Epidemiology of autism
The epidemiology of autism is the study of factors affecting autism spectrum disorders (ASD). A 2012 review of global prevalence estimates of autism spectrum disorders found a median of 62 cases per 10,000 people.[1] There is a lack of evidence from low- and middle-income countries though.[1]
ASD averages a 4.3:1 male-to-female ratio.[2] The number of children known to have autism has increased dramatically since the 1980s, at least partly due to changes in diagnostic practice; it is unclear whether prevalence has actually increased;[2] and as-yet-unidentified environmental risk factors cannot be ruled out.[3] The risk of autism is associated with several prenatal factors, including advanced paternal age and diabetes in the mother during pregnancy.[4] ASD is associated with several genetic disorders[5] and with epilepsy.[6]
Autism is a complex neurodevelopmental disorder. Many causes have been proposed, but its theory of causation is still questionable and ultimately unknown.[2][7] Autism is believed to be largely inherited, although the genetics of autism are complex and it is unclear which genes are responsible.[8] Little evidence exists to support associations with specific environmental exposures.[2]
In rare cases, autism is strongly associated with agents that cause birth defects.[9] Other proposed causes, such as childhood vaccines, are controversial and the vaccine hypotheses lack any convincing scientific evidence.[3] Andrew Wakefield published a small study in 1998 in the United Kingdom suggesting a causal link between autism and the trivalent MMR vaccine. After data included in the report was shown to be deliberately falsified, the paper was retracted, and Wakefield's medical license revoked.[10][11]
Frequency
Although incidence rates measure autism risk directly, most epidemiological studies report other frequency measures, typically point or period prevalence, or sometimes cumulative incidence. Attention is focused mostly on whether prevalence is increasing with time.[2]
Incidence and prevalence
Epidemiology defines several measures of the frequency of occurrence of a disease or condition:[12]
- The incidence rate of a condition is the rate at which new cases occurred per person-year, for example, "2 new cases per 1,000 person-years".
- The cumulative incidence is the proportion of a population that became new cases within a specified time period, for example, "1.5 per 1,000 people became new cases during 2006".
- The point prevalence of a condition is the proportion of a population that had the condition at a single point in time, for example, "10 cases per 1,000 people at the start of 2006".
- The period prevalence is the proportion that had the condition at any time within a stated period, for example, "15 per 1,000 people had cases during 2006".
When studying how diseases are caused, incidence rates are the most appropriate measure of disease frequency as they assess risk directly. However, incidence can be difficult to measure with rarer chronic diseases such as autism.[12] In autism epidemiology, point or period prevalence is more useful than incidence, as the disorder starts long before it is diagnosed, and the gap between initiation and diagnosis is influenced by many factors unrelated to risk. Research focuses mostly on whether point or period prevalence is increasing with time; cumulative incidence is sometimes used in studies of birth cohorts.[2]
Estimation methods
The three basic approaches used to estimate prevalence differ in cost and in quality of results. The simplest and cheapest method is to count known autism cases from sources such as schools and clinics, and divide by the population. This approach is likely to underestimate prevalence because it does not count children who have not been diagnosed yet, and it is likely to generate skewed statistics because some children have better access to treatment.[13]
The second method improves on the first by having investigators examine student or patient records looking for probable cases, to catch cases that have not been identified yet. The third method, which is arguably the best, screens a large sample of an entire community to identify possible cases, and then evaluates each possible case in more detail with standard diagnostic procedures. This last method typically produces the most reliable, and the highest, prevalence estimates.[13]
Frequency estimates
Estimates of the prevalence of autism vary widely depending on diagnostic criteria, age of children screened, and geographical location.[14] Most recent reviews tend to estimate a prevalence of 1–2 per 1,000 for autism and close to 6 per 1,000 for ASD;[2] PDD-NOS is the vast majority of ASD, Asperger syndrome is about 0.3 per 1,000 and the atypical forms childhood disintegrative disorder and Rett syndrome are much rarer.[15]
A 2006 study of nearly 57,000 British nine- and ten-year-olds reported a prevalence of 3.89 per 1,000 for autism and 11.61 per 1,000 for ASD; these higher figures could be associated with broadening diagnostic criteria.[16] Studies based on more-detailed information, such as direct observation rather than examination of medical records, identify higher prevalence; this suggests that published figures may underestimate ASD's true prevalence.[17] A 2009 study of the children in Cambridgeshire, England used different methods to measure prevalence, and estimated that 40% of ASD cases go undiagnosed, with the two least-biased estimates of true prevalence being 11.3 and 15.7 per 1,000.[18]
A 2009 U.S. study based on 2006 data estimated the prevalence of ASD in 8-year-old children to be 9.0 per 1,000 (approximate range 8.6–9.3).[19] A 2009 report based on the 2007 Adult Psychiatric Morbidity Survey by the National Health Service determined that the prevalence of ASD in adults was approximately 1% of the population, with a higher prevalence in males and no significant variation between age groups;[20] these results suggest that prevalence of ASD among adults is similar to that in children and rates of autism are not increasing.[21]
Changes with time
Attention has been focused on whether the prevalence of autism is increasing with time. Earlier prevalence estimates were lower, centering at about 0.5 per 1,000 for autism during the 1960s and 1970s and about 1 per 1,000 in the 1980s, as opposed to today's 1–2 per 1,000.[2]
The number of reported cases of autism increased dramatically in the 1990s and early 2000s, prompting investigations into several potential reasons:[23]
- More children may have autism; that is, the true frequency of autism may have increased.
- There may be more complete pickup of autism (case finding), as a result of increased awareness and funding. For example, attempts to sue vaccine companies may have increased case-reporting.
- The diagnosis may be applied more broadly than before, as a result of the changing definition of the disorder, particularly changes in DSM-III-R and DSM-IV.
- An editorial error in the description of the PDD-NOS category of Autism Spectrum Disorders in the DSM-IV, in 1994, inappropriately broadened the PDD-NOS construct. The error was corrected in the DSM-IV-TR, in 2000, reversing the PDD-NOS construct back to the more restrictive diagnostic criteria requirements from the DSM-III-R.[24]
- Successively earlier diagnosis in each succeeding cohort of children, including recognition in nursery (preschool), may have affected apparent prevalence but not incidence.
- A review of the "rising autism" figures compared to other disabilities in schools shows a corresponding drop in findings of mental retardation.[25]
The reported increase is largely attributable to changes in diagnostic practices, referral patterns, availability of services, age at diagnosis, and public awareness.[2][3][22] A widely cited 2002 pilot study concluded that the observed increase in autism in California cannot be explained by changes in diagnostic criteria,[26] but a 2006 analysis found that special education data poorly measured prevalence because so many cases were undiagnosed, and that the 1994–2003 U.S. increase was associated with declines in other diagnostic categories, indicating that diagnostic substitution had occurred.[27]
A 2007 study that modeled autism incidence found that broadened diagnostic criteria, diagnosis at a younger age, and improved efficiency of case ascertainment, can produce an increase in the frequency of autism ranging up to 29-fold depending on the frequency measure, suggesting that methodological factors may explain the observed increases in autism over time.[28] A small 2008 study found that a significant number (40%) of people diagnosed with pragmatic language impairment as children in previous decades would now be given a diagnosis as autism.[29] A study of all Danish children born in 1994–99 found that children born later were more likely to be diagnosed at a younger age, supporting the argument that apparent increases in autism prevalence were at least partly due to decreases in the age of diagnosis.[30]
A 2009 study of California data found that the reported incidence of autism rose 7- to 8-fold from the early 1990s to 2007, and that changes in diagnostic criteria, inclusion of milder cases, and earlier age of diagnosis probably explain only a 4.25-fold increase; the study did not quantify the effects of wider awareness of autism, increased funding, and expanding treatment options resulting in parents' greater motivation to seek services.[31] Another 2009 California study found that the reported increases are unlikely to be explained by changes in how qualifying condition codes for autism were recorded.[32]
Several environmental risk factors have been proposed to support the hypothesis that the actual frequency of autism has increased. These include certain foods, infectious disease, pesticides, MMR vaccine, and vaccines containing the preservative thiomersal, formerly used in several childhood vaccines in the U.S.[2] Although there is overwhelming scientific evidence against the MMR hypothesis and no convincing evidence for the thiomersal hypothesis, other as-yet-unidentified environmental risk factors cannot be ruled out.[3] Although it is unknown whether autism's frequency has increased, any such increase would suggest directing more attention and funding toward changing environmental factors instead of continuing to focus on genetics.[33]
Geographical frequency
Africa
The prevalence of autism in Africa is unknown.[34]
Americas
Canada
The rate of autism diagnoses in Canada was 1 in 450 in 2003. However, preliminary results of an epidemiological study conducted at Montreal Children's Hospital in the 2003-2004 school year found a prevalence rate of 0.68% (or 1 per 147).[35]
A 2001 review of the medical research conducted by the Public Health Agency of Canada concluded that there was no link between MMR vaccine and either inflammatory bowel disease or autism.[36] The review noted, "An increase in cases of autism was noted by year of birth from 1979 to 1992; however, no incremental increase in cases was observed after the introduction of MMR vaccination." [36] After the introduction of MMR, "A time trend analysis found no correlation between prevalence of MMR vaccination and the incidence of autism in each birth cohort from 1988 to 1993."[36]
United States
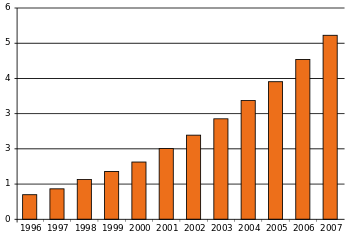
CDC's most recent estimate is that 1 out of every 68 children, or 14.7 per 1,000, have some form of ASD as of 2010.[37] The number of diagnosed cases of autism grew dramatically in the U.S. in the 1990s and early 2000s. For the 2006 surveillance year, identified ASD cases were an estimated 9.0 per 1000 children aged 8 years (95% confidence interval [CI] = 8.6–9.3).[19] These numbers measure what is sometimes called "administrative prevalence", that is, the number of known cases per unit of population, as opposed to the true number of cases.[27] This prevalence estimate rose 57% (95% CI 27%–95%) from 2002 to 2006.[19]
The number of new cases of austism spectrum disorder (ASD) in Caucasian boys is roughly 50% higher than found in Hispanic children, and approximately 30% more likely to occur than in Non-Hispanic white children in the United States.[2][38]
A further study in 2006 concluded that the apparent rise in administrative prevalence was the result of diagnostic substitution, mostly for findings of mental retardation and learning disabilities.[27] "Many of the children now being counted in the autism category would probably have been counted in the mental retardation or learning disabilities categories if they were being labelled 10 years ago instead of today," said researcher Paul Shattuck of the Waisman Center at the University of Wisconsin–Madison, in a statement.[39]
A population-based study in Olmsted County, Minnesota county found that the cumulative incidence of autism grew eightfold from the 1980–83 period to the 1995–97 period. The increase occurred after the introduction of broader, more-precise diagnostic criteria, increased service availability, and increased awareness of autism.[40] During the same period, the reported number of autism cases grew 22-fold in the same location, suggesting that counts reported by clinics or schools provide misleading estimates of the true incidence of autism.[41]
Venezuela
A 2008 study in Venezuela reported a prevalence of 1.1 per 1000 for autism and 1.7 per 1000 for ASD.[42]
Asia
A journal reports that the median prevalence of ASD among 2–6-year-old children who are reported in China from 2000 upwards was 10.3/10,000.[43]
Hong Kong
A 2008 Hong Kong study reported an ASD incidence rate similar to those reported in Australia and North America, and lower than Europeans. It also reported a prevalence of 1.68 per 1,000 for children under 15 years.[44]
Japan
A 2005 study of a part of Yokohama with a stable population of about 300,000 reported a cumulative incidence to age 7 years of 48 cases of ASD per 10,000 children in 1989, and 86 in 1990. After the vaccination rate of the triple MMR vaccine dropped to near zero and was replaced with three single vaccines, the incidence rate grew to 97 and 161 cases per 10,000 children born in 1993 and 1994, respectively, indicating that the combined MMR vaccine did not cause autism.[45] A 2004 Japanese autism association reported that about 360.000 people have typical kanner type autism.
Middle East
Israel
A 2009 study reported that the annual incidence rate of Israeli children with a diagnosis of ASD receiving disability benefits rose from zero in 1982–1984 to 190 per million in 2004. It was not known whether these figures reflected true increases or other factors such as changes in diagnostic measures.[46]
Saudi Arabia
Studies of autism frequency have been particularly rare in the Middle East. One rough estimate is that the prevalence of autism in Saudi Arabia is 18 per 10,000, slightly higher than the 13 per 10,000 reported in developed countries. Estimates for ASD prevalence in Saudi Arabia are not available.[47]
Europe
Denmark
A 2003 study reported that the cumulative incidence of autism in Denmark was stable until 1990. In 1992, thimerosal-containing vaccines were removed in Denmark. The incidence of autism increased after the removal of thimerosal-containing vaccines, during the interval from 1991 until 2000. For example, for children aged 2–4 years, the cumulative incidence was about 0.5 new cases per 10,000 children in 1990 and about 4.5 new cases per 10,000 children in 2000. The study concluded that "ecological data do not support a correlation between thimerosal-containing vaccines and the incidence of autism".[48]
France
France made autism the national focus for the year 2012 and the Health Ministry now evaluates the rate of autism to be 67 per 10000 (1 out of 150).[49]
Eric Fombonne made some studies in the years 1992 and 1997. He found a prevalence of 16 per 10.000 for the global pervasive developmental disorder (PDD).[50][51] The INSERM found a prevalence of 27 per 10,000 for the ASD and a prevalence of 9 per 10,000 for the early infantile autism in 2003.[52] Those figures are considered as underrated as the WHO gives figures between 30 and 60 per 10,000.[53] The French Minister of Health gives a prevalence of 4.9 per 10,000 on its website but it counts only early infantile autism.[54]
Germany
A 2008 study in Germany found that inpatient admission rates for children with ASD increased 30% from 2000 to 2005, with the largest rise between 2000 and 2001 and a decline between 2001 and 2003. Inpatient rates for all mental disorders also rose for ages up to 15 years, so that the ratio of ASD to all admissions rose from 1.3% to 1.4%.[55]
Norway
A 2009 study in Norway reported prevalence rates for ASD ranging from 0.21% to 0.87%, depending on assessment method and assumptions about non-response, suggesting that methodological factors explain large variances in prevalence rates in different studies.[56]
United Kingdom
The incidence and changes in incidence with time are unclear in the United Kingdom.[57] The reported autism incidence in the UK rose starting before the first introduction of the MMR vaccine in 1989.[58] However, a perceived link between the two arising from the results of a fraudulent scientific study, has caused considerable controversy, despite being subsequently disproved.[59] A 2004 study found that the reported incidence of pervasive developmental disorders in a general practice research database in England and Wales grew steadily during 1988–2001 from 0.11 to 2.98 per 10,000 person-years, and concluded that much of this increase may be due to changes in diagnostic practice.[60]
Genetics
As late as the mid-1970s there was little evidence of a genetic role in autism; evidence from genetic epidemiology studies now suggests that it is one of the most heritable of all psychiatric conditions.[61] The first studies of twins estimated heritability to be more than 90%; in other words, that genetics explains more than 90% of autism cases.[8] When only one identical twin is autistic, the other often has learning or social disabilities. For adult siblings, the risk of having one or more features of the broader autism phenotype might be as high as 30%,[62] much higher than the risk in controls.[63] About 10–15% of autism cases have an identifiable Mendelian (single-gene) condition, chromosome abnormality, or other genetic syndrome,[62] and ASD is associated with several genetic disorders.[5]
Since heritability is less than 100% and symptoms vary markedly among identical twins with autism, environmental factors are most likely a significant cause as well. If some of the risk is due to gene-environment interaction the 90% heritability estimate may be too high;[2] new twin data and models with structural genetic variation are needed.[64]
Genetic linkage analysis has been inconclusive; many association analyses have had inadequate power.[64] Studies have examined more than 100 candidate genes; many genes must be examined because more than a third of genes are expressed in the brain and there are few clues on which are relevant to autism.[2]
Risk factors
Boys are at higher risk for autism than girls. The ASD sex ratio averages 4.3:1 and is greatly modified by cognitive impairment: it may be close to 2:1 with mental retardation and more than 5.5:1 without. Recent studies have found no association with socioeconomic status, and have reported inconsistent results about associations with race or ethnicity.[2]
Autism is associated with several prenatal risk factors, including advanced age in either parent, diabetes, bleeding and use of psychiatric drugs in the mother during pregnancy.[4] Autism was found to be indirectly linked to prepregnancy obesity and low weight mothers.[65] It is not known whether mutations that arise spontaneously in autism and other neuropsychiatric disorders come mainly from the mother or the father, or whether the mutations are associated with parental age.[66] However, recent studies have identified advancing paternal age as a significant risk factor for ASD.[67] Increased risk of autism has also been linked to rapid "catch-up" growth for children born to mothers who had unhealthy weight at conception.[65]
A large 2008 population study of Swedish parents of children with autism found that the parents were more likely to have been hospitalized for a mental disorder, that schizophrenia was more common among the mothers and fathers, and that depression and personality disorders were more common among the mothers.[68]
It is not known how many siblings of autistic individuals are themselves autistic. Several studies based on clinical samples have given quite different estimates, and these clinical samples differ in important ways from samples taken from the general community.[69]
Autism has also been shown to cluster in urban neighborhoods of high socioeconomic status. One study from California found a three to fourfold increased risk of autism in a small 30 by 40 km region centered on West Hollywood, Los Angeles.[70]
Comorbid conditions
Autism is associated with several other conditions:
- Genetic disorders. About 10–15% of autism cases have an identifiable Mendelian (single-gene) condition, chromosome abnormality, or other genetic syndrome,[62] and ASD is associated with several genetic disorders.[5]
- Intellectual disability. The fraction of autistic individuals who also meet criteria for intellectual disability has been reported as anywhere from 25% to 70%, a wide variation illustrating the difficulty of assessing autistic intelligence.[71]
- Anxiety disorders are common among children with ASD, although there are no firm data.[72] Symptoms include generalized anxiety and separation anxiety,[73] and are likely affected by age, level of cognitive functioning, degree of social impairment, and ASD-specific difficulties. Many anxiety disorders, such as social phobia, are not commonly diagnosed in people with ASD because such symptoms are better explained by ASD itself, and it is often difficult to tell whether symptoms such as compulsive checking are part of ASD or a co-occurring anxiety problem. The prevalence of anxiety disorders in children with ASD has been reported to be anywhere between 11% and 84%.[72]
- Epilepsy, with variations in risk of epilepsy due to age, cognitive level, and type of language disorder; 5–38% of children with autism have comorbid epilepsy, and only 16% of these have remission in adulthood.[6]
- Several metabolic defects, such as phenylketonuria, are associated with autistic symptoms.[74]
- Minor physical anomalies are significantly increased in the autistic population.[75]
- Preempted diagnoses. Although the DSM-IV rules out concurrent diagnosis of many other conditions along with autism, the full criteria for ADHD, Tourette syndrome, and other of these conditions are often present and these comorbid diagnoses are increasingly accepted.[76] A 2008 study found that nearly 70% of children with ASD had at least one psychiatric disorder, including nearly 30% with social anxiety disorder and similar proportions with ADHD and oppositional defiant disorder.[77] Childhood-onset schizophrenia, a rare and severe form, is another preempted diagnosis whose symptoms are often present along with the symptoms of autism.[78]
References
- 1 2 Elsabbagh M, Divan G, Yun-Joo Koh YJ et al.. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012;5(3):160–79. doi:10.1002/aur.239. PMID 22495912.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 Newschaffer CJ, Croen LA, Daniels J et al. The epidemiology of autism spectrum disorders [PDF]. Annu Rev Public Health. 2007;28:235–58. doi:10.1146/annurev.publhealth.28.021406.144007. PMID 17367287.
- 1 2 3 4 Rutter M. Incidence of autism spectrum disorders: changes over time and their meaning. Acta Paediatr. 2005;94(1):2–15. doi:10.1111/j.1651-2227.2005.tb01779.x. PMID 15858952.
- 1 2 Gardener H, Spiegelman D, Buka SL. Prenatal risk factors for autism: comprehensive meta-analysis. Br J Psychiatry. 2009;195(1):7–14. doi:10.1192/bjp.bp.108.051672. PMID 19567888.
- 1 2 3 Zafeiriou DI, Ververi A, Vargiami E. Childhood autism and associated comorbidities. Brain Dev. 2007;29(5):257–72. doi:10.1016/j.braindev.2006.09.003. PMID 17084999.
- 1 2 Levisohn PM. The autism-epilepsy connection. Epilepsia. 2007;48(Suppl 9):33–5. doi:10.1111/j.1528-1167.2007.01399.x. PMID 18047599.
- ↑ Trottier G, Srivastava L, Walker CD. Etiology of infantile autism: a review of recent advances in genetic and neurobiological research. J Psychiatry Neurosci. 1999;24(2):103–15. PMID 10212552.
- 1 2 Freitag CM. The genetics of autistic disorders and its clinical relevance: a review of the literature. Mol Psychiatry. 2007;12(1):2–22. doi:10.1038/sj.mp.4001896. PMID 17033636.
- ↑ Arndt TL, Stodgell CJ, Rodier PM. The teratology of autism. Int J Dev Neurosci. 2005;23(2–3):189–99. doi:10.1016/j.ijdevneu.2004.11.001. PMID 15749245.
- ↑ Wakefield's article linking MMR vaccine and autism was fraudulent. BMJ. 2011. 342:c7452. Retrieved April 2, 2012. http://www.bmj.com/content/342/bmj.c7452
- ↑ A J Wakefield, S H Murch, A Anthony, J Linnell, et al. Ileal-lymphoid-nodular hyperplasia, non-specific colitis, and pervasive developmental disorder in children. Vol 351. The Lancet. February 28, 1998. http://briandeer.com/mmr/lancet-paper.pdf
- 1 2 Coggon D, Rose G, Barker DJP. Epidemiology for the Uninitiated. 4th ed. BMJ; 1997. ISBN 0-7279-1102-3. Quantifying diseases in populations.
- 1 2 Scahill L, Bearss K. The rise in autism and the mercury myth. J Child Adolesc Psychiatr Nurs. 2009;22(1):51–3. doi:10.1111/j.1744-6171.2008.00152.x. PMID 19200293.
- ↑ Williams JG, Higgins JPT, Brayne CEG. Systematic review of prevalence studies of autism spectrum disorders [PDF]. Arch Dis Child. 2006;91(1):8–15. doi:10.1136/adc.2004.062083. PMID 15863467. PMC 2083083.
- ↑ Fombonne E. Epidemiology of autistic disorder and other pervasive developmental disorders. J Clin Psychiatry. 2005;66(Suppl 10):3–8. PMID 16401144.
- ↑ Baird G, Simonoff E, Pickles A et al. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006;368(9531):210–5. doi:10.1016/S0140-6736(06)69041-7. PMID 16844490.
- ↑ Caronna EB, Milunsky JM, Tager-Flusberg H. Autism spectrum disorders: clinical and research frontiers. Arch Dis Child. 2008;93(6):518–23. doi:10.1136/adc.2006.115337. PMID 18305076.
- ↑ Baron-Cohen S, Scott FJ, Allison C et al. Prevalence of autism-spectrum conditions: UK school-based population study [PDF]. Br J Psychiatry. 2009;194(6):500–9. doi:10.1192/bjp.bp.108.059345. PMID 19478287.
- 1 2 3 Rice Catherine PhD. Prevalence of autism spectrum disorders—Autism and Developmental Disabilities Monitoring Network, United States, 2006. MMWR Surveill Summ. 2009;58(SS-10):1–20. doi:10.1037/e562722010-001. PMID 20023608.
- ↑ Brugha T, McManus S, Meltzer H et al. Autism Spectrum Disorders in adults living in households throughout England: Report from the Adult Psychiatric Morbidity Survey 2007 [PDF]. NHS Information Centre for health and social care; 2009 [Retrieved 2010-02-16].
- ↑ Boseley S. Autism just as common in adults, so MMR jab is off the hook. Guardian. 2009-09-22.
- 1 2 Prevalence and changes in diagnostic practice:
- Fombonne E. The prevalence of autism. JAMA. 2003;289(1):87–9. doi:10.1001/jama.289.1.87. PMID 12503982.
- Wing L, Potter D. The epidemiology of autistic spectrum disorders: is the prevalence rising? Ment Retard Dev Disabil Res Rev. 2002;8(3):151–61. doi:10.1002/mrdd.10029. PMID 12216059.
- ↑ Wing L, Potter D. National Autistic Society. Notes on the prevalence of autism spectrum disorders; 1999 [Retrieved 2007-12-10].
- ↑ "Clarification of the definition of Pervasive Developmental Disorder Not Otherwise Specified".
- ↑ Five Easy Graphs, USDE figures
- ↑ Byrd RS, Sage AC, Keyzer J, et al. (2002). "Report to the legislature on the principal findings of the epidemiology of autism in California: a comprehensive pilot study" (PDF). M.I.N.D. Institute. Archived from the original (PDF) on 2008-04-14.
- 1 2 3 Shattuck PT. The contribution of diagnostic substitution to the growing administrative prevalence of autism in US special education. Pediatrics. 2006;117(4):1028–37. doi:10.1542/peds.2005-1516. PMID 16585296. Lay summary, 2006-04-03.
- ↑ Wazana A, Bresnahan M, Kline J. The autism epidemic: fact or artifact? J Am Acad Child Adolesc Psychiatry. 2007;46(6):721–30. doi:10.1097/chi.0b013e31804a7f3b. PMID 17513984.
- ↑ Bishop DVM, Whitehouse AJO, Watt HJ, Line EA. Autism and diagnostic substitution: evidence from a study of adults with a history of developmental language disorder. Dev Med Child Neurol. 2008;50(5):341–5. doi:10.1111/j.1469-8749.2008.02057.x. PMID 18384386.
- ↑ Parner ET, Schendel DE, Thorsen P. Autism prevalence trends over time in Denmark: changes in prevalence and age at diagnosis. Arch Pediatr Adolesc Med. 2008;162(12):1150–6. doi:10.1001/archpedi.162.12.1150. PMID 19047542.
- ↑ Hertz-Picciotto I, Delwiche L. The rise in autism and the role of age at diagnosis. Epidemiology. 2009;20(1):84–90. doi:10.1097/EDE.0b013e3181902d15. PMID 19234401. Lay summary: WebMD, 2009-01-08.
- ↑ Grether JK, Rosen NJ, Smith KS, Croen LA. Investigation of shifts in autism reporting in the California Department of Developmental Services. J Autism Dev Disord. 2009;39(10):1412–9. doi:10.1007/s10803-009-0754-z. PMID 19479197.
- ↑ Szpir M. Tracing the origins of autism: a spectrum of new studies. Environ Health Perspect. 2006;114(7):A412–8. doi:10.1289/ehp.114-a412. PMID 16835042. PMC 1513312.
- ↑ Mankoski RE, Collins M, Ndosi NK, Mgalla EH, Sarwatt VV, Folstein SE. Etiologies of autism in a case-series from Tanzania. J Autism Dev Disord. 2006;36(8):1039–51. doi:10.1007/s10803-006-0143-9. PMID 16897390.
- ↑ Childhood Autism in Canada: Some issues relating to behavioural intervention by Sonya Norris, Science and Technology Division; Jean-Rodrigue Paré, Political and Social Affairs Division; Sheena Starky, Economics Division, 2006.
- 1 2 3 Public Health Agency of Canada, Canada Communicable Disease Report, "Does Measles-Mumps-Rubella (MMR) Vaccination cause Inflammatory Bowel Disease and Autism?"
- ↑ Centers for Disease Control and Prevention
- ↑ "ASD Data and Statistics". CDC.gov. Archived from the original on 2014-04-18. Retrieved 5 Apr 2014.
- ↑ Rise in Autism Rate Misleading, study says CBC news quoting Paul Shattuck, 2006
- ↑ Barbaresi WJ, Katusic SK, Colligan RC, Weaver AL, Jacobsen SJ. The incidence of autism in Olmsted County, Minnesota, 1976-1997: results from a population-based study. Arch Pediatr Adolesc Med. 2005;159(1):37–44. doi:10.1001/archpedi.159.1.37. PMID 15630056.
- ↑ Barbaresi WJ, Colligan RC, Weaver AL, Katusic SK. The incidence of clinically diagnosed versus research-identified autism in Olmsted County, Minnesota, 1976–1997: results from a retrospective, population-based study. J Autism Dev Disord. 2008;39(3):464–70. doi:10.1007/s10803-008-0645-8. PMID 18791815.
- ↑ Montiel-Nava C, Peña JA. Epidemiological findings of pervasive developmental disorders in a Venezuelan study. Autism. 2008;12(2):191–202. doi:10.1177/1362361307086663. PMID 18308767.
- ↑ A review of the prevalence of Autism Spectrum Disorder in Asia. Research in Autism Spectrum Disorders. April 2010;4(2):156–167. doi:10.1016/j.rasd.2009.10.003.
- ↑ Wong VCN, Hui SLH. Epidemiological study of autism spectrum disorder in China. J Child Neurol. 2008;23(1):67–72. doi:10.1177/0883073807308702. PMID 18160559.
- ↑ Honda H, Shimizu Y, Rutter M. No effect of MMR withdrawal on the incidence of autism: a total population study. J Child Psychol Psychiatry. 2005;46(6):572–9. doi:10.1111/j.1469-7610.2005.01425.x. PMID 15877763. Lay summary: Bandolier, 2005.
- ↑ Senecky Y, Chodick G, Diamond G, Lobel D, Drachman R, Inbar D. Time trends in reported autistic spectrum disorders in Israel, 1972–2004 [PDF]. Isr Med Assoc J. 2009;11(1):30–3. PMID 19344009.
- ↑ Al-Salehi SM, Al-Hifthy EH, Ghaziuddin M. Autism in Saudi Arabia: presentation, clinical correlates and comorbidity. Transcult Psychiatry. 2009;46(2):340–7. doi:10.1177/1363461509105823. PMID 19541755.
- ↑ Madsen KM, Lauritsen MB, Pedersen CB et al. Thimerosal and the occurrence of autism: negative ecological evidence from Danish population-based data. Pediatrics. 2003;112(3):604–6. doi:10.1542/peds.112.3.604. PMID 12949291.
- ↑ Autisme Grande Cause
- ↑ Eric Fombonne., C. du Mazaubrun, Social Psychiatry and Psychiatric Epidemiology, 1992, 27, 203-210.
- ↑ Eric Fombonne et al., Journal of the American Academy of Child and Adolescent Psychiatry, 1997, 36: 1561-1569
- ↑ Expertise collective. Troubles mentaux. Dépistage et prévention chez l'enfant et chez l'adolescent. Inserm, 2003, 8
- ↑ Plan autisme 2008-2010
- ↑ Jean-François Chossy, La situation des autistes en France, besoins et perspectives, rapport remis au Premier ministre, La Documentation française : Paris, Septembre 2003.
- ↑ Bölte S, Poustka F, Holtmann M. Trends in autism spectrum disorder referrals. Epidemiology. 2008;19(3):519–20. doi:10.1097/EDE.0b013e31816a9e13. PMID 18414094.
- ↑ Posserud M, Lundervold AJ, Lie SA, Gillberg C. The prevalence of autism spectrum disorders: impact of diagnostic instrument and non-response bias. Soc Psychiatry Psychiatr Epidemiol. 2009. doi:10.1007/s00127-009-0087-4. PMID 19551326.
- ↑ National Autistic Society. Incidence of autism; 2004 [Retrieved 2007-12-10].
- ↑ Kaye JA, del Mar Melero-Montes M, Jick H. Mumps, measles, and rubella vaccine and the incidence of autism recorded by general practitioners: a time trend analysis. BMJ. 2001;322(7284):460–3. doi:10.1136/bmj.322.7284.460. PMID 11222420. PMC 26561.
- ↑ Deer B (8 February 2009). "MMR doctor Andrew Wakefield fixed data on autism". The Sunday Times. London. Retrieved 2009-02-09.
- ↑ Smeeth L, Cook C, Fombonne E et al. Rate of first recorded diagnosis of autism and other pervasive developmental disorders in United Kingdom general practice, 1988 to 2001. BMC Med. 2004;2:39. doi:10.1186/1741-7015-2-39. PMID 15535890. PMC 533883.
- ↑ Szatmari P, Jones MB. Genetic epidemiology of autism spectrum disorders. In: Volkmar FR. Autism and Pervasive Developmental Disorders. 2nd ed. Cambridge University Press; 2007. ISBN 0-521-54957-4. p. 157–78.
- 1 2 3 Folstein SE, Rosen-Sheidley B. Genetics of autism: complex aetiology for a heterogeneous disorder. Nat Rev Genet. 2001;2(12):943–55. doi:10.1038/35103559. PMID 11733747.
- ↑ Bolton P, Macdonald H, Pickles A et al. A case-control family history study of autism. J Child Psychol Psychiatry. 1994;35(5):877–900. doi:10.1111/j.1469-7610.1994.tb02300.x. PMID 7962246.
- 1 2 Sykes NH, Lamb JA. Autism: the quest for the genes. Expert Rev Mol Med. 2007;9(24):1–15. doi:10.1017/S1462399407000452. PMID 17764594.
- 1 2 Moss, B. G.; Chugani, D. C. (2014). "Increased Risk of Very Low Birth Weight, Rapid Postnatal Growth, and Autism in Underweight and Obese Mothers.". American Journal of Health Promotion. 28 (3): 181–188. doi:10.4278/ajhp.120705-QUAN-325.
- ↑ Schubert C. Male biological clock possibly linked to autism, other disorders. Nat Med. 2008;14(11):1170. doi:10.1038/nm1108-1170a. PMID 18989289.
- ↑ Geschwind DH (February 2009). "Advances in Autism". Annual Review of Medicine. 60 (1): 367–80. doi:10.1146/annurev.med.60.053107.121225. PMC 3645857
 . PMID 19630577.
. PMID 19630577. - ↑ Daniels JL, Forssen U, Hultman CM et al. Parental psychiatric disorders associated with autism spectrum disorders in the offspring. Pediatrics. 2008;121(5):e1357–62. doi:10.1542/peds.2007-2296. PMID 18450879. Lay summary: UNC News, 2008-05-05.
- ↑ Rogers SJ. What are infant siblings teaching us about autism in infancy? Autism Res. 2009;2(3):125–37. doi:10.1002/aur.81. PMID 19582867.
- ↑ Mazumdar S, King M, Liu K et al.. the spatial structure of autism in California 1992-2001 Health and Place. 2009;16:539–46. doi:10.1016/j.healthplace.2009.12.014. PMID 20097113.
- ↑ Dawson M, Mottron L, Gernsbacher MA. Learning in autism [PDF]. In: Byrne JH (ed.-in-chief), Roediger HL III (vol. ed.). Learning and Memory: A Comprehensive Reference. Vol. 2. Academic Press; 2008. doi:10.1016/B978-012370509-9.00152-2. ISBN 0-12-370504-5. p. 759–72.
- 1 2 White SW, Oswald D, Ollendick T, Scahill L. Anxiety in children and adolescents with autism spectrum disorders. Clin Psychol Rev. 2009;29(3):216–29. doi:10.1016/j.cpr.2009.01.003. PMID 19223098.
- ↑ MacNeil BM, Lopes VA, Minnes PM. Anxiety in children and adolescents with Autism Spectrum Disorders. Res Autism Spectr Disord. 2009;3(1):1–21. doi:10.1016/j.rasd.2008.06.001.
- ↑ Manzi B, Loizzo AL, Giana G, Curatolo P. Autism and metabolic diseases. J Child Neurol. 2008;23(3):307–14. doi:10.1177/0883073807308698. PMID 18079313.
- ↑ Ozgen HM, Hop JW, Hox JJ, Beemer FA, van Engeland H. Minor physical anomalies in autism: a meta-analysis. Mol Psychiatry. 2008. doi:10.1038/mp.2008.75. PMID 18626481.
- ↑ Steyaert JG, De La Marche W. What's new in autism? Eur J Pediatr. 2008;167(10):1091–101. doi:10.1007/s00431-008-0764-4. PMID 18597114.
- ↑ Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G. Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample. J Am Acad Child Adolesc Psychiatry. 2008;47(8):921–9. doi:10.1097/CHI.0b013e318179964f. PMID 18645422.
- ↑ Rapoport J, Chavez A, Greenstein D, Addington A, Gogtay N. Autism spectrum disorders and childhood-onset schizophrenia: clinical and biological contributions to a relation revisited. J Am Acad Child Adolesc Psychiatry. 2009;48(1):10–8. doi:10.1097/CHI.0b013e31818b1c63. PMID 19218893.