Frank–Starling law
The Frank–Starling law of the heart (also known as Starling's law or the Frank–Starling mechanism or Maestrini heart's law) states that the stroke volume of the heart increases in response to an increase in the volume of blood filling the heart (the end diastolic volume) when all other factors remain constant. In other words, as a larger volume of blood flows into the ventricle, the blood will stretch the walls of the heart, causing a greater expansion during diastole, which in turn increases the force of the contraction and thus the quantity of blood that is pumped into the aorta during systole. The increased volume of blood stretches the ventricular wall, causing cardiac muscle to contract more forcefully (the so-called Frank–Starling mechanisms). The stroke volume may also increase as a result of greater contractility of the cardiac muscle during exercise, independent of the end-diastolic volume. The Frank–Starling mechanism appears to make its greatest contribution to increasing stroke volume at lower work rates, and contractility has its greatest influence at higher work rates.
This allows the cardiac output to be synchronized with the venous return, arterial blood supply and humoral length[1] without depending upon external regulation to make alterations.
Physiology
As the heart fills with more blood than usual, the force of cardiac muscular contractions increases.[2] This is a result of an increase in the load experienced by each muscle fiber due to the extra blood load entering the heart. The stretching of the muscle fibers augments cardiac muscle contraction by increasing the calcium sensitivity of the myofibrils,[3] causing a greater number of actin-myosin cross-bridges to form within the muscle fibers. The force that any single cardiac muscle fiber generates is proportional to the initial sarcomere length (known as preload), and the stretch on the individual fibers is related to the end-diastolic volume of the left and right ventricles.
In the human heart, maximal force is generated with an initial sarcomere length of 2.2 micrometers, a length which is rarely exceeded in the normal heart. Initial lengths larger or smaller than this optimal value will decrease the force the muscle can achieve. For larger sarcomere lengths, this is the result of less overlap of the thin and thick filaments; for smaller sarcomere lengths, the cause is the decreased sensitivity for calcium by the myofilaments.
Clinical examples
Shifting along the line
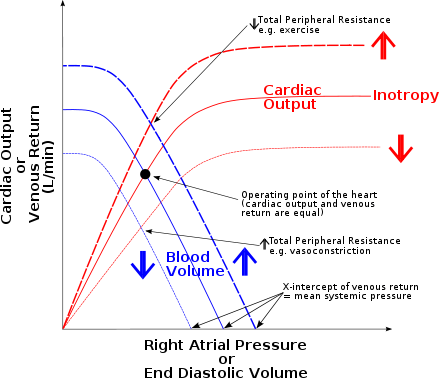
- A blood volume increase would cause a shift along the line to the right, which increases left ventricular end diastolic volume (x axis), and therefore also increases stroke volume (y axis) (because the line curves upwards).
This can be seen most dramatically in the case of premature ventricular contraction. The premature ventricular contraction causes early emptying of the left ventricle (LV) into the aorta. Since the next ventricular contraction will come at its regular time, the filling time for the LV increases, causing an increased LV end-diastolic volume. Because of the Frank–Starling law, the next ventricular contraction will be more forceful, causing the ejection of the larger than normal volume of blood, and bringing the LV end-systolic volume back to baseline.
For example, during vasoconstriction the end diastolic volume (EDV) will increase due to an increase in TPR (total peripheral resistance) (increased TPR causes a decrease in the stroke volume which means that more blood will be left in the ventricle upon contraction – an increased end systolic volume (ESV). ESV + normal venous return will increase the end diastolic volume). Increased EDV causes the stretching of the ventricular myocardial cells which in turn use more force when contracting. Cardiac output will then increase according to the Frank–Starling graph. (The above is true of healthy myocardium. In the failing heart, the more the myocardium is dilated, the weaker it can pump, as it then reverts to Laplace's law.) The S3, or third heart sound can be heard due to this increase in volume which can be pathognomic for heart failure.
- By contrast, pericardial effusion would result in a shift along the line to the left, decreasing stroke volume.
History
The law was named after the two physiologists, Otto Frank and Ernest Starling, who first described it.
Long before the development of the sliding filament hypothesis and our understanding that active tension depends on the maximum load on a single cardiac sarcomere or Cardiomyocyte, Ernest Starling hypothesized in 1918 that "the mechanical energy set free in the passage from the resting to the active state is a function of the length of the fiber." We now have a technological glimpse of the powerful mechanical/molecular basis of the sliding filament theory perhaps unforeseen by Frank or Starling. We still lack a working mathematical construct that proves a link between sliding filament theory and Frank–Starling. Initial length of myocardial fibers determines the initial work done during the cardiac cycle.
Indeed, the first formulation of the law was theorized by the Italian physiologist Dario Maestrini, who on December 13, 1914, started the first of 19 experiments that led him to formulate the "legge del cuore" .[4][5][6][7][8][9][10][11][12][13][14][15][16]
Professor Ernest Henry Starling,[17] (most famous at the time), was the holder of the Physiology chair at London University and traced Maestrini theories in 1918. Despite the sudden death of Starling, whose great fame was the driving motive of the proposed award of the Nobel Prize, Maestrini never received due recognition, and today the "law of the heart" is known worldwide as "Starling's Law," though, among the Italian doctors, it is known by the nickname "Legge di Maestrini".[18][19][20][21][22]
In 1974 an editorial comment in The Lancet briefly mentioned that "Starling’s law [of the heart] was no complete novelty, and, like many others, he built on the work of notable predecessors".[23]
See also
References
- ↑ Costanzo, Linda S. (2007). Physiology. Hagerstwon, MD: Lippincott Williams & Wilkins. p. 81. ISBN 0-7817-7311-3.
- ↑ "Cardiac Basic Physiology". Retrieved 2009-01-07.
- ↑ Klabunde, Richard E. "Cardiovascular Physiology Concepts". Lippincott Williams & Wilkins, 2011, p. 74.
- ↑ Spadolini, Igino (1946). UTET, eds. Trattato di Fisiologia,. 2. Torino.
- ↑ Berne, Robert M. (2004). Ambrosiana, eds. Fisiologia. Milano.
- ↑ "www.ancecardio.it" (PDF) (in Italian). pp. 29–31. Retrieved 6 August 2010.
- ↑ MAESTRINI, D. (February 1951). "[Genesis of the so-called insufficient contractions of the heart in decompensation.]". Policlinico Prat. 58 (9): 257–68. PMID 14833944.
- ↑ MAESTRINI, D. (July 1951). "[The importance of the altered organic exchange (fatigue), of the structure and colloidal state of the fiber, for the genesis of the so-called small, insufficient contractions of the heart in failure.]". Policlinico Prat. 58 (30): 933–45. PMID 14864102.
- ↑ MAESTRINI, D. (November 1951). "[The law of the heart in biology and clinical medicine.]". Minerva Med. 42 (80): 857–64. PMID 14919226.
- ↑ MAESTRINI, D. (June 1952). "[A new theory of cardiac decompensation.]". Policlinico Prat. 59 (24): 797–814. PMID 14957592.
- ↑ MAESTRINI, D. "[Not Available.]". Gazz Sanit. 18 (5): 162–4. PMID 18859625.
- ↑ PENNACCHIO, L.; D. MAESTRINI (September 1952). "[Comment on a new theory of cardiac insufficiency.]". Policlinico Prat. 59 (37): 1223–4. PMID 13026471.
- ↑ MAESTRINI, D. (January 1958). "[The law of the heart from its discovery to the present time.]". Minerva Med. 49 (3-4): Varia, 28–36. PMID 13516733.
- ↑ MAESTRINI, D. (December 1958). "[Variations of cardiac volume dynamics in clinical practice, examined in the light of the law of the heart.]". Minerva Cardioangiol. 6 (12): 657–67. PMID 13643787.
- ↑ MAESTRINI, D. (February 1959). "[S. Baglioni and the law of the heart.]". Policlinico Prat. 66 (7): 224–30. PMID 13645276.
- ↑ MAESTRINI, D. (October 1959). "[On cardiac dynamics in the phase preceding right hypertrophy and on its electrocardiographic aspect in man.]". Policlinico Prat. 66: 1409–13. PMID 13853750.
- ↑ Katz, AM.; EH. Starling (December 2002). "Ernest Henry Starling, his predecessors, and the "Law of the Heart".". Circulation. 106 (23): 2986–92. doi:10.1161/01.CIR.0000040594.96123.55. PMID 12460884.
- ↑ Dario, Maestrini, ed. (1925), "La legge del cuore in clinica", Comunicazione Soc. Med. Chirur. Osp. Abruzzesi, seduta del 30 Agosto 1925, Cuore e Circolazione, p. 506
- ↑ "Maestrini biografie" (PDF). Retrieved 6 August 2010.
- ↑ Maestrini, Dario (1967). Roma, Luigi Pozzi editore, eds. Nuove vedute e nuove realtà in Cardiologia 1911-1967. Roma. p. 279.
- ↑ Italo Farnetani Italo, Farnetani; Farnetani, Francesca (2002). "È ad Arezzo il giallo della "Legge di Maestrini-Starling,". Il Cisalpino. 3: 57–62.
- ↑ Massimo Pandolfi,; Francesco De Tommasi. ANALECTA HISTORICO MEDICA, ed. "www.profpaolovanni.it" (PDF). pp. 185–187. Retrieved 6 August 2010.
- ↑ "Editorial: Starling's law survives.". Lancet. 304 (7884): 818. October 1974. doi:10.1016/S0140-6736(74)91080-0. PMID 4138723.
External links
- 1355808810 at GPnotebook
- "New Concepts in the Control of Muscle Contraction" by Gerry A Smith PhD (Cantab)