Cardiac catheterization

Cardiac catheterization (heart cath) is the insertion of a catheter into a chamber or vessel of the heart. This is done both for diagnostic and interventional purposes. Subsets of this technique are mainly coronary catheterization, involving the catheterization of the coronary arteries, and catheterization of cardiac chambers and valves of the cardiac system.
Procedure
"Cardiac catheterization" is a general term for a group of procedures that are performed using this method, such as coronary angiography and left ventricle angiography. Once the catheter is in place, it can be used to perform a number of procedures including angioplasty, percutaneous coronary intervention (PCI), balloon septostomy, electrophysiology study or catheter ablation.
Procedures can be diagnostic or therapeutic. For example, coronary angiography is a diagnostic procedure that allows the interventional cardiologist to visualize the coronary vessels. Percutaneous coronary intervention, however, involves the use of mechanical stents to increase blood flow to previously blocked (or occluded) vessels. Other common diagnostic procedures include measuring pressures throughout the four chambers of the heart and evaluating pressure differences across the major heart valves. Interventional cardiologists can also use cardiac catheterization to estimate the cardiac output, the amount of blood pumped by the heart per minute.[1]

Cardiac catheterization requires the use of fluoroscopy to visualize the path of the catheter as it enters the heart or as it enters the coronary arteries. The coronary arteries are known as "epicardial vessels" as they are located in the epicardium, the outermost layer of the heart.[2] Fluoroscopy can be conceptually described as continuous x-rays. The use of fluoroscopy requires radiopaque contrast, which in rare cases can lead to contrast-induced kidney injury (see Contrast-induced nephropathy).
There are two major categories of cardiac catheterization:[3]
- Left heart catheterization allows for direct intervention in cases of coronary artery occlusion. This technique is also used to assess the amount of occlusion (or blockage) in a coronary artery, often described as a percentage of occlusion. A thin, flexible wire is inserted into either the femoral artery or the radial artery and threaded toward the heart until it is in the ascending aorta. At this point, the wire can be maneuvered into the coronary ostia and into the coronary arteries. A catheter is guided over the wire and enters either the left or right coronary artery. In this position, the interventional cardiologist can inject contrast and visualize the flow through the vessel. If necessary, the physician can utilize percutaneous coronary intervention techniques, including the use of a stent (either bare-metal or drug-eluting) to open the blocked vessel and restore appropriate blood flow. In general, occlusions greater than 70% of the width of the vessel lumen are thought to require intervention. However, in cases where multiple vessels are blocked (so called "three vessel disease"), the interventional cardiologist may opt instead to refer the patient to a cardiothoracic surgeon for coronary artery bypass graft (CABG; see Coronary artery bypass surgery) surgery.
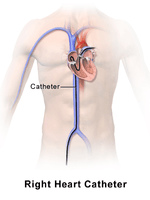
- Right heart catheterization allows the physician to determine the pressures within the heart (intracardiac pressures). In this case, the heart is most often accessed via the femoral vein; neither the femoral artery nor the radial artery are used. Values are commonly obtained for the right atrium, right ventricle, pulmonary arteries, and for the pulmonary capillary "wedge" pressures, which approximate the pressure values of the left-sided heart chambers. Right heart catheterizations also allow the physician to estimate the cardiac output, the amount of blood that flows from the heart each minute, and the cardiac index, a hemodynamic parameter that relates the cardiac output to a patient's body surface area. Determination of cardiac output can be done by releasing a small amount of normal saline in one area of the heart and measuring temperature changes over time in another area of the heart. It is important to note that the coronary arteries are not accessed during a right heart catheterization.
Coronary catheterization
Main page: Coronary catheterization
Indications for diagnostic use of coronary catheterization
Patients without cardiac symptoms or high-risk markers for a heart problem should not have a coronary catheterization to screen for problems.
Indications for cardiac catheterization include the following:
- Heart Attack (includes ST elevation MI, Non-ST Elevation MI, Unstable Angina)
- Abnormal Stress Test
- New-onset unexplained heart failure
- Survival of sudden cardiac death or dangerous cardiac arrhythmia
- Persistent chest pain despite optimal medical therapy
- Workup of suspected Prinzmetal Angina (coronary vasospasm)
Right heart catheterization, along with pulmonary function testing and other testing should be done to confirm pulmonary hypertension prior to having vasoactive pharmacologic treatments approved and initiated.[5]
Investigative techniques used with coronary catheterization
- to measure intracardiac and intravascular blood pressures
- to take tissue samples for biopsy
- to inject various agents for measuring blood flow in the heart; also to detect and quantify the presence of an intracardiac shunt
- to inject contrast agents in order to study the shape of the heart vessels and chambers and how they change as the heart beats
Catheterization of chambers and valves
Catheterization of cardiac chambers and valves may be performed at the same time as a coronary catheterization, and may also involve nearby major vessels, such as the aorta. It is the main method of cardiac ventriculography (another being radionuclide ventriculography, whose use has largely been replaced by echocardiography).
It has the ability to measure the pressure gradient across a valve and derive valve area from it. Thereby, it can assist in diagnosis of, for example, aortic stenosis.[6]
This is also the procedure used in balloon septostomy, which is the widening of a foramen ovale, patent foramen ovale (PFO), or atrial septal defect (ASD) using a balloon catheter.
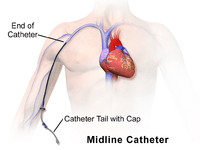
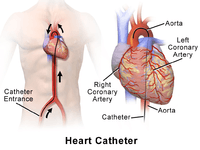
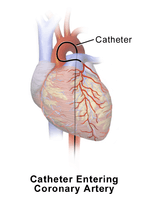
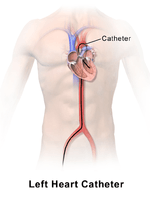
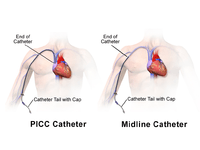
| Catheter Illustrations | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
History
The history of cardiac catheterization dates back to Claude Bernard (1813-1878), who used it on animal models. Clinical application of cardiac catheterization begins with Werner Forssmann in the 1930s, who inserted a catheter into the vein of his own forearm, guided it fluoroscopically into his right atrium, and took an X-ray picture of it. Forssmann won the Nobel Prize in Physiology or Medicine for this achievement, though hospital administrators removed him from his position owing to his unorthodox methods. During World War II, André Frédéric Cournand, a professor at Columbia University College of Physicians and Surgeons who also shared the Nobel Prize, and his colleagues developed techniques for left and right heart catheterization.
Dr. Eugene A. Stead, founder of the Physician Assistant profession, also performed research in the 1940s which paved the way for cardiac catheterization in medicine today.
References
- ↑ Harrison's Principles of Internal Medicine. McGraw-Hill. 2015.
- ↑ Malouf JF, Edwards WD, Tajik A, Seward JB. Chapter 4. Functional Anatomy of the Heart. In: Fuster V, Walsh RA, Harrington RA. eds. Hurst's The Heart, 13e. New York, NY: McGraw-Hill; 2011. http://accessmedicine.mhmedical.com/content.aspx?bookid=376&Sectionid=40279729. Accessed May 09, 2015.
- ↑ Leopold JA, Faxon DP. Diagnostic Cardiac Catheterization and Coronary Angiography. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson J, Loscalzo J.eds. 'Harrison's Principles of Internal Medicine, 19e. New York, NY: McGraw-Hill; 2015. http://accessmedicine.mhmedical.com/content.aspx?bookid=1130&Sectionid=79742087. Accessed May 09, 2015.
- ↑ Sabatine, edited by Marc S. (2011). Pocket medicine (4th ed.). Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 1608319059.
- ↑ American College of Chest Physicians; American Thoracic Society (September 2013), "Five Things Physicians and Patients Should Question", Choosing Wisely: an initiative of the ABIM Foundation, American College of Chest Physicians and American Thoracic Society, retrieved 6 January 2013
- ↑ Elizabeth D Agabegi; Agabegi, Steven S. (2008). Step-Up to Medicine (Step-Up Series). Hagerstwon, MD: Lippincott Williams & Wilkins. ISBN 0-7817-7153-6.
External links
- MedlinePlus Medical Encyclopedia: Cardiac catheterization
- eMedicine: Cardiac Catheterization (Left Heart)
- The Parachute Implant: a cardiac catheterization device for treating heart disease