they do not have a clinically apparent Horner's syndrome, then the lesion is just below the stellate ganglion in the sympathetic chain.
Diagnosis

Three tests are useful in confirming the presence and severity of Horner syndrome:
- Cocaine drop test: Cocaine eyedrops block the reuptake of post-ganglionic norepinephrine resulting in the dilation of a normal pupil from retention of norepinephrine in the synapse. However, in Horner's syndrome the lack of norepinephrine in the synaptic cleft causes mydriatic failure. A more recently introduced approach that is more dependable and obviates the difficulties in obtaining cocaine is to apply the alpha-agonist apraclonidine to both eyes and observe the increased mydriatic effect (due to hypersensitivity) on the affected side of Horner syndrome (the opposite effect to what the cocaine test would produce in the presence of Horner's).
- Paredrine test: This test helps to localize the cause of the miosis. If the third order neuron (the last of three neurons in the pathway which ultimately discharges norepinephrine into the synaptic cleft) is intact, then the amphetamine causes neurotransmitter vesicle release, thus releasing norepinephrine into the synaptic cleft and resulting in robust mydriasis of the affected pupil. If the lesion itself is of the third order neuron, then the amphetamine will have no effect and the pupil remains constricted. There is no pharmacological test to differentiate between a first and second order neuron lesion.[3]
- Dilation lag test
It is important to distinguish the ptosis caused by Horner's syndrome from the ptosis caused by a lesion to the oculomotor nerve. In the former, the ptosis occurs with a constricted pupil (due to a loss of sympathetics to the eye), whereas in the latter, the ptosis occurs with a dilated pupil (due to a loss of innervation to the sphincter pupillae). In a clinical setting, these two ptoses are fairly easy to distinguish. In addition to the blown pupil in a CNIII (oculomotor nerve) lesion, this ptosis is much more severe, occasionally occluding the whole eye. The ptosis of Horner syndrome can be quite mild or barely noticeable (partial ptosis).
When anisocoria occurs and the examiner is unsure whether the abnormal pupil is the constricted or dilated one, if a one-sided ptosis is present then the abnormally sized pupil can be presumed to be on the side of the ptosis.
In children
The most common causes in young children are birth trauma and a type of cancer called neuroblastoma.[4] The cause of about a third of cases in children is unknown.[4]
History
It is named after Johann Friedrich Horner, the Swiss ophthalmologist who first described the syndrome in 1869.[5][6] Several others had previously described cases, but "Horner's syndrome" is most prevalent. In France and Italy, Claude Bernard is also eponymized with the condition ("Claude Bernard-Horner syndrome").
See also
References
- 1 2 3 Ropper AH, Brown RH (2005). "14: disorders of ocular movement and pupillary function". In Ropper AH, Brown RH. Adams and Victor's Principles of Neurology (8th ed.). New York: McGraw-Hill Professional. pp. 222–45. doi:10.1036/0071469710. ISBN 0-07-141620-X.
- ↑ Laing, C; Thomas, DJ; Mathias, CJ; Unwin, RJ (2000). "Headache, hypertension and Horner's syndrome". Journal of the Royal Society of Medicine. 93 (10): 535–536. PMC 1298129
 . PMID 11064693..
. PMID 11064693.. - 1 2 Lee JH, Lee HK, Lee DH, Choi CG, Kim SJ, Suh DC (2007). "Neuroimaging strategies for three types of Horner syndrome with emphasis on anatomic location". AJR Am J Roentgenol. 188 (1): W74–81. doi:10.2214/AJR.05.1588. PMID 17179330.
- 1 2 Kennard, Christopher; Leigh, R. John (2011-06-28). Neuro-ophthalmology: Handbook of Clinical Neurology (Series Editors: Aminoff, Boller and Swaab). Elsevier. p. 452. ISBN 9780702045479.
- ↑ Horner JF (1869). "Über eine Form von Ptosis". Klin Monatsbl Augenheilk. 7: 193–8.
- ↑ synd/1056 at Who Named It?