Cognitive behavioral therapy
| Cognitive behavioral therapy | |
|---|---|
| Intervention | |
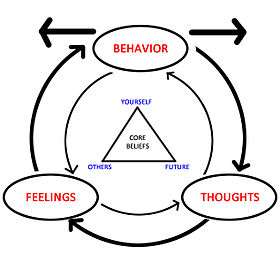 The diagram depicts how emotions, thoughts, and behaviors all influence each other. The triangle in the middle represents CBT's tenet that all humans' core beliefs can be summed up in three categories: self, others, future. | |
| MeSH | D015928 |
Cognitive behavioral therapy (CBT) is a psychosocial intervention[1][2] that is the most widely used evidence-based practice for treating mental disorders.[3] Guided by empirical research, CBT focuses on the development of personal coping strategies that target solving current problems and changing unhelpful patterns in cognitions (e.g., thoughts, beliefs, and attitudes), behaviors, and emotional regulation.[2][4] It was originally designed to treat depression, and is now used for a number of mental health conditions.[5][6]
The CBT model is based on a combination of the basic principles from behavioral and cognitive psychology.[2] It is different from historical approaches to psychotherapy, such as the psychoanalytic approach where the therapist looks for the unconscious meaning behind behaviors and then formulates a diagnosis. Instead, CBT is "problem-focused" and "action-oriented", meaning it is used to treat specific problems related to a diagnosed mental disorder and the therapist's role is to assist the client in finding and practising effective strategies to address the identified goals and decrease symptoms of the disorder.[7] CBT is based on the belief that thought distortions and maladaptive behaviors play a role in the development and maintenance of psychological disorders,[3] and that symptoms and associated distress can be reduced by teaching new information-processing skills and coping mechanisms.[1][7][8]
When compared to psychotropic medications, review studies have found CBT-alone to be as effective for treating less severe forms of depression and anxiety, posttraumatic stress disorder (PTSD), tics, substance abuse (with the exception of opioid use disorder), eating disorders, and borderline personality disorder, and it is often recommended in combination with medications for treating other conditions, such as severe obsessive compulsive disorder (OCD) and major depression, opioid addiction, bipolar, and psychotic disorders.[1] In addition, CBT is recommended as the first line of treatment for the majority of psychological disorders in children and adolescents, including aggression and conduct disorder.[1][4] Researchers have found that other bona fide therapeutic interventions were equally effective for treating certain conditions in adults,[9][10] but CBT was found to be superior in treating most disorders.[1] Along with interpersonal psychotherapy (IPT), CBT is recommended in treatment guidelines as a psychosocial treatment of choice,[1][11] and CBT and IPT are the only psychosocial interventions that psychiatry residents are mandated to be trained in.[1]
Description
Mainstream cognitive behavioral therapy assumes that changing maladaptive thinking leads to change in behavior and affect,[12] but recent variants emphasize changes in one's relationship to maladaptive thinking rather than changes in thinking itself.[13] The goal of cognitive behavioral therapy is not to diagnose a person with a particular disease, but to look at the person as a whole and decide what needs to be fixed. The basic steps in a cognitive-behavioral assessment include:
- Step 1: Identify critical behaviors
- Step 2: Determine whether critical behaviors are excesses or deficits
- Step 3: Evaluate critical behaviors for frequency, duration, or intensity (obtain a baseline)
- Step 4: If excess, attempt to decrease frequency, duration, or intensity of behaviors; if deficits, attempt to increase behaviors.[14]
These steps are based on a system created by Kanfer and Saslow.[15] After identifying the behaviors that need changing, whether they be in excess or deficit, and treatment has occurred, the psychologist must identify whether or not the intervention succeeded. For example, "If the goal was to decrease the behavior, then there should be a decrease relative to the baseline. If the critical behavior remains at or above the baseline, then the intervention has failed."[15]
Therapists or computer-based programs use CBT techniques to help individuals challenge their patterns and beliefs and replace "errors in thinking such as overgeneralizing, magnifying negatives, minimizing positives and catastrophizing" with "more realistic and effective thoughts, thus decreasing emotional distress and self-defeating behavior."[12] These errors in thinking are known as cognitive distortions. Cognitive distortions can be either a pseudo- discrimination belief or an over-generalization of something.[16] CBT techniques may also be used to help individuals take a more open, mindful, and aware posture toward them so as to diminish their impact.[13] Mainstream CBT helps individuals replace "maladaptive... coping skills, cognitions, emotions and behaviors with more adaptive ones",[17] by challenging an individual's way of thinking and the way that they react to certain habits or behaviors,[18] but there is still controversy about the degree to which these traditional cognitive elements account for the effects seen with CBT over and above the earlier behavioral elements such as exposure and skills training.[19]
Modern forms of CBT include a number of diverse but related techniques such as exposure therapy, stress inoculation training, cognitive processing therapy, cognitive therapy, relaxation training, dialectical behavior therapy, and acceptance and commitment therapy.[20] Some practitioners promote a form of mindful cognitive therapy which includes a greater emphasis on self-awareness as part of the therapeutic process.[21]
CBT has six phases:[17]
- Assessment or psychological assessment;
- Reconceptualization;
- Skills acquisition;
- Skills consolidation and application training;
- Generalization and maintenance;
- Post-treatment assessment follow-up.
The reconceptualization phase makes up much of the "cognitive" portion of CBT.[17] A summary of modern CBT approaches is given by Hofmann.[22]
There are different protocols for delivering cognitive behavioral therapy, with important similarities among them.[23] Use of the term CBT may refer to different interventions, including "self-instructions (e.g. distraction, imagery, motivational self-talk), relaxation and/or biofeedback, development of adaptive coping strategies (e.g. minimizing negative or self-defeating thoughts), changing maladaptive beliefs about pain, and goal setting".[17] Treatment is sometimes manualized, with brief, direct, and time-limited treatments for individual psychological disorders that are specific technique-driven. CBT is used in both individual and group settings, and the techniques are often adapted for self-help applications. Some clinicians and researchers are cognitively oriented (e.g. cognitive restructuring), while others are more behaviorally oriented (e.g. in vivo exposure therapy). Interventions such as imaginal exposure therapy combine both approaches.[24][25]
Medical uses
In adults, CBT has been shown to have effectiveness and a role in the treatment plans for anxiety disorders,[26][27] depression,[28][29] eating disorders,[30] chronic low back pain,[17] personality disorders,[31] psychosis,[32] schizophrenia,[33] substance use disorders,[34] in the adjustment, depression, and anxiety associated with fibromyalgia,[12] and with post-spinal cord injuries.[35]
In children or adolescents, CBT is an effective part of treatment plans for anxiety disorders,[36] body dysmorphic disorder,[37] depression and suicidality,[38] eating disorders and obesity,[39] obsessive–compulsive disorder,[40] and posttraumatic stress disorder,[41] as well as tic disorders, trichotillomania, and other repetitive behavior disorders.[42] CBT-SP, an adaptation of CBT for suicide prevention (SP), was specifically designed for treating youths who are severely depressed and who have recently attempted suicide within the past 90 days, and was found to be effective, feasible, and acceptable.[43] Sparx is a video game to help young persons, using the CBT method to teach them how to resolve their own issues. CBT has also been shown to be effective for posttraumatic stress disorder in very young children (3 to 6 years of age).[44] CBT has also been applied to a variety of childhood disorders,[45] including depressive disorders and various anxiety disorders.
Cochrane reviews have found no evidence that CBT is effective for tinnitus, although there appears to be an effect on management of associated depression and quality of life in this condition.[46] Other recent Cochrane Reviews found no convincing evidence that CBT training helps foster care providers manage difficult behaviors in the youths under their care,[47] nor was it helpful in treating men who abuse their intimate partners.[48]
According to a 2004 review by INSERM of three methods, cognitive behavioral therapy was either "proven" or "presumed" to be an effective therapy on several specific mental disorders.[49] According to the study, CBT was effective at treating schizophrenia, depression, bipolar disorder, panic disorder, post-traumatic stress, anxiety disorders, bulimia, anorexia, personality disorders and alcohol dependency.[49]
Some meta-analyses find CBT more effective than psychodynamic therapy and equal to other therapies in treating anxiety and depression.[50][51]
Computerized CBT (CCBT) has been proven to be effective by randomized controlled and other trials in treating depression and anxiety disorders,[27][29][52][53][54][55][56] including children,[57] as well as insomnia.[58] Some research has found similar effectiveness to an intervention of informational websites and weekly telephone calls.[59][60] CCBT was found to be equally effective as face-to-face CBT in adolescent anxiety[61] and insomnia.[58]
Criticism of CBT sometimes focuses on implementations (such as the UK IAPT) which may result initially in low quality therapy being offered by poorly trained practitioners.[62][63] However evidence supports the effectiveness of CBT for anxiety and depression.[54]
Mounting evidence suggests that the addition of hypnotherapy as an adjunct to CBT improves treatment efficacy for a variety of clinical issues.[64][65][66]
CBT has been applied in both clinical and non-clinical environments to treat disorders such as personality conditions and behavioral problems.[67] A systematic review of CBT in depression and anxiety disorders concluded that "CBT delivered in primary care, especially including computer- or Internet-based self-help programs, is potentially more effective than usual care and could be delivered effectively by primary care therapists."[52]
Emerging evidence suggests a possible role for CBT in the treatment of attention deficit hyperactivity disorder (ADHD);[68] hypochondriasis;[69] coping with the impact of multiple sclerosis;[70] sleep disturbances related to aging;[71] dysmenorrhea;[72] and bipolar disorder,[73] but more study is needed and results should be interpreted with caution. CBT can have a therapeutic effects on easing symptoms of anxiety and depression in people with Alzheimer's disease.[74] CBT has been studied as an aid in the treatment of anxiety associated with stuttering. Initial studies have shown CBT to be effective in reducing social anxiety in adults who stutter,[75] but not in reducing stuttering frequency.[76][77]
Martinez-Devesa et al. (2010) found no evidence that CBT is effective for tinnitus, although there appears to be an effect on management of associated depression and quality of life in this condition.[46] Turner et al. (2007) found no convincing evidence that CBT training helps foster care providers manage difficult behaviors in the youths under their care,[47] and Smedslund et al. (2007) found that it was not helpful in treating men who abuse their intimate partners.[48]
In the case of metastatic breast cancer, Edwards et al. (2008) maintained that the current body of evidence is not sufficient to rule out the possibility that psychological interventions may cause harm to women with this advanced neoplasm.[78]
There is some evidence that CBT is superior in the long-term to benzodiazepines and the nonbenzodiazepines in the treatment and management of insomnia.[79] CBT has been shown to be moderately effective for treating chronic fatigue syndrome.[80]
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) recommends CBT in the treatment plans for a number of mental health difficulties, including posttraumatic stress disorder, obsessive–compulsive disorder (OCD), bulimia nervosa, and clinical depression.[81]
Anxiety disorders
CBT has been shown to be effective in the treatment of adult anxiety disorders.[82]
A basic concept in some CBT treatments used in anxiety disorders is in vivo exposure. The term refers to the direct confrontation of feared objects, activities, or situations by a patient. For example, a woman with PTSD who fears the location where she was assaulted may be assisted by her therapist in going to that location and directly confronting those fears. Likewise, a person with social anxiety disorder who fears public speaking may be instructed to directly confront those fears by giving a speech.[83] This "two-factor" model is often credited to O. Hobart Mowrer.[84] Through exposure to the stimulus, this harmful conditioning can be "unlearned" (referred to as extinction and habituation). Studies have provided evidence that when examining animals and humans that glucocorticoids may possibly lead to a more successful extinction learning during exposure therapy. For instance, glucocorticoids can prevent aversive learning episodes from being retrieved and heighten reinforcement of memory traces creating a non-fearful reaction in feared situations. A combination of glucocorticoids and exposure therapy may be a better improved treatment for treating patients with anxiety disorders.[85]
Schizophrenia, psychosis and mood disorders
Cognitive behavioral therapy has been shown as an effective treatment for clinical depression.[28] The American Psychiatric Association Practice Guidelines (April 2000) indicated that, among psychotherapeutic approaches, cognitive behavioral therapy and interpersonal psychotherapy had the best-documented efficacy for treatment of major depressive disorder.[86] One etiological theory of depression is Aaron T. Beck's cognitive theory of depression. His theory states that depressed people think the way they do because their thinking is biased towards negative interpretations. According to this theory, depressed people acquire a negative schema of the world in childhood and adolescence as an effect of stressful life events, and the negative schema is activated later in life when the person encounters similar situations.[87]
Beck also described a negative cognitive triad, made up of the negative schemata and cognitive biases of the person, theorizing that depressed individuals make negative evaluations of themselves, the world, and the future. According to this theory, depressed people have views such as "I never do a good job", "It is impossible to have a good day", and "things will never get better." A negative schema helps give rise to the cognitive bias, and the cognitive bias helps fuel the negative schema. This is the negative triad. Beck further proposed that depressed people often have the following cognitive biases: arbitrary inference, selective abstraction, over-generalization, magnification, and minimization. These cognitive biases are quick to make negative, generalized, and personal inferences of the self, thus fueling the negative schema.[87]
In long-term psychoses, CBT is used to complement medication and is adapted to meet individual needs. Interventions particularly related to these conditions include exploring reality testing, changing delusions and hallucinations, examining factors which precipitate relapse, and managing relapses.[32] Several meta-analyses suggested that CBT is effective in schizophrenia,[33][88] and the American Psychiatric Association includes CBT in its schizophrenia guideline as an evidence-based treatment. There is also limited evidence of effectiveness for CBT in bipolar disorder[73] and severe depression.[89]
A 2010 meta-analysis found that no trial employing both blinding and psychological placebo has shown CBT to be effective in either schizophrenia or bipolar disorder, and that the effect size of CBT was small in major depressive disorder. They also found a lack of evidence to conclude that CBT was effective in preventing relapses in bipolar disorder.[90] Evidence that severe depression is mitigated by CBT is also lacking, with anti-depressant medications still viewed as significantly more effective than CBT,[28] although success with CBT for depression was observed beginning in the 1990s.[91]
According to Cox, Abramson, Devine, and Hollon (2012), cognitive behavioral therapy can also be used to reduce prejudice towards others. This other-directed prejudice can cause depression in the "others," or in the self when a person becomes part of a group he or she previously had prejudice towards (i.e. deprejudice).[92] "Devine and colleagues (2012) developed a successful Prejudice Perpetrator intervention with many conceptual parallels to CBT.[93] Like CBT, their intervention taught Sources to be aware of their automative thoughts and to intentionally deploy a variety of cognitive techniques against automatic stereotyping."[92]
| Measured outcome | Findings in words | Findings in numbers | Quality of evidence |
|---|---|---|---|
| Global effects | |||
| No change in mental state | CBT seems no better than other psychosocial treatments for mental state | RR 0.84 CI 0.64 to 1.09 | Very low |
| Relapse | Relapse was not reduced by CBT | RR 0.91 CI 0.63 to 1.32 | Low |
| Rehospitalisation | Rehospitalisation was not reduced by CBT | RR 0.86 CI 0.62 to 1.21 | |
| Social functioning | Social functioning was improved in the CBT group - at about 26 weeks - but it is unclear what this means in everyday life | MD 8.80 higher CI 4.07 to 21.67 | Very low |
| High quality of life | Quality of life was not changed in the CBT group | MD 1.86 lower CI 19.2 lower to 15.48 higher | |
| Adverse effects | |||
| Adverse effects (within 24–52 weeks of onset of therapy) | No more likely to have adverse effects with CBT | RR 2 CI 0.71 to 5.64 | Very low |
With older adults
CBT is used to help people of all ages, but the therapy should be adjusted based on the age of the patient with whom the therapist is dealing. Older individuals in particular have certain characteristics that need to be acknowledged and the therapy altered to account for these differences thanks to age.[95]
Prevention of mental illness
For anxiety disorders, use of CBT with people at risk has significantly reduced the number of episodes of generalized anxiety disorder and other anxiety symptoms, and also given significant improvements in explanatory style, hopelessness, and dysfunctional attitudes.[54][96][97] In another study, 3% of the group receiving the CBT intervention developed generalized anxiety disorder by 12 months postintervention compared with 14% in the control group.[98] Subthreshold panic disorder sufferers were found to significantly benefit from use of CBT.[99][100] Use of CBT was found to significantly reduce social anxiety prevalence.[101]
For depressive disorders, a stepped-care intervention (watchful waiting, CBT and medication if appropriate) achieved a 50% lower incidence rate in a patient group aged 75 or older.[102] Another depression study found a neutral effect compared to personal, social, and health education, and usual school provision, and included a comment on potential for increased depression scores from people who have received CBT due to greater self recognition and acknowledgement of existing symptoms of depression and negative thinking styles.[103] A further study also saw a neutral result.[104] A meta-study of the Coping with Depression course, a cognitive behavioural intervention delivered by a psychoeducational method, saw a 38% reduction in risk of major depression.[105]
For people at risk of psychosis, in 2014 the UK National Institute for Health and Care Excellence (NICE) recommended preventive CBT.[106][107]
Gambling addiction
CBT is also used for problem gambling addiction. The number of individuals who gamble is 1–3% around the world.[108] Cognitive behavioral therapy develop skills for relapse prevention and learn to control mind and manage high-risk cases.[109]
History
Philosophical roots
Precursors of certain fundamental aspects of CBT have been identified in various ancient philosophical traditions, particularly Stoicism.[110] Stoic philosophers, particularly Epictetus, believed logic could be used to identify and discard false beliefs that lead to destructive emotions, which has influenced the way modern cognitive-behavioral therapists identify cognitive distortions that contribute to depression and anxiety.[111] For example, Aaron T. Beck's original treatment manual for depression states, "The philosophical origins of cognitive therapy can be traced back to the Stoic philosophers".[112] Another example of Stoic influence on cognitive theorists is Epictetus on Albert Ellis.[113] A key philosophical figure who also influenced the development of CBT was John Stuart Mill.[114]
Behavior therapy roots
The modern roots of CBT can be traced to the development of behavior therapy in the early 20th century, the development of cognitive therapy in the 1960s, and the subsequent merging of the two. Groundbreaking work of behaviorism began with Watson's and Rayner's studies of conditioning in 1920.[115] Behaviorally-centered therapeutic approaches appeared as early as 1924[116] with Mary Cover Jones' work dedicated to the unlearning of fears in children.[117] These were the antecedents of the development of Joseph Wolpe's behavioral therapy in the 1950s.[115] It was the work of Wolpe and Watson, which was based on Ivan Pavlov's work on learning and conditioning, that influenced Hans Eysenck and Arnold Lazarus to develop new behavioral therapy techniques based on classical conditioning.[115][118] One of Eysenck's colleagues, Glenn Wilson showed that classical fear conditioning in humans could be controlled by verbally induced cognitive expectations,[119] thus opening a field of research that supports the rationale of cognitive behaviorial therapy.
During the 1950s and 1960s, behavioral therapy became widely utilized by researchers in the United States, the United Kingdom, and South Africa, who were inspired by the behaviorist learning theory of Ivan Pavlov, John B. Watson, and Clark L. Hull.[116] In Britain, Joseph Wolpe, who applied the findings of animal experiments to his method of systematic desensitization,[115] applied behavioral research to the treatment of neurotic disorders. Wolpe's therapeutic efforts were precursors to today's fear reduction techniques.[116] British psychologist Hans Eysenck presented behavior therapy as a constructive alternative.[116][120]
At the same time of Eysenck's work, B. F. Skinner and his associates were beginning to have an impact with their work on operant conditioning.[115][118] Skinner's work was referred to as radical behaviorism and avoided anything related to cognition.[115] However, Julian Rotter, in 1954, and Albert Bandura, in 1969, contributed behavior therapy with their respective work on social learning theory, by demonstrating the effects of cognition on learning and behavior modification.[115][118]
The emphasis on behavioral factors constituted the "first wave" of CBT.[121]
Cognitive therapy roots
One of the first therapists to address cognition in psychotherapy was Alfred Adler with his notion of basic mistakes and how they contributed to creation of unhealthy or useless behavioral and life goals.[122] Adler's work influenced the work of Albert Ellis,[122] who developed one of the earliest cognitive-based psychotherapies, known today as Rational emotive behavior therapy, or REBT.[123]
Around the same time that rational emotive therapy, as it was known then, was being developed, Aaron T. Beck was conducting free association sessions in his psychoanalytic practice.[124] During these sessions, Beck noticed that thoughts were not as unconscious as Freud had previously theorized, and that certain types of thinking may be the culprits of emotional distress.[124] It was from this hypothesis that Beck developed cognitive therapy, and called these thoughts "automatic thoughts".[124]
It was these two therapies, rational emotive therapy and cognitive therapy, that started the "second wave" of CBT, which was the emphasis on cognitive factors.[121]
Behavior and cognitive therapies merge
Although the early behavioral approaches were successful in many of the neurotic disorders, they had little success in treating depression.[115][116][125] Behaviorism was also losing in popularity due to the so-called "cognitive revolution". The therapeutic approaches of Albert Ellis and Aaron T. Beck gained popularity among behavior therapists, despite the earlier behaviorist rejection of "mentalistic" concepts like thoughts and cognitions.[115] Both of these systems included behavioral elements and interventions and primarily concentrated on problems in the present.
In initial studies, cognitive therapy was often contrasted with behavioral treatments to see which was most effective. During the 1980s and 1990s, cognitive and behavioral techniques were merged into cognitive behavioral therapy. Pivotal to this merging was the successful development of treatments for panic disorder by David M. Clark in the UK and David H. Barlow in the US.[116]
Over time, cognitive behavior therapy became to be known not only as a therapy, but as an umbrella term for all cognitive-based psychotherapies.[115] These therapies include, but are not limited to, rational emotive therapy, cognitive therapy, acceptance and commitment therapy, dialectical behavior therapy, reality therapy/choice theory, cognitive processing therapy, EMDR, and multimodal therapy.[115] All of these therapies are a blending of cognitive- and behavior-based elements.
This blending of theoretical and technical foundations from both behavior and cognitive therapies constitute the "third wave" of CBT,[121] which is the current wave.[121] The most prominent therapies of this third wave are dialectical behavior therapy and acceptance and commitment therapy.[121]
Methods of access
Therapist
A typical CBT programme would consist of face-to-face sessions between patient and therapist, made up of 6-18 sessions of around an hour each with a gap of a 1–3 weeks between sessions. This initial programme might be followed by some booster sessions, for instance after one month and three months.[126] CBT has also been found to be effective if patient and therapist type in real time to each other over computer links.[127][128]
Cognitive behavioral therapy is most closely allied with the scientist–practitioner model in which clinical practice and research is informed by a scientific perspective, clear operationalization of the problem, and an emphasis on measurement, including measuring changes in cognition and behavior and in the attainment of goals. These are often met through "homework" assignments in which the patient and the therapist work together to craft an assignment to complete before the next session.[129] The completion of these assignments – which can be as simple as a person suffering from depression attending some kind of social event – indicates a dedication to treatment compliance and a desire to change.[129] The therapists can then logically gauge the next step of treatment based on how thoroughly the patient completes the assignment.[129] Effective cognitive behavioral therapy is dependent on a therapeutic alliance between the healthcare practitioner and the person seeking assistance.[2][130] Unlike many other forms of psychotherapy, the patient is very involved in CBT.[129] For example, an anxious patient may be asked to talk to a stranger as a homework assignment, but if that is too difficult, he or she can work out an easier assignment first.[129] The therapist needs to be flexible and willing to listen to the patient rather than acting as an authority figure.[129]
Computerized or internet-delivered
Computerized cognitive behavioral therapy (CCBT) has been described by NICE as a "generic term for delivering CBT via an interactive computer interface delivered by a personal computer, internet, or interactive voice response system",[131] instead of face-to-face with a human therapist. It is also known as internet-delivered cognitive behavioral therapy or ICBT.[132] CCBT has potential to improve access to evidence-based therapies, and to overcome the prohibitive costs and lack of availability sometimes associated with retaining a human therapist.[133] In this context, it is important not to confuse CBT with 'computer-based training', which nowadays is more commonly referred to as e-Learning.
CCBT has been found in meta-studies to be cost-effective and often cheaper than usual care,[134][135] including for anxiety.[136] Studies have shown that individuals with social anxiety and depression experienced improvement with online CBT-based methods.[137] A review of current CCBT research in the treatment of OCD in children found this interface to hold great potential for future treatment of OCD in youths and adolescent populations.[138] CCBT is also predisposed to treating mood disorders amongst non-heterosexual populations, who may avoid face-to-face therapy from fear of stigma. However presently CCBT programs seldom cater to these populations.[139]
A key issue in CCBT use is low uptake and completion rates, even when it has been clearly made available and explained.[140][141] CCBT completion rates and treatment efficacy have been found in some studies to be higher when use of CCBT is supported personally, with supporters not limited only to therapists, than when use is in a self-help form alone.[134][142] Another approach to improving uptake and completion rate, as well as treatment outcome, is to design software that supports the formation of a strong therapeutic alliance between the user and the technology.[143]
In February 2006 NICE recommended that CCBT be made available for use within the NHS across England and Wales for patients presenting with mild-to-moderate depression, rather than immediately opting for antidepressant medication,[131] and CCBT is made available by some health systems.[144] The 2009 NICE guideline recognized that there are likely to be a number of computerized CBT products that are useful to patients, but removed endorsement of any specific product.[145]
A relatively new avenue of research is the combination of artificial intelligence and CCBT. It has been proposed to use modern technology to create CCBT that simulates face-to-face therapy. This might be achieved in cognitive behaviour therapy for a specific disorder using the comprehensive domain knowledge of CBT.[146] One area where this has been attempted is the specific domain area of social anxiety in those who stutter.[147]
Reading self-help materials
Enabling patients to read self-help CBT guides has been shown to be effective by some studies.[148][149][150] However one study found a negative effect in patients who tended to ruminate,[151] and another meta-analysis found that the benefit was only significant when the self-help was guided (e.g. by a medical professional).[152]
Group educational course
Patient participation in group courses has been shown to be effective.[153] In a meta-analysis reviewing evidence-based treatment of OCD in children, individual CBT was found to be more efficacious than group CBT.[138]
Types
Brief CBT
Brief cognitive behavioral therapy (BCBT) is a form of CBT which has been developed for situations in which there are time constraints on the therapy sessions.[154] BCBT takes place over a couple of sessions that can last up to 12 accumulated hours by design. This technique was first implemented and developed on soldiers overseas in active duty by David M. Rudd to prevent suicide.[154]
Breakdown of treatment[154]
- Orientation
- Commitment to treatment
- Crisis response and safety planning
- Means restriction
- Survival kit
- Reasons for living card
- Model of suicidality
- Treatment journal
- Lessons learned
- Skill focus
- Skill development worksheets
- Coping cards
- Demonstration
- Practice
- Skill refinement
- Relapse prevention
- Skill generalization
- Skill refinement
Cognitive emotional behavioral therapy
Cognitive emotional behavioral therapy (CEBT) is a form of CBT developed initially for individuals with eating disorders but now used with a range of problems including anxiety, depression, obsessive compulsive disorder (OCD), post-traumatic stress disorder (PTSD) and anger problems. It combines aspects of CBT and dialectical behavioural therapy and aims to improve understanding and tolerance of emotions in order to facilitate the therapeutic process. It is frequently used as a "pretreatment" to prepare and better equip individuals for longer-term therapy.[155]
Structured cognitive behavioral training
Structured cognitive behavioral training (SCBT) is a cognitive-based process with core philosophies that draw heavily from CBT. Like CBT, SCBT asserts that behavior is inextricably related to beliefs, thoughts and emotions. SCBT also builds on core CBT philosophy by incorporating other well-known modalities in the fields of behavioral health and psychology: most notably, Albert Ellis's Rational Emotive Behavior Therapy. SCBT differs from CBT in two distinct ways. First, SCBT is delivered in a highly regimented format. Second, SCBT is a predetermined and finite training process that becomes personalized by the input of the participant. SCBT is designed with the intention to bring a participant to a specific result in a specific period of time. SCBT has been used to challenge addictive behavior, particularly with substances such as tobacco, alcohol and food, and to manage diabetes and subdue stress and anxiety. SCBT has also been used in the field of criminal psychology in the effort to reduce recidivism.
Moral reconation therapy
Moral reconation therapy, a type of CBT used to help felons overcome antisocial personality disorder (ASPD), slightly decreases the risk of further offending.[156] It is generally implemented in a group format because of the risk of offenders with ASPD being given one-on-one therapy reinforces narcissistic behavioral characteristics, and can be used in correctional or outpatient settings. Groups usually meet weekly for two to six months.[157]
Stress inoculation training
This type of therapy uses a blend of cognitive, behavioral and some humanistic training techniques to target the stressors of the client. This usually is used to help clients better cope with their stress or anxiety after stressful events.[158] This is a three-phase process that trains the client to use skills that they already have to better adapt to their current stressors. The first phase is an interview phase that includes psychological testing, client self-monitoring, and a variety of reading materials. This allows the therapist to individually tailor the training process to the client.[158] Clients learn how to categorize problems into emotion-focused or problem-focused, so that they can better treat their negative situations. This phase ultimately prepares the client to eventually confront and reflect upon their current reactions to stressors, before looking at ways to change their reactions and emotions in relation to their stressors. The focus is conceptualization.[158]
The second phase emphasizes the aspect of skills acquisition and rehearsal that continues from the earlier phase of conceptualization. The client is taught skills that help them cope with their stressors. These skills are then practised in the space of therapy. These skills involve self-regulation, problem-solving, interpersonal communication skills, etc.[158]
The third and final phase is the application and following through of the skills learned in the training process. This gives the client opportunities to apply their learned skills to a wide range of stressors. Activities include role-playing, imagery, modeling, etc. In the end, the client will have been trained on a preventative basis to inoculate personal, chronic, and future stressors by breaking down their stressors into problems they will address in long-term, short-term, and intermediate coping goals.[158]
Criticisms
Relative effectiveness
The research conducted for CBT has been a topic of sustained controversy. While some researchers write that CBT is more effective than other treatments,[159] many other researchers[9][160][161] and practitioners[162][163] have questioned the validity of such claims. For example, one study[159] determined CBT to be superior to other treatments in treating anxiety and depression. However, researchers[9] responding directly to that study conducted a re-analysis and found no evidence of CBT being superior to other bona fide treatments, and conducted an analysis of thirteen other CBT clinical trials and determined that they failed to provide evidence of CBT superiority.
A major criticism has been that clinical studies of CBT efficacy (or any psychotherapy) are not double-blind (i.e., either the subjects or the therapists in psychotherapy studies are not blind to the type of treatment). They may be single-blinded, i.e. the rater may not know the treatment the patient received, but neither the patients nor the therapists are blinded to the type of therapy given (two out of three of the persons involved in the trial, i.e., all of the persons involved in the treatment, are unblinded). The patient is an active participant in correcting negative distorted thoughts, thus quite aware of the treatment group they are in.[164]
The importance of double-blinding was shown in a meta-analysis that examined the effectiveness of CBT when placebo control and blindedness were factored in.[165] Pooled data from published trials of CBT in schizophrenia, major depressive disorder (MDD), and bipolar disorder that used controls for non-specific effects of intervention were analyzed. This study concluded that CBT is no better than non-specific control interventions in the treatment of schizophrenia and does not reduce relapse rates; treatment effects are small in treatment studies of MDD, and it is not an effective treatment strategy for prevention of relapse in bipolar disorder. For MDD, the authors note that the pooled effect size was very low. Nevertheless, the methodological processes used to select the studies in the previously mentioned meta-analysis and the worth of its findings have been called into question.[166][167][168]
Declining effectiveness
Additionally, a recent meta-analysis revealed that the positive effects of CBT on depression have been declining since 1977. The overall results showed two different declines in effect sizes: 1) an overall decline between 1977 and 2014, and 2) a steeper decline between 1995 and 2014. Additional sub-analysis revealed that CBT studies where therapists in the test group were instructed to adhere to the Beck CBT manual had a steeper decline in effect sizes since 1977 than studies where therapists in the test group were instructed to use CBT without a manual. The authors reported that they were unsure why the effects were declining but did list inadequate therapist training, failure to adhere to a manual, lack of therapist experience, and patients' hope and faith in its efficacy waning as potential reasons. The authors did mention that the current study was limited to depressive disorders only.[169]
High drop-out rates
Furthermore, other researchers[160] write that CBT studies have high drop-out rates compared to other treatments. At times, the CBT drop-out rates can be more than five times higher than other treatments groups. For example, the researchers provided statistics of 28 participants in a group receiving CBT therapy dropping out, compared to 5 participants in a group receiving problem-solving therapy dropping out, or 11 participants in a group receiving psychodynamic therapy dropping out.[160] This high drop-out rate is also evident in the treatment of several disorders, particularly the eating disorder anorexia nervosa, which is commonly treated with CBT. Those treated with CBT have a high chance of dropping out of therapy before completion and reverting to their anorexia behaviors.[170]
Other researchers[161] conducting an analysis of treatments for youths who self-injure found similar drop-out rates in CBT and DBT groups. In this study, the researchers analyzed several clinical trials that measured the efficacy of CBT administered to youths who self-injure. The researchers concluded that none of them were found to be efficacious. These conclusions[161] were made using the APA Division 12 Task Force on the Promotion and Dissemination of Psychological Procedures to determine intervention potency.[171]
Philosophical concerns with CBT methods
The methods employed in CBT research have not been the only criticisms; some individuals have called its theory and therapy into question. For example, Fancher[163] argues that CBT has failed to provide a framework for clear and correct thinking. He states that it is strange for CBT theorists to develop a framework for determining distorted thinking without ever developing a framework for "cognitive clarity" or what would count as "healthy, normal thinking." Additionally, he writes that irrational thinking cannot be a source of mental and emotional distress when there is no evidence of rational thinking causing psychological well-being. Or, that social psychology has proven the normal cognitive processes of the average person to be irrational, even those who are psychologically well. Fancher also says that the theory of CBT is inconsistent with basic principles and research of rationality, and even ignores many rules of logic. He argues that CBT makes something of thinking that is far less exciting and true than thinking probably is. Among his other arguments are the maintaining of the status quo promoted in CBT, the self-deception encouraged within clients and patients engaged in CBT, how poorly the research is conducted, and some of its basic tenets and norms: "The basic norm of cognitive therapy is this: except for how the patient thinks, everything is ok".[172]
Meanwhile, Slife and Williams[162] write that one of the hidden assumptions in CBT is that of determinism, or the absence of free will. They argue that CBT invokes a type of cause-and-effect relationship with cognition. They state that CBT holds that external stimuli from the environment enter the mind, causing different thoughts that cause emotional states. Nowhere in CBT theory is agency, or free will, accounted for. At its most basic foundational assumptions, CBT holds that human beings have no free will and are just determined by the cognitive processes invoked by external stimuli.
Another criticism of CBT theory, especially as applied to Major Depressive Disorder (MDD), is that it confounds the symptoms of the disorder with its causes.[164]
Side effects
CBT is generally seen as having very low if any side effects.[173][174][175] Calls have been made for more appraisal of CBT side effects.[176][177]
Society and culture
The UK's National Health Service announced in 2008 that more therapists would be trained to provide CBT at government expense[178] as part of an initiative called Improving Access to Psychological Therapies (IAPT).[179] NICE said that CBT would become the mainstay of treatment for non-severe depression, with medication used only in cases where CBT had failed.[178] Therapists complained that the data does not fully support the attention and funding CBT receives. Psychotherapist and professor Andrew Samuels stated that this constitutes "a coup, a power play by a community that has suddenly found itself on the brink of corralling an enormous amount of money ... Everyone has been seduced by CBT's apparent cheapness."[178][180] The UK Council for Psychotherapy issued a press release in 2012 saying that the IAPT's policies were undermining traditional psychotherapy and criticized proposals that would limit some approved therapies to CBT,[181] claiming that they restricted patients to "a watered down version of cognitive behavioural therapy (CBT), often delivered by very lightly trained staff".[181]
NICE also recommends offering CBT to people suffering from schizophrenia, as well as those at risk of suffering from a psychotic episode.[182]
References
- 1 2 3 4 5 6 7 Hollon SD, Beck AT (2013). "Chapter 11 Cognitive and Cognitive-Behavioral Therapies". In MJ Lambert. Bergin and Garfield's Handbook of Psychotherapy and Behavior Change (6th ed.). Hoboken, NJ: John Wiley & Sons. pp. 393–394. ISBN 9781118418680.
- 1 2 3 4 Beck JS (2011), Cognitive behavior therapy: Basics and beyond (2nd ed.), New York, NY: The Guilford Press, pp. 19–20
- 1 2 Field TA, Beeson ET, Jones LK (2015), "The New ABCs: A Practitioner's Guide to Neuroscience-Informed Cognitive-Behavior Therapy" (PDF), Journal of Mental Health Counseling, 37 (3): 206–220, doi:10.17744/1040-2861-37.3.206
- 1 2 Benjamin CL, Puleo CM, Settipani CA, et al. (2011), "History of cognitive-behavioral therapy in youth", Child and Adolescent Psychiatric Clinics of North America, 20 (2): 179–189, doi:10.1016/j.chc.2011.01.011, PMC 3077930
 , PMID 21440849
, PMID 21440849 - ↑ McKay D, Sookman D, Neziroglu F, Wilhelm S, Stein DJ, Kyrios M, Matthews K, Veale D (28 February 2015). "Efficacy of cognitive-behavioral therapy for obsessive-compulsive disorder.". Psychiatry Research. 225 (3): 236–246. doi:10.1016/j.psychres.2014.11.058. PMID 25613661.
- ↑ Zhu Z, Zhang L, Jiang J, et al. (December 2014). "Comparison of psychological placebo and waiting list control conditions in the assessment of cognitive behavioral therapy for the treatment of generalized anxiety disorder: a meta-analysis.". Shanghai archives of psychiatry. 26 (6): 319–31. doi:10.11919/j.issn.1002-0829.214173. PMID 25642106.
- 1 2 Schacter DL, Gilbert DT, Wegner DM (2010), Psychology (2nd ed.), New York: Worth Pub, p. 600
- ↑ Brewin C (1996). "Theoretical foundations of cognitive-behavioral therapy for anxiety and depression". Annual Review of Psychology. 47: 33–57. doi:10.1146/annurev.psych.47.1.33.
- 1 2 3 Baardseth TP, Goldberg SB, Pace BT, Wislocki AP, Frost ND, et al. (2013). "Cognitive-behavioral therapy versus other therapies: Redux". Clinical Psychology Review. 33: 395–405. doi:10.1016/j.cpr.2013.01.004.
- ↑ Shedler J (2010). "The efficacy of psychodynamic psychotherapy". American Psychologist. 65 (2): 98–109. doi:10.1037/a0018378. PMID 20141265.
- ↑ Barth; et al., "Comparative Efficacy of Seven Psychotherapeutic Interventions for Patients with Depression: A Network Meta-Analysis", PLoS Med, 10 (5): e1001454, doi:10.1371/journal.pmed.1001454
- 1 2 3 Hassett, Afton L.; Gevirtz, Richard N. (2009). "Nonpharmacologic Treatment for Fibromyalgia: Patient Education, Cognitive-Behavioral Therapy, Relaxation Techniques, and Complementary and Alternative Medicine". Rheumatic Disease Clinics of North America. 35 (2): 393–407. doi:10.1016/j.rdc.2009.05.003. PMC 2743408. PMID 19647150.
- 1 2 Hayes, Steven C.; Villatte, Matthieu; Levin, Michael; Hildebrandt, Mikaela (2011). "Open, Aware, and Active: Contextual Approaches as an Emerging Trend in the Behavioral and Cognitive Therapies". Annual Review of Clinical Psychology. 7 (1): 141–68. doi:10.1146/annurev-clinpsy-032210-104449. PMID 21219193.
- ↑ Kaplan, Robert; Saccuzzo, Dennis. Psychological Testing. Wadsworth. pp. 415, Table 15.3.
- 1 2 Kaplan, Robert; Saccuzzo, Dennis. Psychological Testing. Wadsworth. p. 415.
- ↑ Dawes, RM (April 1964). "COGNITIVE DISTORTION Monograph Supplement 4-V14". Psychological Reports. 14 (2): 443–459. doi:10.2466/pr0.1964.14.2.443.
- 1 2 3 4 5 Gatchel, Robert J.; Rollings, Kathryn H. (2008). "Evidence-informed management of chronic low back pain with cognitive behavioral therapy". The Spine Journal. 8 (1): 40–4. doi:10.1016/j.spinee.2007.10.007. PMC 3237294. PMID 18164452.
- ↑ Kozier B (2008). Fundamentals of nursing: concepts, process and practice. Pearson Education. p. 187. ISBN 978-0-13-197653-5.
- ↑ Longmore, Richard J.; Worrell, Michael (2007). "Do we need to challenge thoughts in cognitive behavior therapy?". Clinical Psychology Review. 27 (2): 173–87. doi:10.1016/j.cpr.2006.08.001. PMID 17157970.
- ↑ E. B. Foa, Effective Treatments for PTSD: Practice Guidelines from the International Society for Traumatic Stress Studies, Guilford, New York, NY, USA, 2nd edition, 2009.
- ↑ Graham, Michael C. (2014). Facts of Life: ten issues of contentment. Outskirts Press. ISBN 978-1-4787-2259-5.
- ↑ Hofmann SG (2011). An Introduction to Modern CBT. Psychological Solutions to Mental Health Problems. Chichester, UK: Wiley-Blackwell. ISBN 0-470-97175-4.
- ↑ Hofmann, Stefan G.; Sawyer, Alice T.; Fang, Angela (2010). "The Empirical Status of the "New Wave" of Cognitive Behavioral Therapy". Psychiatric Clinics of North America. 33 (3): 701–10. doi:10.1016/j.psc.2010.04.006. PMC 2898899. PMID 20599141.
- ↑ Foa, Edna B.; Rothbaum, Barbara O.; Furr, Jami M. (Jan 2003). "Augmenting exposure therapy with other CBT procedures". Psychiatric Annals. 33 (1): 47–53. doi:10.3928/0048-5713-20030101-08.
- ↑ Jessamy, Hibberd; Jo, Usmar. This book will make you happy. Quercus. ISBN 9781848662810. Retrieved 15 July 2014.
- ↑ Otte, C (2011). "Cognitive behavioral therapy in anxiety disorders: Current state of the evidence". Dialogues in clinical neuroscience. 13 (4): 413–21. PMC 3263389. PMID 22275847.
- 1 2 Robinson, Emma; Titov, Nickolai; Andrews, Gavin; McIntyre, Karen; Schwencke, Genevieve; Solley, Karen (2010). García, Antonio Verdejo, ed. "Internet Treatment for Generalized Anxiety Disorder: A Randomized Controlled Trial Comparing Clinician vs. Technician Assistance". PLoS ONE. 5 (6): e10942. Bibcode:2010PLoSO...510942R. doi:10.1371/journal.pone.0010942. PMC 2880592. PMID 20532167.
- 1 2 3 Driessen, Ellen; Hollon, Steven D. (2010). "Cognitive Behavioral Therapy for Mood Disorders: Efficacy, Moderators and Mediators". Psychiatric Clinics of North America. 33 (3): 537–55. doi:10.1016/j.psc.2010.04.005. PMC 2933381. PMID 20599132.
- 1 2 Foroushani, Pooria; Schneider, Justine; Assareh, Neda (2011). "Meta-review of the effectiveness of computerised CBT in treating depression". BMC Psychiatry. 11 (1): 131. doi:10.1186/1471-244X-11-131. PMC 3180363. PMID 21838902.
- ↑ Murphy, Rebecca; Straebler, Suzanne; Cooper, Zafra; Fairburn, Christopher G. (2010). "Cognitive Behavioral Therapy for Eating Disorders". Psychiatric Clinics of North America. 33 (3): 611–27. doi:10.1016/j.psc.2010.04.004. PMC 2928448. PMID 20599136.
- ↑ Matusiewicz, Alexis K.; Hopwood, Christopher J.; Banducci, Annie N.; Lejuez, C.W. (2010). "The Effectiveness of Cognitive Behavioral Therapy for Personality Disorders". Psychiatric Clinics of North America. 33 (3): 657–85. doi:10.1016/j.psc.2010.04.007. PMC 3138327. PMID 20599139.
- 1 2 Gutiérrez, M; Sánchez, M; Trujillo, A; Sánchez, L (2009). "Cognitive-behavioral therapy for chronic psychosis" (PDF). Actas espanolas de psiquiatria. 37 (2): 106–14. PMID 19401859.
- 1 2 Rathod, Shanaya; Phiri, Peter; Kingdon, David (2010). "Cognitive Behavioral Therapy for Schizophrenia". Psychiatric Clinics of North America. 33 (3): 527–36. doi:10.1016/j.psc.2010.04.009. PMID 20599131.
- ↑ McHugh, R. Kathryn; Hearon, Bridget A.; Otto, Michael W. (2010). "Cognitive Behavioral Therapy for Substance Use Disorders". Psychiatric Clinics of North America. 33 (3): 511–25. doi:10.1016/j.psc.2010.04.012. PMC 2897895. PMID 20599130.
- ↑ Mehta, Swati; Orenczuk, Steven; Hansen, Kevin T.; Aubut, Jo-Anne L.; Hitzig, Sander L.; Legassic, Matthew; Teasell, Robert W.; Spinal Cord Injury Rehabilitation Evidence Research Team (2011). "An evidence-based review of the effectiveness of cognitive behavioral therapy for psychosocial issues post-spinal cord injury". Rehabilitation Psychology. 56 (1): 15–25. doi:10.1037/a0022743. PMC 3206089. PMID 21401282.
- ↑ Seligman, Laura D.; Ollendick, Thomas H. (2011). "Cognitive-Behavioral Therapy for Anxiety Disorders in Youth". Child and Adolescent Psychiatric Clinics of North America. 20 (2): 217–38. doi:10.1016/j.chc.2011.01.003. PMC 3091167. PMID 21440852.
- ↑ Phillips, Katharine A.; Rogers, Jamison (2011). "Cognitive-Behavioral Therapy for Youth with Body Dysmorphic Disorder: Current Status and Future Directions". Child and Adolescent Psychiatric Clinics of North America. 20 (2): 287–304. doi:10.1016/j.chc.2011.01.004. PMC 3070293. PMID 21440856.
- ↑ Spirito, Anthony; Esposito-Smythers, Christianne; Wolff, Jennifer; Uhl, Kristen (2011). "Cognitive-Behavioral Therapy for Adolescent Depression and Suicidality". Child and Adolescent Psychiatric Clinics of North America. 20 (2): 191–204. doi:10.1016/j.chc.2011.01.012. PMC 3073681. PMID 21440850.
- ↑ Wilfley, Denise E.; Kolko, Rachel P.; Kass, Andrea E. (2011). "Cognitive-Behavioral Therapy for Weight Management and Eating Disorders in Children and Adolescents". Child and Adolescent Psychiatric Clinics of North America. 20 (2): 271–85. doi:10.1016/j.chc.2011.01.002. PMC 3065663. PMID 21440855.
- ↑ Boileau, B (2011). "A review of obsessive-compulsive disorder in children and adolescents". Dialogues in clinical neuroscience. 13 (4): 401–11. PMC 3263388. PMID 22275846.
- ↑ Kowalik, Joanna; Weller, Jennifer; Venter, Jacob; Drachman, David (2011). "Cognitive behavioral therapy for the treatment of pediatric posttraumatic stress disorder: A review and meta-analysis". Journal of Behavior Therapy and Experimental Psychiatry. 42 (3): 405–13. doi:10.1016/j.jbtep.2011.02.002. PMID 21458405.
- ↑ Flessner, Christopher A. (2011). "Cognitive-Behavioral Therapy for Childhood Repetitive Behavior Disorders: Tic Disorders and Trichotillomania". Child and Adolescent Psychiatric Clinics of North America. 20 (2): 319–28. doi:10.1016/j.chc.2011.01.007. PMC 3074180. PMID 21440858.
- ↑ Stanley B.; Brown G.; Brent D.A.; Wells K.; Poling K.; Curry J.; Kennard B.D.; Wagner A.; Cwik M.F.; Klomek A.B.; Goldstein T.; Vitiello B.; Barnett S.; Daniel S.; Hughes J. (2009). "Cognitive-Behavioral Therapy for Suicide Prevention (CBT-SP): Treatment model, feasibility, and acceptability". Journal of the American Academy of Psychiatry. 48 (10): 1005–1013. doi:10.1097/chi.0b013e3181b5dbfe.
- ↑ Scheeringa, Michael S.; Weems, Carl F.; Cohen, Judith A.; Amaya-Jackson, Lisa; Guthrie, Donald (2011). "Trauma-focused cognitive-behavioral therapy for posttraumatic stress disorder in three-through six year-old children: A randomized clinical trial". Journal of Child Psychology and Psychiatry. 52 (8): 853–60. doi:10.1111/j.1469-7610.2010.02354.x. PMC 3116969. PMID 21155776.
- ↑ Reinicke, M., Dattillo, F., Freeman, A., (Eds.), 2003. Cognitive Therapy with Children and Adolescents, Second Edition: A Casebook for Clinical Practice. ISBN 978-1572308534
- 1 2 Martinez-Devesa, Pablo; Perera, Rafael; Theodoulou, Megan; Waddell, Angus (2010). Martinez-Devesa, Pablo, ed. "Cognitive behavioural therapy for tinnitus". Cochrane Database of Systematic Reviews (9): CD005233. doi:10.1002/14651858.CD005233.pub3. PMID 20824844.
- 1 2 Turner, William; MacDonald, Geraldine; Dennis, Jane A (2007). Turner, William, ed. "Behavioural and cognitive behavioural training interventions for assisting foster carers in the management of difficult behaviour". Cochrane Database of Systematic Reviews (1): CD003760. doi:10.1002/14651858.CD003760.pub3. PMID 17253496.
- 1 2 Smedslund, Geir; Dalsbø, Therese K; Steiro, Asbjørn; Winsvold, Aina; Clench-Aas, Jocelyne (2007). Smedslund, Geir, ed. "Cognitive behavioural therapy for men who physically abuse their female partner". Cochrane Database of Systematic Reviews (3): CD006048. doi:10.1002/14651858.CD006048.pub2. PMID 17636823.
- 1 2 INSERM Collective Expertise Centre (2000). "Psychotherapy: Three approaches evaluated". PMID 21348158.
- ↑ Tolin, David F. (2010). "Is cognitive–behavioral therapy more effective than other therapies?A meta-analytic review". Clinical Psychology Review. 30 (6): 710–20. doi:10.1016/j.cpr.2010.05.003. PMID 20547435.
- ↑ Cuijpers, Pim; Van Straten, Annemieke; Andersson, Gerhard; Van Oppen, Patricia (2008). "Psychotherapy for depression in adults: A meta-analysis of comparative outcome studies". Journal of Consulting and Clinical Psychology. 76 (6): 909–22. doi:10.1037/a0013075. PMID 19045960.
- 1 2 Hoifodt, R. S.; Strøm, C.; Kolstrup, N.; Eisemann, M.; Waterloo, K. (2011). "Effectiveness of cognitive behavioural therapy in primary health care: A review". Family Practice. 28 (5): 489–504. doi:10.1093/fampra/cmr017. PMID 21555339.
- ↑ https://web.archive.org/web/20130221021730/http://www.ehub.anu.edu.au/assist/about/research.php. Archived from the original on February 21, 2013. Retrieved November 22, 2012. Missing or empty
|title=(help) - 1 2 3 Titov, Nickolai; Andrews, Gavin; Sachdev, Perminder (2010). "Computer-delivered cognitive behavioural therapy: Effective and getting ready for dissemination". F1000 Medicine Reports. 2: 49. doi:10.3410/M2-49. PMC 2950044. PMID 20948835.
- ↑ Williams, Alishia D; Andrews, Gavin (2013). Andersson, Gerhard, ed. "The Effectiveness of Internet Cognitive Behavioural Therapy (iCBT) for Depression in Primary Care: A Quality Assurance Study". PLoS ONE. 8 (2): e57447. Bibcode:2013PLoSO...857447W. doi:10.1371/journal.pone.0057447. PMC 3579844. PMID 23451231.
- ↑ "CRE Publications | CRE". Comorbidity.edu.au. Retrieved 2014-08-14.
- ↑ http://www.seattleimplementation.org/wp-content/uploads/2011/12/ccp-78-5-737.pdf
- 1 2 Espie, Colin A.; Kyle, Simon D.; Williams, Chris; Ong, Jason C.; Douglas, Neil J.; Hames, Peter; Brown, June S.L. (2012). "A Randomized, Placebo-Controlled Trial of Online Cognitive Behavioral Therapy for Chronic Insomnia Disorder Delivered via an Automated Media-Rich Web Application". Sleep. 35 (6): 769–81. doi:10.5665/sleep.1872. PMC 3353040. PMID 22654196.
- ↑ (PDF) https://web.archive.org/web/20131203020947/http://www.bohrf.org.uk/downloads/Computerised_CBT-Sep2012.pdf. Archived from the original (PDF) on December 3, 2013. Retrieved January 29, 2013. Missing or empty
|title=(help) - ↑ https://web.archive.org/web/20121116020909/http://www.thementalelf.net/mental-health-conditions/anxiety-disorders/moodgym-no-better-than-informational-websites-according-to-new-workplace-rct. Archived from the original on November 16, 2012. Retrieved January 29, 2013. Missing or empty
|title=(help) - ↑ Spence, Susan H.; Donovan, Caroline L.; March, Sonja; Gamble, Amanda; Anderson, Renee E.; Prosser, Samantha; Kenardy, Justin (2011). "A randomized controlled trial of online versus clinic-based CBT for adolescent anxiety". Journal of Consulting and Clinical Psychology. 79 (5): 629–42. doi:10.1037/a0024512. PMID 21744945.
- ↑ "UKCP response to Andy Burnham's speech on mental health" (Press release). UK Council for Psychotherapy. 1 February 2012. Retrieved April 26, 2013.
- ↑ Leahy, Robert L. (November 23, 2011). "Cognitive-Behavioral Therapy: Proven Effectiveness". Psychology Today.
- ↑ Kirsch, Irving; Montgomery, Guy; Sapirstein, Guy (1995). "Hypnosis as an adjunct to cognitive-behavioral psychotherapy: A meta-analysis". Journal of Consulting and Clinical Psychology. 63 (2): 214–20. doi:10.1037/0022-006X.63.2.214. PMID 7751482.
- ↑ Alladin, Assen; Alibhai, Alisha (2007). "Cognitive Hypnotherapy for Depression:An Empirical Investigation". International Journal of Clinical and Experimental Hypnosis. 55 (2): 147–66. doi:10.1080/00207140601177897. PMID 17365072.
- ↑ Elkins, Gary; Johnson, Aimee; Fisher, William (2012). "Cognitive Hypnotherapy for Pain Management". American Journal of Clinical Hypnosis. 54 (4): 294–310. doi:10.1080/00029157.2011.654284. PMID 22655332.
- ↑ Butler, A; Chapman, J; Forman, E; Beck, A (2006). "The empirical status of cognitive-behavioral therapy: A review of meta-analyses". Clinical Psychology Review. 26 (1): 17–31. doi:10.1016/j.cpr.2005.07.003. PMID 16199119.
- ↑ Knouse, Laura E.; Safren, Steven A. (2010). "Current Status of Cognitive Behavioral Therapy for Adult Attention-Deficit Hyperactivity Disorder". Psychiatric Clinics of North America. 33 (3): 497–509. doi:10.1016/j.psc.2010.04.001. PMC 2909688. PMID 20599129.
- ↑ Thomson, Alex; Page, Lisa (2007). Thomson, Alex, ed. "Psychotherapies for hypochondriasis". Cochrane Database of Systematic Reviews (4): CD006520. doi:10.1002/14651858.CD006520.pub2. PMID 17943915.
- ↑ Thomas, Peter W; Thomas, Sarah; Hillier, Charles; Galvin, Kate; Baker, Roger (2006). Thomas, Peter W, ed. "Psychological interventions for multiple sclerosis". Cochrane Database of Systematic Reviews (1): CD004431. doi:10.1002/14651858.CD004431.pub2. PMID 16437487.
- ↑ Montgomery, Paul; Dennis, Jane A (2003). Montgomery, Paul, ed. "Cognitive behavioural interventions for sleep problems in adults aged 60+". Cochrane Database of Systematic Reviews (2): CD003161. doi:10.1002/14651858.CD003161. PMID 12076472.
- ↑ Proctor, Michelle; Murphy, Patricia A; Pattison, Helen M; Suckling, Jane A; Farquhar, Cindy (2007). Proctor, Michelle, ed. "Behavioural interventions for dysmenorrhoea". Cochrane Database of Systematic Reviews (3): CD002248. doi:10.1002/14651858.CD002248.pub3. PMID 17636702.
- 1 2 Costa, Rafael Thomaz da; Rangé, Bernard Pimentel; Malagris, Lucia Emmanoel Novaes; Sardinha, Aline; De Carvalho, Marcele Regine de; Nardi, Antonio Egidio (2010). "Cognitive–behavioral therapy for bipolar disorder". Expert Review of Neurotherapeutics. 10 (7): 1089–99. doi:10.1586/ern.10.75. PMID 20586690.
- ↑ Orgeta, V; Qazi, A; Spector, AE; Orrell, M (22 January 2014). "Psychological treatments for depression and anxiety in dementia and mild cognitive impairment.". The Cochrane database of systematic reviews. 1: CD009125. doi:10.1002/14651858.CD009125.pub2. PMID 24449085.
- ↑ O'Brian, S.; Onslow, M. (2011). "Clinical management of stuttering in children and adults". BMJ. 342: d3742. doi:10.1136/bmj.d3742. PMID 21705407.
- ↑ Iverach, L.; Menzies, R. G.; O'Brian, S.; Packman, A.; Onslow, M. (2011). "Anxiety and Stuttering: Continuing to Explore a Complex Relationship". American Journal of Speech-Language Pathology. 20 (3): 221–32. doi:10.1044/1058-0360(2011/10-0091). PMID 21478283.
- ↑ Menzies, Ross G.; Onslow, Mark; Packman, Ann; O'Brian, Sue (2009). "Cognitive behavior therapy for adults who stutter: A tutorial for speech-language pathologists". Journal of Fluency Disorders. 34 (3): 187–200. doi:10.1016/j.jfludis.2009.09.002. PMID 19948272.
- ↑ Edwards, Adrian GK; Hulbert-Williams, Nicholas; Neal, Richard D (2008). Edwards, Adrian GK, ed. "Psychological interventions for women with metastatic breast cancer". Cochrane Database of Systematic Reviews (3): CD004253. doi:10.1002/14651858.CD004253.pub3. PMID 18646104.
- ↑ Mitchell, Matthew D; Gehrman, Philip; Perlis, Michael; Umscheid, Craig A (2012). "Comparative effectiveness of cognitive behavioral therapy for insomnia: A systematic review". BMC Family Practice. 13 (1): 40. doi:10.1186/1471-2296-13-40. PMC 3481424. PMID 22631616.
- ↑ Chambers, D.; Bagnall, A.-M.; Hempel, S.; Forbes, C. (2006). "Interventions for the treatment, management and rehabilitation of patients with chronic fatigue syndrome/myalgic encephalomyelitis: An updated systematic review". Journal of the Royal Society of Medicine. 99 (10): 506–20. doi:10.1258/jrsm.99.10.506. PMC 1592057. PMID 17021301.
- ↑ "Cognitive behavioural therapy for the management of common mental health problems" (PDF). National Institute for Health and Clinical Excellence. April 2008. Retrieved 2013-11-04.
- ↑ Hoffman, Stefan G.; Smits, Jasper A. J. (2008). "Cognitive-Behavioral Therapy for Adult Anxiety Disorders". The Journal of Clinical Psychiatry. 69 (4): 621–32. doi:10.4088/JCP.v69n0415. PMC 2409267. PMID 18363421.
- ↑ "Definition of In Vivo Exposure". Ptsd.about.com. 2014-06-09. Retrieved 2014-08-14.
- ↑ Mowrer OH (1960). Learning theory and behavior. New York: Wiley. ISBN 0-88275-127-1.
- ↑ Bentz, Dorothée; Michael, Tanja; De Quervain, Dominique J.-F.; Wilhelm, Frank H. (October 29, 2009). "Enhancing exposure therapy for anxiety disorders with glucocorticoids: From basic mechanisms of emotional learning to clinical applications". Journal of Anxiety Disorders. 24 (2): 223–30. doi:10.1016/j.janxdis.2009.10.011. PMID 19962269. Retrieved 2014-10-26.
- ↑ Hirschfeld, Robert M.A. (2006). "Guideline Watch: Practice Guideline for the Treatment of Patients With Bipolar Disorder, 2nd Edition" (PDF). APA Practice Guidelines for the Treatment of Psychiatric Disorders: Comprehensive Guidelines and Guideline Watches. 1. doi:10.1176/appi.books.9780890423363.50051 (inactive 2015-04-14). ISBN 0-89042-336-9.
- 1 2 Neale JM, Davison GC (2001). Abnormal psychology (8th ed.). New York: John Wiley & Sons. p. 247. ISBN 0-471-31811-6.
- ↑ Wykes, T.; Steel, C.; Everitt, B.; Tarrier, N. (2007). "Cognitive Behavior Therapy for Schizophrenia: Effect Sizes, Clinical Models, and Methodological Rigor". Schizophrenia Bulletin. 34 (3): 523–37. doi:10.1093/schbul/sbm114. PMC 2632426. PMID 17962231.
- ↑ Kingdon, David; Price, Jessica (April 17, 2009). "Cognitive-behavioral Therapy in Severe Mental Illness". Psychiatric Times. 26 (5).
- ↑ Lynch, D.; Laws, K. R.; McKenna, P. J. (2009). "Cognitive behavioural therapy for major psychiatric disorder: Does it really work? A meta-analytical review of well-controlled trials". Psychological Medicine. 40 (1): 9–24. doi:10.1017/S003329170900590X. PMID 19476688.
- ↑ Gloaguen, Valérie; Cottraux, Jean; Cucherat, Michel; Blackburn, IM (1998). "A meta-analysis of the effects of cognitive therapy in depressed patients". Journal of Affective Disorders. 49 (1): 59–72. doi:10.1016/S0165-0327(97)00199-7. PMID 9574861.
- 1 2 Cox, W. T. L.; Abramson, L. Y.; Devine, P. G.; Hollon, S. D. (2012). "Stereotypes, Prejudice, and Depression: The Integrated Perspective". Perspectives on Psychological Science. 7 (5): 427–49. doi:10.1177/1745691612455204.
- ↑ Devine, Patricia G.; Forscher, Patrick S.; Austin, Anthony J.; Cox, William T.L. (2012). "Long-term reduction in implicit race bias: A prejudice habit-breaking intervention". Journal of Experimental Social Psychology. 48 (6): 1267–1278. doi:10.1016/j.jesp.2012.06.003. PMC 3603687. PMID 23524616.
- ↑ Jones C, Hacker D, Cormac I, Meaden A, Irving CB (2012). "Cognitive Behavioural Therapy versus other psychosocial treatments for schizophrenia". Cochrane Database of Systematic Reviews. 4: CD008712. doi:10.1002/14651858.CD008712.pub2. PMID 22513966.
- ↑ Bienenfeld, David (2009). "Cognitive therapy with older adults". Psychiatric Annals. 39 (9): 828–32. doi:10.3928/00485713-20090821-02.
- ↑ Seligman, Martin E. P.; Schulman, Peter; Derubeis, Robert J.; Hollon, Steven D. (1999). "The prevention of depression and anxiety". Prevention & Treatment. 2 (1). doi:10.1037/1522-3736.2.1.28a.
- ↑ Schmidt, Norman B.; Eggleston, A. Meade; Woolaway-Bickel, Kelly; Fitzpatrick, Kathleen Kara; Vasey, Michael W.; Richey, J. Anthony (2007). "Anxiety Sensitivity Amelioration Training (ASAT): A longitudinal primary prevention program targeting cognitive vulnerability". Journal of Anxiety Disorders. 21 (3): 302–19. doi:10.1016/j.janxdis.2006.06.002. PMID 16889931.
- ↑ Higgins, Diana M.; Hacker, Jeffrey E. (2008). "A Randomized Trial of Brief Cognitive-Behavioral Therapy for Prevention of Generalized Anxiety Disorder". The Journal of Clinical Psychiatry. 69 (8): 1336. doi:10.4088/JCP.v69n0819a. PMID 18816156.
- ↑ Meulenbeek, P.; Willemse, G.; Smit, F.; Van Balkom, A.; Spinhoven, P.; Cuijpers, P. (2010). "Early intervention in panic: Pragmatic randomised controlled trial". The British Journal of Psychiatry. 196 (4): 326–31. doi:10.1192/bjp.bp.109.072504. PMID 20357312.
- ↑ Gardenswartz, Cara Ann; Craske, Michelle G. (2001). "Prevention of panic disorder". Behavior Therapy. 32 (4): 725–37. doi:10.1016/S0005-7894(01)80017-4.
- ↑ Aune, Tore; Stiles, Tore C. (2009). "Universal-based prevention of syndromal and subsyndromal social anxiety: A randomized controlled study". Journal of Consulting and Clinical Psychology. 77 (5): 867–79. doi:10.1037/a0015813. PMID 19803567.
- ↑ van't Veer-Tazelaar, Petronella J.; Van Marwijk, HW; Van Oppen, P; Van Hout, HP; Van Der Horst, HE; Cuijpers, P; Smit, F; Beekman, AT (2009). "Stepped-Care Prevention of Anxiety and Depression in Late Life: A Randomized Controlled Trial". Archives of General Psychiatry. 66 (3): 297–304. doi:10.1001/archgenpsychiatry.2008.555. PMID 19255379.
- ↑ Stallard, P.; Sayal, K.; Phillips, R.; Taylor, J. A.; Spears, M.; Anderson, R.; Araya, R.; Lewis, G.; et al. (2012). "Classroom based cognitive behavioural therapy in reducing symptoms of depression in high risk adolescents: Pragmatic cluster randomised controlled trial". BMJ. 345: e6058. doi:10.1136/bmj.e6058. PMC 3465253. PMID 23043090.
- ↑ Clarke, G. N.; Hawkins, W.; Murphy, M.; Sheeber, L. (1993). "School-Based Primary Prevention of Depressive Symptomatology in Adolescents: Findings from Two Studies". Journal of Adolescent Research. 8 (2): 183–204. doi:10.1177/074355489382004.
- ↑ Cuijpers, Pim; Muñoz, Ricardo F.; Clarke, Gregory N.; Lewinsohn, Peter M. (2009). "Psychoeducational treatment and prevention of depression: The 'coping with depression' course thirty years later". Clinical Psychology Review. 29 (5): 449–58. doi:10.1016/j.cpr.2009.04.005. PMID 19450912.
- ↑ "Psychosis and schizophrenia in adults: updated NICE guidance for 2014". National Elf Service.
- ↑ "Psychosis and schizophrenia". nice.org.uk.
- ↑ Okuda, Mayumi; Balán, Iván; Petry, Nancy M.; Oquendo, Maria; Blanco, Carlos (2009-12-01). "Cognitive Behavioral Therapy for Pathological Gambling: Cultural Considerations". The American Journal of Psychiatry. 166 (12): 1325–1330. doi:10.1176/appi.ajp.2009.08081235. ISSN 0002-953X. PMC 2789341. PMID 19952084.
- ↑ "Cognitive–Behavioral Therapy for Pathological Gamblers" (PDF).
- ↑ Donald Robertson (2010). The Philosophy of Cognitive-Behavioural Therapy: Stoicism as Rational and Cognitive Psychotherapy. London: Karnac. p. xix. ISBN 978-1-85575-756-1.
- ↑ Mathews, John (2015). "Stoicism and CBT: Is Therapy A Philosophical Pursuit?". Virginia Counseling. Virginia Counseling.
- ↑ Beck AT, Rush AJ, Shaw BF, Emery G (1979). Cognitive Therapy of Depression. New York: Guilford Press. p. 8. ISBN 0-89862-000-7.
- ↑ Engler, B. (2006). Personality theories (7th Ed.) p. 424. Boston, MA: Houghton Mifflin Company.
- ↑ Robinson, D. N. (1995). An intellectual history of psychology (3rd Ed). Madison, WI: University of Wisconsin Press.
- 1 2 3 4 5 6 7 8 9 10 11 Trull, T. J. (2007). Clinical psychology (7th Ed). Belmont, CA: Thomson/Wadsworth.
- 1 2 3 4 5 6 Rachman, S (1997). "The evolution of cognitive behaviour therapy". In Clark, D; Fairburn, CG; Gelder, MG. Science and practice of cognitive behaviour therapy. Oxford: Oxford University Press. pp. 1–26. ISBN 0-19-262726-0.
- ↑ Jones, M. C. (1924). "The Elimination of Children's Fears". Journal of Experimental Psychology. 7 (5): 382–390. doi:10.1037/h0072283.
- 1 2 3 Corsini, R. J. & Wedding, D. (Eds.) (2008). Current psychotherapies (8th Ed.). Belmont, CA: Thomson Brooks/Cole.
- ↑ Wilson G.D. (1968). "Reversal of differential conditioning by instructions". Journal of Experimental Psychology. 76: 491–493. doi:10.1037/h0025540.
- ↑ Eysenck, H. J. (1952). "The effects of psychotherapy: An evaluation". Journal of Consulting Psychology. 16 (5): 319–24. doi:10.1037/h0063633. PMID 13000035.
- 1 2 3 4 5 Wilson, G. T. (2008). Behavior therapy. In R. J. Corsini & D. Wedding. Current psychotherapies (8th ed.). pp 63-106. Belmont, CA: Thomson Brooks/Cole.
- 1 2 Mosak H. H. & Maniacci, M. (2008). Adlerian psychotherapy. In R. J. Corsini & D. Wedding. Current psychotherapies (8th ed.). pp 63-106. Belmont, CA: Thomson Brooks/Cole.
- ↑ Ellis, A. (2008). Rational emotive behavior therapy. In R. J. Corsini & D. Wedding. Current psychotherapies (8th ed.). pp 63-106. Belmont, CA: Thomson Brooks/Cole.
- 1 2 3 Oatley, K. (2004). Emotions: A brief history p. 53. Malden, MA: Blackwell Publishing.
- ↑ Thorpe, G. L. & Olson, S. L. (1997). Behavior therapy: Concepts, procedures, and applications (2nd ed.). Boston, MA: Allyn & Bacon.
- ↑ Cognitive behavioural therapy for the management of common mental health problems (PDF). National Institute for Health and Care Excellence. April 2008.
- ↑ Kessler, David; Lewis, Glyn; Kaur, Surinder; Wiles, Nicola; King, Michael; Weich, Scott; Sharp, Debbie J; Araya, Ricardo; et al. (2009). "Therapist-delivered internet psychotherapy for depression in primary care: A randomised controlled trial". The Lancet. 374 (9690): 628–34. doi:10.1016/S0140-6736(09)61257-5. PMID 19700005.
- ↑ Hollinghurst, S.; Peters, T. J.; Kaur, S.; Wiles, N.; Lewis, G.; Kessler, D. (2010). "Cost-effectiveness of therapist-delivered online cognitive-behavioural therapy for depression: Randomised controlled trial". The British Journal of Psychiatry. 197 (4): 297–304. doi:10.1192/bjp.bp.109.073080. PMID 20884953.
- 1 2 3 4 5 6 Martin, Ben. "In-Depth: Cognitive Behavioral Therapy". PsychCentral. Retrieved March 15, 2012.
- ↑ Bender, S. & Messner, E. (2003). Becoming a therapist: What do I say, and why? (pp. 24, 34-35). New York, NY: The Guilford Press.
- 1 2 "Depression and anxiety – computerised cognitive behavioural therapy (CCBT)". National Institute for Health and Care Excellence. 2012-01-12. Retrieved 2012-02-04.
- ↑ Nordgren, L.B.; Hedman, E.; Etienne, J.; Bodin, J.; Kadowaki, A.; Eriksson, S.; Lindkvist, E.; Andersson, G.; et al. (August 2014). "Effectiveness and cost-effectiveness of individually tailored Internet-delivered cognitive behavior therapy for anxiety disorders in a primary care population: A randomized controlled trial". Behaviour Research and Therapy. 59: 1–11. doi:10.1016/j.brat.2014.05.007. PMID 24933451. Retrieved 18 August 2014.
- ↑ Marks, Isaac M.; Mataix-Cols, David; Kenwright, Mark; Cameron, Rachel; Hirsch, Steven; Gega, Lina (2003). "Pragmatic evaluation of computer-aided self-help for anxiety and depression". The British Journal of Psychiatry. 183: 57–65. doi:10.1192/bjp.183.1.57. PMID 12835245.
- 1 2 P. Musiata1 c1 and N. Tarriera1. "Cambridge Journals Online - Psychological Medicine - Abstract - Collateral outcomes in e-mental health: a systematic review of the evidence for added benefits of computerized cognitive behavior therapy interventions for mental health". Journals.cambridge.org. Retrieved 2014-08-14.
- ↑ MoodGYM was superior to informational websites in terms of psychological outcomes or service use
- ↑ Adelman CB, Panza KE, Bartley CA, Bontempo A, Bloch MH (2014). "A meta-analysis of computerized cognitive-behavioral therapy for the treatment of DSM-5 anxiety disorders". J Clin Psychiatry. 75: e695–704. doi:10.4088/JCP.13r08894. PMID 25093485.
- ↑ Andrews, G; Cuijpers, P; Craske, MG; McEvoy, P; Titov, N (13 October 2010). "Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: a meta-analysis.". PLOS ONE. 5 (10): e13196. doi:10.1371/journal.pone.0013196. PMC 2954140. PMID 20967242.
- 1 2 Freeman, J; Garcia, A; Frank, H; Benito, K; Conelea, C; Walther, M; Edmunds, J (2014). "Evidence base update for psychosocial treatments for pediatric obsessive-compulsive disorder.". Journal of Clinical Child and Adolescent Psychology. 43 (1): 7–26. doi:10.1080/15374416.2013.804386. PMID 23746138.
- ↑ Rozbroj, Tomas; et, al. (2014). "Assessing the Applicability of E-Therapies for Depression, Anxiety, and Other Mood Disorders Among Lesbians and Gay Men: Analysis of 24 Web- and Mobile Phone-Based Self-Help Interventions". Journal of Medical Internet Research. 16 (5): e166. doi:10.2196/jmir.3529. PMID 24996000.
- ↑ "A randomized controlled trial of the computerized CBT programme, MoodGYM, for public mental health service users waiting for interventions". British Journal of Clinical Psychology. 53: 433–450. doi:10.1111/bjc.12055. Retrieved 2014-08-14.
- ↑ "Understanding the acceptability of e-mental health - attitudes and expectations towards computerised self-help treatments for mental health problems".
- ↑ Spurgeon, Joyce A.; Wright, Jesse H. (2010). "Computer-Assisted Cognitive-Behavioral Therapy". Current Psychiatry Reports. 12 (6): 547–52. doi:10.1007/s11920-010-0152-4. PMID 20872100.
- ↑ Duggan, G.B. (2016). "Applying psychology to understand relationships with technology: from ELIZA to interactive healthcare". Behaviour and Information Technology. 35: 536–547. doi:10.1080/0144929X.2016.1141320.
- ↑ "Devon Partnership NHS Trust: Home" (PDF). NHS UK.
- ↑ "CG91 Depression with a chronic physical health problem". National Institute for Health and Care Excellence. 28 October 2009.
- ↑ Helgadóttir, Fjóla Dögg; Menzies, Ross G; Onslow, Mark; Packman, Ann; O'Brian, Sue (2009). "Online CBT I: Bridging the Gap Between Eliza and Modern Online CBT Treatment Packages". Behaviour Change. 26 (4): 245–53. doi:10.1375/bech.26.4.245.
- ↑ Helgadóttir, Fjóla Dögg; Menzies, Ross G; Onslow, Mark; Packman, Ann; O'Brian, Sue (2009). "Online CBT II: A Phase I Trial of a Standalone, Online CBT Treatment Program for Social Anxiety in Stuttering". Behaviour Change. 26 (4): 254–70. doi:10.1375/bech.26.4.254.
- ↑ (PDF) https://web.archive.org/web/20121024054235/http://www.mindinbexley.org.uk/docs/E-self_help_guide.pdf. Archived from the original (PDF) on October 24, 2012. Retrieved April 9, 2013. Missing or empty
|title=(help) - ↑ Williams, Christopher; Wilson, Philip; Morrison, Jill; McMahon, Alex; Andrew, Walker; Allan, Lesley; McConnachie, Alex; McNeill, Yvonne; et al. (2013). Andersson, Gerhard, ed. "Guided Self-Help Cognitive Behavioural Therapy for Depression in Primary Care: A Randomised Controlled Trial". PLoS ONE. 8 (1): e52735. Bibcode:2013PLoSO...852735W. doi:10.1371/journal.pone.0052735. PMC 3543408. PMID 23326352.
- ↑ Williams, C. (2001). "Use of written cognitive-behavioural therapy self-help materials to treat depression". Advances in Psychiatric Treatment. 7 (3): 233–40. doi:10.1192/apt.7.3.233.
- ↑ Haeffel, Gerald J. (2010). "When self-help is no help: Traditional cognitive skills training does not prevent depressive symptoms in people who ruminate". Behaviour Research and Therapy. 48 (2): 152–7. doi:10.1016/j.brat.2009.09.016. PMID 19875102.
- ↑ Gellatly, Judith; Bower, Peter; Hennessy, SUE; Richards, David; Gilbody, Simon; Lovell, Karina (2007). "What makes self-help interventions effective in the management of depressive symptoms? Meta-analysis and meta-regression". Psychological Medicine. 37 (9): 1217–28. doi:10.1017/S0033291707000062. PMID 17306044.
- ↑ Houghton, Simon; Saxon, Dave (2007). "An evaluation of large group CBT psycho-education for anxiety disorders delivered in routine practice". Patient Education and Counseling. 68 (1): 107–10. doi:10.1016/j.pec.2007.05.010. PMID 17582724.
- 1 2 3 Rudd, M. David (2012). "Brief cognitive behavioral therapy (BCBT) for suicidality in military populations". Military Psychology. 24 (6): 592–603. doi:10.1080/08995605.2012.736325.
- ↑ Choudhury, Koushiki (2013). Managing workplace stress: the cognitive behavioural way. New York: Springer India. ISBN 9788132206835.
- ↑ Ferguson, LM; Wormith, JS (September 2013). "A meta-analysis of moral reconation therapy.". International journal of offender therapy and comparative criminology. 57 (9): 1076–106. doi:10.1177/0306624x12447771. PMID 22744908.
- ↑ SAMHSA. "Moral Reconation Therapy". Retrieved 22 February 2015.
- 1 2 3 4 5 Meichenbaum, D (1996). "Stress Inoculation Training for Coping with Stressors". The Clinical Psychologist. 69: 4–7.
- 1 2 Tolin D. F. (2010). "Is cognitive-behavioral therapy more effective than other therapies? A meta-analytic review". Clinical Psychology Review. 30: 710–720. doi:10.1016/j.cpr.2010.05.003. PMID 20547435.
- 1 2 3 Cuijpers P.; van Straten A.; Andersson G.; Van Oppen P. (2008). "Psychotherapy for depression in adults: A meta-analysis of comparative outcome studies". Journal of Consulting and Clinical Psychology. 76 (6): 909–922. doi:10.1037/a0013075. PMID 19045960.
- 1 2 3 Glenn C. R.; Franklin J. C.; Nock M. K. (2014). "Evidence-based psychosocial treatments for self-injurious thoughts and behaviors in youth". Journal of Clinical Child and Adolescent Psychology. 44: 1–29. doi:10.1080/15374416.2014.945211. PMID 25256034.
- 1 2 Slife, B. D., & William, R. N. (1995). What’s behind the research? Discovering hidden assumptions in the behavioral sciences. Thousand Oaks, CA: Sage.
- 1 2 Fancher, R. T. (1995). Cultures of healing: Correcting the image of American mental health care. New York: W. H. Freeman and Company.
- 1 2 Berger, D. Psychiatric Times, July 30, 2013. http://www.psychiatrictimes.com/cognitive-behavioral-therapy/cognitive-behavioral-therapy-escape-binds-tight-methodology/page/0/1?cid=fb#sthash.ti9rtA48.dpuf
- ↑ Lynch D, Laws KR, McKenna PJ; Laws; McKenna (2010). "Cognitive behavioral therapy for major psychiatric disorder: does it really work? A meta-analytical review of well-controlled trials". Psychol Med. 40 (1): 9–24. doi:10.1017/S003329170900590X. PMID 19476688.
- ↑ Lincoln, TM (2010). "Letter to the editor: A comment on Lynch et al. (2009)". Psychological Medicine. 40 (5): 877–80. doi:10.1017/S0033291709991838. PMID 19917145.
- ↑ Kingdon, D (2010). "Over-simplification and exclusion of non-conforming studies can demonstrate absence of effect: A lynching party?". Psychological Medicine. 40 (1): 25–7. doi:10.1017/S0033291709990201. PMID 19570315.
- ↑ Wood, AM; Joseph, S (2010). "Letter to the Editor: An agenda for the next decade of psychotherapy research and practice". Psychological Medicine. 40 (6): 1055–6. doi:10.1017/S0033291710000243. PMID 20158935.
- ↑ Johnsen, TJ; Friborg, O (July 2015). "The effects of cognitive behavioral therapy as an anti-depressive treatment is falling: A meta-analysis.". Psychological Bulletin. 141 (4): 747–68. doi:10.1037/bul0000015. PMID 25961373.
- ↑ Nolen-Hoeksema, Susan (2014). Abnormal Psychology (6 ed.). McGraw-Hill Education. p. 357. ISBN 9781259060724.
- ↑ Chambless, D. L., Babich, K., Crits-Christoph, P., Frank, E., Gilson, M., & Montgomery, R. (1993). Task force on the promotion and dissemination of psychological procedures: A reported adopted by the Division 12 Board. Unpublished report.
- ↑ Fancher, R. T. (1995). Cultures of healing: Correcting the image of American mental health care (p. 231). New York: W. H. Freeman and Company.
- ↑ http://www.mayoclinic.org/tests-procedures/cognitive-behavioral-therapy/details/risks/cmc-20186935
- ↑ http://www.bbc.co.uk/science/0/23590545
- ↑ http://whatyoushouldknow.depression-alliance.co.uk/non-drug-treatments/cognitive-behavioural-therapy/
- ↑ http://www.nationalelfservice.net/treatment/psychotherapy/psychotherapy-trials-should-report-the-side-effects-of-treatment/
- ↑ http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0072481/
- 1 2 3 Laurance J (December 16, 2008). "The big question: can cognitive behavioural therapy help people with eating disorders?". The Independent. Retrieved April 22, 2012.
- ↑ Leader D (September 8, 2008). "A quick fix for the soul". The Guardian. Retrieved April 22, 2012.
- ↑ "CBT superiority questioned at conference". University of East Anglia. July 7, 2008. Retrieved April 22, 2012.
- 1 2 "UKCP response to Andy Burnham's speech on mental health" (Press release). UK Council for Psychotherapy. February 1, 2012. Retrieved April 22, 2012.
- ↑ "Psychosis and schizophrenia in adults: treatment and management". Retrieved February 2014. Check date values in:
|access-date=(help)
Further reading
- Aaron T. Beck (1979). Cognitive Therapy and the Emotional Disorders. Plume. ISBN 978-0-45200-928-8
- Butler G, Fennell M, and Hackmann A. (2008). Cognitive-Behavioral Therapy for Anxiety Disorders. New York: The Guilford Press. ISBN 978-1-60623-869-1
- Dattilio FM, Freeman A. (Eds.) (2007). Cognitive-Behavioral Strategies in Crisis Intervention (3rd ed.). New York: The Guilford Press. ISBN 978-1-60623-648-2
- Fancher, R. T. (1995). The Middlebrowland of Cognitive Therapy. In Cultures of Healing: Correcting the image of American mental healthcare. p. 195-250.
- Haggett, Ali (2016). 'Men, mental illness and suicide: the current scene in historical context'. History & Policy. http://www.historyandpolicy.org/policy-papers/papers/men-mental-illness-and-suicide-the-current-scene-in-historical-context
- Hofmann, SG. (2011). An Introduction to Modern CBT. Psychological Solutions to Mental Health Problems. Chichester, UK: Wiley-Blackwell. ISBN 0-470-97175-4.
- Willson R, Branch R. (2006). Cognitive Behavioural Therapy for Dummies. ISBN 978-0-470-01838-5
External links
| Library resources about Cognitive behavioral therapy |
- Association for Behavioral and Cognitive Therapies (ABCT)
- British Association for Behavioural and Cognitive Psychotherapies
- National Association of Cognitive-Behavioral Therapists
- Effective Child Therapy Public Service Website
- International Association of Cognitive Psychotherapy
- Information on CBT Treatments for various disorders
- Information on Research-based CBT Treatments