Bone
| Bone | |
|---|---|
 A bone dating from the Pleistocene Ice Age of an extinct species of elephant. | |
 A scanning electronic micrograph of bone at 10,000x magnification. | |
| Identifiers | |
| MeSH | D001842 |
| TA | A02.0.00.000 |
| TH | H3.01.00.0.00001 |
| FMA | 30317 |
A bone is a rigid organ that constitutes part of the vertebral skeleton. Bones support and protect the various organs of the body, produce red and white blood cells, store minerals and also enable mobility as well as support for the body. Bone tissue is a type of dense connective tissue. Bones come in a variety of shapes and sizes and have a complex internal and external structure. They are lightweight yet strong and hard, and serve multiple functions. Mineralized osseous tissue, or bone tissue, is of two types, cortical and cancellous, and gives a bone rigidity and a coral-like three-dimensional internal structure. Other types of tissue found in bones include marrow, endosteum, periosteum, nerves, blood vessels and cartilage.
Bone is an active tissue composed of different types of bone cells. Osteoblasts and osteocytes are involved in the creation and mineralisation of bone; osteoclasts are involved in the reabsorption of bone tissue. The mineralised matrix of bone tissue has an organic component of mainly collagen called ossein and an inorganic component of bone mineral made up of various salts.
In the human body at birth, there are over 270 bones,[1] but many of these fuse together during development, leaving a total of 206 separate bones in the adult,[2] not counting numerous small sesamoid bones. The largest bone in the body is the thigh-bone (femur) and the smallest is the stapes in the middle ear.
Structure

Bone is not a uniformly solid material, but is mostly a matrix. The primary tissue of bone, bone tissue (osseous tissue), is relatively hard and lightweight. Its matrix is mostly made up of a composite material incorporating the inorganic mineral calcium phosphate in the chemical arrangement termed calcium hydroxylapatite (this is the bone mineral that gives bones their rigidity) and collagen, an elastic protein which improves fracture resistance.[3] Bone is formed by the hardening of this matrix around entrapped cells. When these cells become entrapped from osteoblasts they become osteocytes.
Layered structure
Cortical bone

The hard outer layer of bones is composed of cortical bone also called compact bone. Cortical referring to the outer (cortex) layer. The hard outer layer gives bone its smooth, white, and solid appearance, and accounts for 80% of the total bone mass of an adult human skeleton. However, that proportion may be much lower, especially in marine mammals and marine turtles, or in various Mesozoic marine reptiles, such as ichthyosaurs,[4] among others.[5]
Cortical bone consists of multiple microscopic columns, each called an osteon. Each column is multiple layers of osteoblasts and osteocytes around a central canal called the Haversian canal. Volkmann's canals at right angles connect the osteons together. The columns are metabolically active, and as bone is reabsorbed and created the nature and location of the cells within the osteon will change. Cortical bone is covered by a periosteum on its outer surface, and an endosteum on its inner surface. The endosteum is the boundary between the cortical bone and the cancellous bone. [6]
Cancellous bone

Filling the interior of the bone is the cancellous bone also known as trabecular or spongy bone tissue.[6] It is an open cell porous network. Thin formations of osteoblasts covered in endosteum create an irregular network of spaces.[7] Within these spaces are bone marrow and hematopoietic stem cells that give rise to platelets, red blood cells and white blood cells.[7] Trabecular marrow is composed of a network of rod- and plate-like elements that make the overall organ lighter and allow room for blood vessels and marrow. Trabecular bone accounts for the remaining 20% of total bone mass but has nearly ten times the surface area of compact bone.[8]
Bone marrow
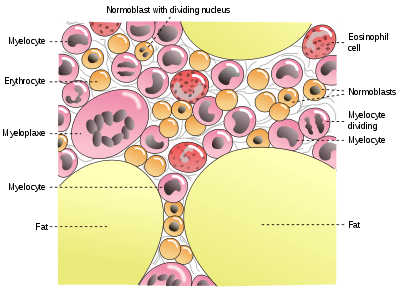
Bone marrow, also known as myeloid tissue, can be found in almost any bone that holds cancellous tissue. In newborns, all such bones are filled exclusively with red marrow, but as the child ages it is mostly replaced by yellow, or fatty marrow. In adults, red marrow is mostly found in the bone marrow of the femur, the ribs, the vertebrae and pelvic bones.
Composition
Cells

Bone is a metabolically active tissue composed of several types of cells. These cells include osteoblasts, which are involved in the creation and mineralization of bone tissue, osteocytes, and osteoclasts, which are involved in the reabsorption of bone tissue. Osteoblasts and osteocytes are derived from osteoprogenitor cells, but osteoclasts are derived from the same cells that differentiate to form macrophages and monocytes.[9] Within the marrow of the bone there are also hematopoietic stem cells. These cells give rise to other cells, including white blood cells, red blood cells, and platelets.[10]
- Osteoblasts are mononucleate bone-forming cells. They are located on the surface of osteoid seams and make a protein mixture known as osteoid, which mineralizes to become bone.[11] The osteoid seam is a narrow region of newly formed organic matrix, not yet mineralized, located on the surface of a bone. Osteoid is primarily composed of Type I collagen. Osteoblasts also manufacture hormones, such as prostaglandins, to act on the bone itself. They robustly produce alkaline phosphatase, an enzyme that has a role in the mineralisation of bone, as well as many matrix proteins.
- Osteocytes are mostly inactive osteoblasts.[9] Osteocytes originate from osteoblasts that have migrated into and become trapped and surrounded by bone matrix that they themselves produced.[6] The spaces they occupy are known as lacunae. Osteocytes have many processes that reach out to meet osteoblasts and other osteocytes probably for the purposes of communication.

- Osteoclasts are the cells responsible for bone resorption, thus they break down bone. New bone is then formed by the osteoblasts. Bone is constantly remodelled by the resorption of osteoclasts and created by osteoblasts.[9] Osteoclasts are large cells with multiple nuclei located on bone surfaces in what are called Howship's lacunae (or resorption pits). These lacunae are the result of surrounding bone tissue that has been reabsorbed.[12] Because the osteoclasts are derived from a monocyte stem-cell lineage, they are equipped with phagocytic-like mechanisms similar to circulating macrophages.[9] Osteoclasts mature and/or migrate to discrete bone surfaces. Upon arrival, active enzymes, such as tartrate resistant acid phosphatase, are secreted against the mineral substrate. The reabsorption of bone by osteoclasts also plays a role in calcium homeostasis.[12]
Extracellular
Bones consist of living cells embedded in a mineralized organic matrix. This matrix consists of organic components, mainly collagen – "organic" referring to materials produced as a result of the human body – and inorganic components, primarily hydroxyapatite and other salts of calcium and phosphate. Above 30% of the acellular part of bone consists of the organic components, and 70% of salts.[13] The strands of collagen give bone its tensile strength, and the interspersed crystals of hydroxyapatite give bone its compressional strength. These effects are synergistic.[13]

The inorganic composition of bone (bone mineral) is primarily formed from salts of calcium and phosphate, the major salt being hydroxyapatite (Ca10(PO4)6(OH)2).[13] The exact composition of the matrix may change over time and with nutrition, with the ratio of calcium to phosphate varying between 1.3 and 2.0 (per weight), and trace minerals such as magnesium, sodium, potassium and carbonate also being found.[13]
The organic part of matrix is mainly composed of Type I collagen.[13][14] Collagen composes 90–95% of the organic matrix, with remainder of the matrix being a homogenous liquid called ground substance consisting of proteoglycans such as hyaluronic acid and chondroitin sulfate.[13] Collagen consists of strands of repeating units, which give bone tensile strength, and are arranged in an overlapping fashion that prevents shear stress. The function of ground substance is not fully known.[13] Two types of bone can be identified microscopically according to the arrangement of collagen:
- Woven bone, (also known as fibrous bone) which is characterized by a haphazard organization of collagen fibers and is mechanically weak[15]
- Lamellar bone, which has a regular parallel alignment of collagen into sheets ("lamellae") and is mechanically strong [15]

Woven bone is produced when osteoblasts produce osteoid rapidly, which occurs initially in all fetal bones, but is later replaced by more resilient lamellar bone. In adults woven bone is created after fractures or in Paget's disease. Woven bone is weaker, with a smaller number of randomly oriented collagen fibers, but forms quickly; it is for this appearance of the fibrous matrix that the bone is termed woven. It is soon replaced by lamellar bone, which is highly organized in concentric sheets with a much lower proportion of osteocytes to surrounding tissue. Lamellar bone, which makes its first appearance in humans in the fetus during the third trimester,[16] is stronger and filled with many collagen fibers parallel to other fibers in the same layer (these parallel columns are called osteons). In cross-section, the fibers run in opposite directions in alternating layers, much like in plywood, assisting in the bone's ability to resist torsion forces. After a fracture, woven bone forms initially and is gradually replaced by lamellar bone during a process known as "bony substitution." Compared to woven bone, lamellar bone formation takes place more slowly. The orderly deposition of collagen fibers restricts the formation of osteoid to about 1 to 2 µm per day. Lamellar bone also requires a relatively flat surface to lay the collagen fibers in parallel or concentric layers.
Deposition
The extracellular matrix of bone is laid down by osteoblasts, which secrete both collagen and ground substance. These synthesise collagen within the cell, and then secrete collagen fibrils. The collagen fibres rapidly polymerise to form collagen strands. At this stage they are not yet mineralised, and are called "osteoid". Around the strands calcium and phosphate precipitate on the surface of these strands, within a days to weeks becoming crystals of hydroxyapatite.[13]
In order to mineralise the bone, the osteoblasts secrete vesicles containing alkaline phosphatase. This cleaves the phosphate groups and acts as the foci for calcium and phosphate deposition. The vesicles then rupture and act as a centre for crystals to grow on. More particularly, bone mineral is formed from globular and plate structures.[17][18]
Types

There are five types of bones in the human body: long, short, flat, irregular, and sesamoid.[19]
- Long bones are characterized by a shaft, the diaphysis, that is much longer than its width; and by an epiphysis, a rounded head at each end of the shaft. They are made up mostly of compact bone, with lesser amounts of marrow, located within the medullary cavity, and spongy, cancellous bone. Most bones of the limbs, including those of the fingers and toes, are long bones. The exceptions are the eight carpal bones of the wrist, the seven articulating tarsal bones of the ankle and the sesamoid bone of the kneecap. Long bones such as the clavicle, that have a differently shaped shaft or ends are also called modified long bones.
- Short bones are roughly cube-shaped, and have only a thin layer of compact bone surrounding a spongy interior. The bones of the wrist and ankle are short bones.
- Flat bones are thin and generally curved, with two parallel layers of compact bones sandwiching a layer of spongy bone. Most of the bones of the skull are flat bones, as is the sternum.
- Sesamoid bones are bones embedded in tendons. Since they act to hold the tendon further away from the joint, the angle of the tendon is increased and thus the leverage of the muscle is increased. Examples of sesamoid bones are the patella and the pisiform.
- Irregular bones do not fit into the above categories. They consist of thin layers of compact bone surrounding a spongy interior. As implied by the name, their shapes are irregular and complicated. Often this irregular shape is due to their many centers of ossification or because they contain bony sinuses. The bones of the spine, pelvis, and some bones of the skull are irregular bones. Examples include the ethmoid and sphenoid bones.[20]
Terminology
In the study of anatomy, anatomists use a number of anatomical terms to describe the appearance, shape and function of bones. Other anatomical terms are also used to describe the location of bones. Like other anatomical terms, many of these derive from Latin and Greek. Some anatomists still use Latin to refer to bones. The term "osseous", and the prefix "osteo-", referring to things related to bone, are still used commonly today.
Some examples of terms used to describe bones include the term "foramen" to describe a hole through which something passes, and a "canal" or "meatus" to describe a tunnel-like structure. A protrusion from a bone can be called a number of terms, including a "condyle", "crest", "spine", "eminence", "tubercle" or "tuberosity", depending on the protrusion's shape and location. In general, long bones are said to have a "head", "neck", and "body".
When two bones join together, they are said to "articulate". If the two bones have a fibrous connection and are relatively immobile, then the joint is called a "suture".
Development
The formation of bone is called ossification. During the fetal stage of development this occurs by two processes, Intramembranous ossification and endochondral ossification. Intramembranous ossification involves the creation of bone from connective tissue, whereas in the process of endochondral ossification bone is created from cartilage.
Intramembranous ossification
Intramembranous ossification mainly occurs during formation of the flat bones of the skull but also the mandible, maxilla, and clavicles; the bone is formed from connective tissue such as mesenchyme tissue rather than from cartilage. The steps in intramembranous ossification are:
- Development of ossification center
- Calcification
- Formation of trabeculae
- Development of periosteum
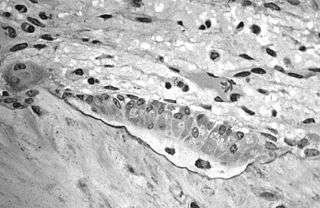
Endochondral ossification

.jpg)
Endochondral ossification, on the other hand, occurs in long bones and most of the rest of the bones in the body; it involves an initial hyaline cartilage that continues to grow. The steps in endochondral ossification are:
- Development of cartilage model
- Growth of cartilage model
- Development of the primary ossification center
- Development of the secondary ossification center
- Formation of articular cartilage and epiphyseal plate
Endochondral ossification begins with points in the cartilage called "primary ossification centers." They mostly appear during fetal development, though a few short bones begin their primary ossification after birth. They are responsible for the formation of the diaphyses of long bones, short bones and certain parts of irregular bones. Secondary ossification occurs after birth, and forms the epiphyses of long bones and the extremities of irregular and flat bones. The diaphysis and both epiphyses of a long bone are separated by a growing zone of cartilage (the epiphyseal plate). When the child reaches skeletal maturity (18 to 25 years of age), all of the cartilage is replaced by bone, fusing the diaphysis and both epiphyses together (epiphyseal closure). In the upper limbs, only the diaphyses of the long bones and scapula are ossified. The epiphyses, carpal bones, coracoid process, medial border of the scapula, and acromion are still cartilaginous.[21]
The following steps are followed in the conversion of cartilage to bone:
- Zone of reserve cartilage. This region, farthest from the marrow cavity, consists of typical hyaline cartilage that as yet shows no sign of transforming into bone.[22]
- Zone of cell proliferation. A little closer to the marrow cavity, chondrocytes multiply and arrange themselves into longitudinal columns of flattened lacunae.[22]
- Zone of cell hypertrophy. Next, the chondrocytes cease to divide and begin to hypertrophy (enlarge), much like they do in the primary ossification center of the fetus. The walls of the matrix between lacunae become very thin.[22]
- Zone of calcification. Minerals are deposited in the matrix between the columns of lacunae and calcify the cartilage. These are not the permanent mineral deposits of bone, but only a temporary support for the cartilage that would otherwise soon be weakened by the breakdown of the enlarged lacunae.[22]
- Zone of bone deposition. Within each column, the walls between the lacunae break down and the chondrocytes die. This converts each column into a longitudinal channel, which is immediately invaded by blood vessels and marrow from the marrow cavity. Osteoblasts line up along the walls of these channels and begin depositing concentric lamellae of matrix, while osteoclasts dissolve the temporarily calcified cartilage.[22]
Function
| Functions of Bone |
|---|
Mechanical
|
Synthetic
|
Metabolic
|
Bones have a variety of functions:
Mechanical
Bones serve a variety of mechanical functions. Together the bones in the body form the skeleton. They provide a frame to keep the body supported, and an attachment point for skeletal muscles, tendons, ligaments and joints, which function together to generate and transfer forces so that individual body parts or the whole body can be manipulated in three-dimensional space (the interaction between bone and muscle is studied in biomechanics).
Bones protect internal organs, such as the skull protecting the brain or the ribs protecting the heart and lungs. Because of the way that bone is formed, bone has a high compressive strength of about 170 MPa (1800 kgf/cm²),[3] poor tensile strength of 104–121 MPa, and a very low shear stress strength (51.6 MPa).[23][24] This means that bone resists pushing(compressional) stress well, resist pulling(tensional) stress less well, but only poorly resists shear stress (such as due to torsional loads). While bone is essentially brittle, bone does have a significant degree of elasticity, contributed chiefly by collagen. The macroscopic yield strength of cancellous bone has been investigated using high resolution computer models.[25]
Mechanically, bones also have a special role in hearing. The ossicles are three small bones in the middle ear which are involved in sound transduction.
Synthetic
Cancellous bones contain bone marrow. Bone marrow produces blood cells in a process called hematopoiesis.[26] Blood cells that are created in bone marrow include red blood cells, platelets and white blood cells.[27] Progenitor cells such as the hematopoietic stem cell divide in a process called mitosis to produce precursor cells. These include precursors which eventually give rise to white blood cells, and erythroblasts which give rise to red blood cells.[28] Unlike red and white blood cells, created by mitosis, platelets are shed from very large cells called megakaryocytes.[29] This process of progressive differentiation occurs within the bone marrow. After the cells are matured, they enter the circulation.[30] Every day, over 2.5 billion red blood cells and platelets, and 50–100 billion granulocytes are produced in this way.[10]
As well as creating cells, bone marrow is also one of the major sites where defective or aged red blood cells are destroyed.[10]
Metabolic
- Mineral storage — bones act as reserves of minerals important for the body, most notably calcium and phosphorus.
- Growth factor storage — mineralized bone matrix stores important growth factors such as insulin-like growth factors, transforming growth factor, bone morphogenetic proteins and others.
- Fat storage — the yellow bone marrow acts as a storage reserve of fatty acids.
- Acid-base balance — bone buffers the blood against excessive pH changes by absorbing or releasing alkaline salts.
- Detoxification — bone tissues can also store heavy metals and other foreign elements, removing them from the blood and reducing their effects on other tissues. These can later be gradually released for excretion.
- Endocrine organ — bone controls phosphate metabolism by releasing fibroblast growth factor – 23 (FGF-23), which acts on kidneys to reduce phosphate reabsorption. Bone cells also release a hormone called osteocalcin, which contributes to the regulation of blood sugar (glucose) and fat deposition. Osteocalcin increases both the insulin secretion and sensitivity, in addition to boosting the number of insulin-producing cells and reducing stores of fat.[31]
- Calcium balance—The process of bone resorption by the osteoclasts releases stored calcium into the systemic circulation and is an important process in regulating calcium balance. As bone formation actively fixes circulating calcium in its mineral form, removing it from the bloodstream, resorption actively unfixes it thereby increasing circulating calcium levels. These processes occur in tandem at site-specific locations.
Remodeling
Bone is constantly being created and replaced in a process known as remodeling. This ongoing turnover of bone is a process of resorption followed by replacement of bone with little change in shape. This is accomplished through osteoblasts and osteoclasts. Cells are stimulated by a variety of signals, and together referred to as a remodeling unit. Approximately 10% of the skeletal mass of an adult is remodelled each year.[32] The purpose of remodeling is to regulate calcium homeostasis, repair microdamaged bones from everyday stress, and also to shape and sculpt the skeleton during growth.. Repeated stress, such as weight-bearing exercise or bone healing, results in the bone thickening at the points of maximum stress (Wolff's law). It has been hypothesized that this is a result of bone's piezoelectric properties, which cause bone to generate small electrical potentials under stress.[33]
The action of osteoblasts and osteoclasts are controlled by a number of chemical enzymes that either promote or inhibit the activity of the bone remodeling cells, controlling the rate at which bone is made, destroyed, or changed in shape. The cells also use paracrine signalling to control the activity of each other. For example, the rate at which osteoclasts resorb bone is inhibited by calcitonin and osteoprotegerin. Calcitonin is produced by parafollicular cells in the thyroid gland, and can bind to receptors on osteoclasts to directly inhibit osteoclast activity. Osteoprotegerin is secreted by osteoblasts and is able to bind RANK-L, inhibiting osteoclast stimulation.[34]
Osteoblasts can also be stimulated to increase bone mass through increased secretion of osteoid and by inhibiting the ability of osteoclasts to break down osseous tissue. Increased secretion of osteoid is stimulated by the secretion of growth hormone by the pituitary, thyroid hormone and the sex hormones (estrogens and androgens). These hormones also promote increased secretion of osteoprotegerin.[34] Osteoblasts can also be induced to secrete a number of cytokines that promote reabsorbtion of bone by stimulating osteoclast activity and differentiation from progenitor cells. Vitamin D, parathyroid hormone and stimulation from osteocytes induce osteoblasts to increase secretion of RANK-ligand and interleukin 6, which cytokines then stimulate increased reabsorption of bone by osteoclasts. These same compounds also increase secretion of macrophage colony-stimulating factor by osteoblasts, which promotes the differentiation of progenitor cells into osteoclasts, and decrease secretion of osteoprotegerin.
Bone volume
Bone volume is determined by the rates of bone formation and bone resorption. Recent research has suggested that certain growth factors may work to locally alter bone formation by increasing osteoblast activity. Numerous bone-derived growth factors have been isolated and classified via bone cultures. These factors include insulin-like growth factors I and II, transforming growth factor-beta, fibroblast growth factor, platelet-derived growth factor, and bone morphogenetic proteins.[35] Evidence suggests that bone cells produce growth factors for extracellular storage in the bone matrix. The release of these growth factors from the bone matrix could cause the proliferation of osteoblast precursors. Essentially, bone growth factors may act as potential determinants of local bone formation.[35] Research has suggested that trabecular bone volume in postemenopausal osteoporosis may be determined by the relationship between the total bone forming surface and the percent of surface resorption.[36]
Clinical significance
A number of diseases can affect bone, including arthritis, fractures, infections, osteoporosis and tumours. Conditions relating to bone can be managed by a variety of doctors, including rheumatologists for joints, and orthopedic surgeons, who may conduct surgery to fix broken bones. Other doctors, such as rehabilitation specialists may be involved in recovery, radiologists in interpreting the findings on imaging, and pathologists in investigating the cause of the disease, and family doctors may play a role in preventing complications of bone disease such as osteoporosis.
When a doctor sees a patient, a history and exam will be taken. Bones are then often imaged, called radiography. This might include ultrasound X-ray, CT scan, MRI scan and other imaging such as a Bone scan, which may be used to investigate cancer.[37] Other tests such as a blood test for autoimmune markers may be taken, or a synovial fluid aspirate may be taken.[37]
Fractures
In normal bone, fractures occur when there is significant force applied, or repetitive trauma over a long time. Fractures can also occur when a bone is weakened, such as with osteoporosis, or when there is a structural problem, such as when the bone remodels excessively (such as Paget's disease) or is the site of the growth of cancer.[38] Common fractures include wrist fractures and hip fractures, associated with osteoporosis, vertebral fractures associated with high-energy trauma and cancer, and fractures of long-bones. Not all fractures are painful.[38] When serious, depending on the fractures type and location, complications may include flail chest, compartment syndromes or fat embolism. Compound fractures involve the bone's penetration through the skin.
Fractures and their underlying causes can be investigated by X-rays, CT scans and MRIs.[38] Fractures are described by their location and shape, and several classification systems exist, depending on the location of the fracture. A common long bone fracture in children is a Salter–Harris fracture.[39] When fractures are managed, pain relief is often given, and the fractured area is often immobilised. This is to promote bone healing. In addition, surgical measures such as internal fixation may be used. Because of the immobilisation, people with fractures are often advised to undergo rehabilitation.[38]
Tumors
There are several types of tumour that can affect bone; examples of benign bone tumours include osteoma, osteoid osteoma, osteochondroma, osteoblastoma, enchondroma, giant cell tumor of bone, aneurysmal bone cyst, and fibrous dysplasia of bone.
Cancer
Cancer can arise in bone tissue, and bones are also a common site for other cancers to spread (metastasise) to.[40] Cancers that arise in bone are called "primary" cancers, although such cancers are rare.[40] Metastases within bone are "secondary" cancers, with the most common being breast cancer, lung cancer, prostate cancer, thyroid cancer, and kidney cancer.[40] Secondary cancers that affect bone can either destroy bone (called a "lytic" cancer) or create bone (a "sclerotic" cancer). Cancers of the bone marrow inside the bone can also affect bone tissue, examples including leukemia and multiple myeloma. Bone may also be affected by cancers in other parts of the body. Cancers in other parts of the body may release parathyroid hormone or parathyroid hormone-related peptide. This increases bone reabsorption, and can lead to bone fractures.
Bone tissue that is destroyed or altered as a result of cancers is distorted, weakened, and more prone to fracture. This may lead to compression of the spinal cord, destruction of the marrow resulting in bruising, bleeding and immunosuppression, and is one cause of bone pain. If the cancer is metastatic, then there might be other symptoms depending on the site of the original cancer. Some bone cancers can also be felt.
Cancers of the bone are managed according to their type, their stage, prognosis, and what symptoms they cause. Many primary cancers of bone are treated with radiotherapy. Cancers of bone marrow may be treated with chemotherapy, and other forms of targeted therapy such as immunotherapy may be used.[41] Palliative care, which focuses on maximising a person's quality of life, may play a role in management, particularly if the likelihood of survival within five years is poor.
Painful conditions

- Osteomyelitis is inflammation of the bone or bone marrow due to bacterial infection.
- Osteogenesis imperfecta
- Osteochondritis dissecans
- Arthritis
- Ankylosing spondylitis
- Skeletal fluorosis is a bone disease caused by an excessive accumulation of fluoride in the bones. In advanced cases, skeletal fluorosis damages bones and joints and is painful.
Osteoporosis
Osteoporosis is a disease of bone where there is reduced bone mineral density, increasing the likelihood of fractures.[42] Osteoporosis is defined by the World Health Organization in women as a bone mineral density 2.5 standard deviations below peak bone mass, relative to the age and sex-matched average, as measured by Dual energy X-ray absorptiometry, with the term "established osteoporosis" including the presence of a fragility fracture.[43] Osteoporosis is most common in women after menopause, when it is called "postmenopausal osteoporosis", but may develop in men and premenopausal women in the presence of particular hormonal disorders and other chronic diseases or as a result of smoking and medications, specifically glucocorticoids.[42] Osteoporosis usually has no symptoms until a fracture occurs.[42] For this reason, DEXA scans are often done in people with one or more risk factors, who have developed osteoporosis and be at risk of fracture.[42]
Osteoporosis treatment includes advice to stop smoking, decrease alcohol consumption, exercise regularly, and have a healthy diet. Calcium supplements may also be advised, as may Vitamin D. When medication is used, it may include bisphosphonates, Strontium ranelate, and osteoporosis may be one factor considered when commencing Hormone replacement therapy.[44]
Osteology

The study of bones and teeth is referred to as osteology. It is frequently used in anthropology, archeology and forensic science for a variety of tasks. This can include determining the nutritional, health, age or injury status of the individual the bones were taken from. Preparing fleshed bones for these types of studies can involve the process of maceration.
Typically anthropologists and archeologists study bone tools made by Homo sapiens and Homo neanderthalensis. Bones can serve a number of uses such as projectile points or artistic pigments, and can also be made from external bones such as antlers.
Other animals

Bird skeletons are very lightweight. Their bones are smaller and thinner, to aid flight. Among mammals, bats come closest to birds in terms of bone density, suggesting that small dense bones are a flight adaptation. Many bird bones have little marrow due to their being hollow.[45]
A bird's beak is primarily made of bone as projections of the mandibles which are covered in keratin.
A deer's antlers are composed of bone which is an unusual example of bone being outside the skin of the animal once the velvet is shed.[46]
The extinct predatory fish Dunkleosteus had sharp edges of hard exposed bone along its jaws.
Many animals possess an exoskeleton that is not made of bone, These include insects and crustaceans.
Society and culture
Bones from slaughtered animals have a number of uses. In prehistoric times, they have been used for making bone tools. They have further been used in bone carving, already important in prehistoric art, and also in modern time as crafting materials for buttons, beads, handles, bobbins, calculation aids, head nuts, dice, poker chips, pick-up sticks, ornaments, etc. A special genre is scrimshaw.
Bone glue can be made by prolonged boiling of ground or cracked bones, followed by filtering and evaporation to thicken the resulting fluid. Historically once important, bone glue and other animal glues today have only a few specialized uses, such as in antiques restoration. Essentially the same process, with further refinement, thickening and drying, is used to make gelatin.
Broth is made by simmering several ingredients for a long time, traditionally including bones.
Ground bones are used as an organic phosphorus-nitrogen fertilizer and as additive in animal feed. Bones, in particular after calcination to bone ash, are used as source of calcium phosphate for the production of bone china and previously also phosphorus chemicals.
Bone char, a porous, black, granular material primarily used for filtration and also as a black pigment, is produced by charring mammal bones.
Oracle bone script was a writing system used in Ancient china based on inscriptions in bones.
To point the bone at someone is considered bad luck in some cultures, such as Australian aborigines, such as by the Kurdaitcha.
Osteopathic medicine is a school of medical thought originally developed based on the idea of the link between the musculoskeletal system and overall health, but now very similar to mainstream medicine. As of 2012, over 77,000 physicians in the United States are trained in Osteopathic medicine colleges.[47]
The wishbones of fowl have been used for divination, and are still customarily used in a tradition to determine which one of two people pulling on either prong of the bone may make a wish.
Various cultures throughout history have adopted the custom of shaping an infant's head by the practice of artificial cranial deformation. A widely practised custom in China was that of foot binding to limit the normal growth of the foot.
See also
| Wikimedia Commons has media related to Bones. |
| Wikiquote has quotations related to: Bone |
- Artificial bone
- Bone grafting
- Bone health
- Distraction osteogenesis
- Mineralized tissues
- National Bone Health Campaign
References
- ↑ Steele, D. Gentry; Claud A. Bramblett (1988). The Anatomy and Biology of the Human Skeleton. Texas A&M University Press. p. 4. ISBN 0-89096-300-2.
- ↑ Mammal anatomy : an illustrated guide. New York: Marshall Cavendish. 2010. p. 129. ISBN 9780761478829.
- 1 2 Schmidt-Nielsen, Knut (1984). "Scaling: Why Is Animal Size So Important?". Cambridge: Cambridge University Press: 6. ISBN 0-521-31987-0.
- ↑ de Buffrénil V.; Mazin J.-M. (1990). "Bone histology of the ichthyosaurs: comparative data and functional interpretation". Paleobiology. 16: 435–447. JSTOR 2400968.
- ↑ Laurin, M.; Canoville, A.; Germain, D. (2011). "Bone microanatomy and lifestyle: a descriptive approach". Comptes rendus Palevol. 10 (5–6): 381–402. doi:10.1016/j.crpv.2011.02.003.
- 1 2 3 Deakin 2006, p. 192.
- 1 2 Deakin 2006, p. 195.
- ↑ Hall, Susan J. (2007). Basic Biomechanics with OLC. (5th ed.,Revised. ed.). Burr Ridge: McGraw-Hill Higher Education. p. 88. ISBN 0-07-126041-2.
- 1 2 3 4 Deakin 2006, p. 189.
- 1 2 3 Deakin 2006, p. 58.
- ↑ Deakin 2006, pp. 189–190.
- 1 2 Deakin 2006, p. 190.
- 1 2 3 4 5 6 7 8 Hall 2005, p. 981.
- ↑ Harrisons 2008, p. 2365.
- 1 2 Currey, John D. (2002). "The Structure of Bone Tissue", pp. 12–14 in Bones: Structure and Mechanics. Princeton University Press. Princeton, NJ. ISBN 9781400849505
- ↑ Salentijn, L. Biology of Mineralized Tissues: Cartilage and Bone, Columbia University College of Dental Medicine post-graduate dental lecture series, 2007
- ↑ Bertazzo, S.; Bertran, C. A. (2006). "Morphological and dimensional characteristics of bone mineral crystals". Bioceramics. 309–311 (Pt. 1, 2): 3–10. doi:10.4028/www.scientific.net/KEM.309-311.3.
- ↑ Bertazzo, S.; Bertran, C.A.; Camilli, J.A. (2006). "Morphological Characterization of Femur and Parietal Bone Mineral of Rats at Different Ages". Key Engineering Materials. 309–311: 11–14. doi:10.4028/www.scientific.net/KEM.309-311.11.
- ↑ "Types of bone". mananatomy.com. Retrieved 6 February 2016.
- ↑ Pratt, Rebecca. "Bone as an Organ". AnatomyOne. Amirsys, Inc. Retrieved 2012-09-28.
- ↑ Agur, Anne (2009). Grant's Atlas of Anatomy. Philadelphia: Lippincott, Williams, and Wilkins. p. 598. ISBN 978-0-7817-7055-2.
- 1 2 3 4 5 Saladin, Kenneth (2012). Anatomy and Physiology: The Unity of Form and Function. New York: McGraw-Hill. p. 217. ISBN 978-0-07-337825-1.
- ↑ Vincent, Kevin. "Topic 3: Structure and Mechanical Properties of Bone". BENG 112A Biomechanics, Winter Quarter, 2013. Department of Bioengineering, University of California.
- ↑ Turner, C.H.; Wang, T.; Burr, D.B. (2001). "Shear Strength and Fatigue Properties of Human Cortical Bone Determined from Pure Shear Tests". Calcified Tissue International. 69 (6): 373–378. doi:10.1007/s00223-001-1006-1. PMID 11800235.
- ↑ Levrero, F.; Margetts, L.; et al. (2016). "Evaluating the macroscopic yield behaviour of trabecular bone using a nonlinear homogenisation approach". Journal of the Mechanical Behavior of Biomedical Materials. 61: 384–396. doi:10.1016/j.jmbbm.2016.04.008.
- ↑ Fernández, KS; de Alarcón, PA (December 2013). "Development of the hematopoietic system and disorders of hematopoiesis that present during infancy and early childhood.". Pediatric clinics of North America. 60 (6): 1273–89. doi:10.1016/j.pcl.2013.08.002. PMID 24237971.
- ↑ Deakin 2006, p. 60-61.
- ↑ Deakin 2006, p. 60.
- ↑ Deakin 2006, p. 57.
- ↑ Deakin 2006, p. 46.
- ↑ Lee, Na Kyung; et al. (10 August 2007). "Endocrine Regulation of Energy Metabolism by the Skeleton" (PDF). Cell. 130 (3): 456–469. doi:10.1016/j.cell.2007.05.047. PMC 2013746
 . PMID 17693256. Retrieved 2008-03-15.
. PMID 17693256. Retrieved 2008-03-15. - ↑ Manolagas, SC (April 2000). "Birth and death of bone cells: basic regulatory mechanisms and implications for the pathogenesis and treatment of osteoporosis.". Endocrine Reviews. 21 (2): 115–37. doi:10.1210/edrv.21.2.0395. PMID 10782361.
- ↑ ed, Russell T. Woodburne ..., consulting (1999). Anatomy, physiology, and metabolic disorders (5. print. ed.). Summit, N.J.: Novartis Pharmaceutical Corp. pp. 187–189. ISBN 0-914168-88-6.
- 1 2 Boulpaep, Emile L.; Boron, Walter F. (2005). Medical physiology: a cellular and molecular approach. Philadelphia: Saunders. pp. 1089–1091. ISBN 1-4160-2328-3.
- 1 2 Mohan, S.; Baylink, D. J. (1991). "Bone growth factors". Clinical Orthopaedics and Related Research (263): 30–48. doi:10.1097/00003086-199102000-00004. PMID 1993386.
- ↑ Nordin, BE; Aaron, J; Speed, R; Crilly, RG (8 August 1981). "Bone formation and resorption as the determinants of trabecular bone volume in postmenopausal osteoporosis". Lancet. 2 (8241): 277–9. doi:10.1016/S0140-6736(81)90526-2. PMID 6114324.
- 1 2 Britton 2010, pp. 1059–1062.
- 1 2 3 4 Britton 2010, pp. 1068.
- ↑ Salter RB, Harris WR (1963). "Injuries Involving the Epiphyseal Plate". J Bone Joint Surg Am. 45 (3): 587–622.
- 1 2 3 Britton 2010, pp. 1125.
- ↑ Britton 2010, pp. 1032.
- 1 2 3 4 Britton 2010, pp. 1116–1121.
- ↑ WHO (1994). "Assessment of fracture risk and its application to screening for postmenopausal osteoporosis. Report of a WHO Study Group". World Health Organization technical report series. 843: 1–129. PMID 7941614.
- ↑ Britton, the editors Nicki R. Colledge, Brian R. Walker, Stuart H. Ralston ; illustrated by Robert (2010). Davidson's principles and practice of medicine. (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. pp. 1116–1121. ISBN 978-0-7020-3085-7.
- ↑ Dumont, E. R. (17 March 2010). "Bone density and the lightweight skeletons of birds". Proceedings of the Royal Society B: Biological Sciences. 277 (1691): 2193–2198. doi:10.1098/rspb.2010.0117.
- ↑ Hans J. Rolf; Alfred Enderle (1999). "Hard fallow deer antler: a living bone till antler casting?". The Anatomical Record. 255 (1): 69–77. doi:10.1002/(SICI)1097-0185(19990501)255:1<69::AID-AR8>3.0.CO;2-R. PMID 10321994.
- ↑ "2012 OSTEOPATHIC MEDICAL PROFESSION REPORT" (PDF). Osteopathic.org. American Osteopathic Organisation. Retrieved 26 November 2014.
Footnotes
- Katja Hoehn; Marieb, Elaine Nicpon (2007). Human Anatomy & Physiology (7th Edition). San Francisco: Benjamin Cummings. ISBN 0-8053-5909-5.
- Bryan H. Derrickson; Tortora, Gerard J. (2005). Principles of anatomy and physiology. New York: Wiley. ISBN 0-471-68934-3.
- Britton, the editors Nicki R. Colledge, Brian R. Walker, Stuart H. Ralston ; illustated by Robert (2010). Davidson's principles and practice of medicine. (21st ed.). Edinburgh: Churchill Livingstone/Elsevier. ISBN 978-0-7020-3085-7.
- Deakin, Barbara Young; et al. (2006). Wheater's functional histology : a text and colour atlas (5th ed.). [Edinburgh?]: Churchill Livingstone/Elsevier. ISBN 978-0-443-068-508. – drawings by Philip J.
- Hall, Arthur C.; Guyton, John E. (2005). Textbook of medical physiology (11th ed.). Philadelphia: W.B. Saunders. ISBN 978-0-7216-0240-0.
- Anthony, S. Fauci; Harrison, T.R.; et al. (2008). Harrison's principles of internal medicine (17th ed.). New York [etc.]: McGraw-Hill Medical. ISBN 978-0-07-147692-8. – Anthony edits the current version; Harrison edited previous versions.
External links
- Educational resource materials (including animations) by the American Society for Bone and Mineral Research
- Review (including references) of piezoelectricity and bone remodelling
- A good basic overview of bone biology from the Science Creative Quarterly
- Usha Kini; B. N. Nandeesh. "Ch 2: Physiology of Bone Formation, Remodeling, and Metabolism". In Ignac Fogelman; Gopinath Gnanasegaran; Hans van der Wall. Radionuclide and hybrid bone imaging (PDF). Berlin: Springer. pp. 29–57. ISBN 978-3-642-02399-6.
- Bone histology photomicrographs