Birdshot chorioretinopathy
| Birdshot chorioretinopathy | |
|---|---|
| Classification and external resources | |
| Specialty | ophthalmology |
| ICD-10 | H30.9 |
| ICD-9-CM | 363.20 |
| OMIM | 605808 |
| DiseasesDB | 32404 |
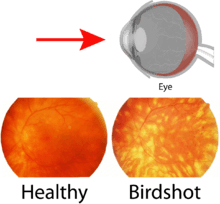
Birdshot chorioretinopathy is a rare form of bilateral posterior uveitis affecting the eye. It causes severe, progressive inflammation of both the choroid and retina.
Affected individuals are almost exclusively caucasian and usually diagnosed in the fourth to sixth decade of their lives.[1]
Pathophysiology
Birdshot chorioretinopathy is a rare form of posterior uveitis and accounts for 1-3% of uveitis cases in general. Birdshot chorioretinopathy is thought to be an autoimmune disease. The disease has strong association with the Human leukocyte antigen haplotype (HLA)-A29, which is the strongest association between a disease and HLA class I documented (85 to 97.5% of patients are HLA-A29 positive). This indicates a role for T-lymphocytes in the pathogenesis. Birdshot chorioretinopathy is associated with IL-17, a hallmark cytokine of TH17 cells that play an important role in autoimmunity .[2][3] The disease affects typically middle-aged or elderly caucasians. HLA-A29 is less prevalent in Asia and no birdshot chorioretinopathy cases have been reported in Asia. When birdshot chorioretinopathy is suspected, a person is usually tested to determine if they are HLA-A29 positive. However, HLA-A29 testing is not considered necessary for definitive diagnosis because HLA-A29 is also common in the general healthy population (7%). Additional (genetic or environmental) or unknown factors may be associated with HLA-A29 in the pathogenesis.
In 2014, Kuiper et al. conducted a genome-wide association study in birdshot chorioretinopathy and studied the entire genome of Dutch, Spanish and English patients. The GWAS identified, in addition to HLA-A29, the endoplasmic reticulum aminopeptidase (ERAP) 2 gene strongly associated with birdshot chorioretinopathy.[4] Genetic variants near ERAP2 on chromosome 5 resulted in high mRNA and protein expression of this aminopeptidase in BSCR patients. ERAP2 is an aminopeptidase that, together with the closely related ERAP1, trims peptides in the endoplasmic reticulum and loads these peptides on HLA molecules for presentation to T cells of the immune system. ERAP-HLA associations have also been reported in Ankylosing spondylitis and Behcet's disease, suggesting shared pathogenic pathways among these diseases.
Symptoms
Symptoms of this disorder include floaters, blurred vision, photopsia (flashing lights in eyes), loss of color vision and nyctalopia. In an eye examination, light-colored spots on the retina are seen. Complete loss of visual acuity may happen.
The name of the condition comes from the small light-colored fundus spots on the retina, scattered in a pattern like birdshot from a shotgun, but these spots might not be present in early stages.
Treatment
Birdshot chorioretinopathy may show resistance to treatment. Immunosuppressant therapy along with oral corticosteroid has been somewhat effective in slowing down the progressive inflammation associated with the disorder, preserving visual integrity as much as possible. Long-term use of such medications must be closely monitored, however, due to the discomforting and potentially debilitating and life-threatening side-effects.[5][5][6]
Immunosuppressive drugs such as the therapeutic monoclonal antibody daclizumab, ciclosporin and methotrexate have proven to be effective treatment options for birdshot chorioretinopathy. Substantial reduction and even stabilization of both vitreous inflammation and retinal vasculitis have been evident via electroretinography, during daclizumab (IL-2 receptor blocker) therapy. This is also supported by the observation of elevated levels of IL-2 in the eyes of patients.[2] Loss of visual acuity unrelated to the inflammation caused by the disorder, however, often remains unchanged despite usage of the drug. This is reflected by the lack of difference in visual acuity and the vision-related quality of life among various treatment categories in birdshot patients.[7] Contraindications and adverse side-effects are always a factor, as well.[8]
Support and advice
- Birdshot Uveitis Society
- International Birdshot Retinochoroidopathy Support Forum
- The Ocular Immunology and Uveitis Foundation Birdshot Support Group
References
- ↑ Cassoux N, Lehoan GP (2000). "Birdshot retinochoroidopathy". Ann Med Interne. 151 (Suppl. 1): 1s45–1s47. PMID 10896989.
- 1 2 Kuiper JJW, Mutis T, de Jager W, de Groot-Mijnes JD, Rothova A (2011). "Intraocular interleukin-17 and proinflammatory cytokines in HLA-A29-associated birdshot chorioretinopathy". Am J Ophthalmol. 152 (2): 177–182. doi:10.1016/j.ajo.2011.01.031. PMID 21570674.
- ↑ Kuiper JJW, Emmelot ME, Rothova A, Mutis T (2013). "Interleukin-17 production and T helper 17 cells in peripheral blood mononuclear cells in response to ocular lysate in patients with birdshot chorioretinopathy". Mol Vis. 27 (19): 2606–14. PMC 3874049
 . PMID 24379648.
. PMID 24379648. - ↑ Kuiper JJW, van Setten J, Ripke S, Van't Slot R, Mulder F, Missotten T, Baarsma GS, Francioli LC, Pulit SL, de Kovel CG, Ten Dam-van Loon N, den Hollander AI, Huis In Het Veld P, Hoyng CB, Cordero-Coma M, Martín J, Llorenç V, Arya B, Thomas D, Bakker SC, Ophoff RA, Rothova A, de Bakker PI, Mutis T, Koeleman BP (2014). "A genome-wide association study identifies a functional ERAP2 haplotype associated with birdshot chorioretinopathy". Hum Mol Genet. 23 (22): 6081–6087. doi:10.1093/hmg/ddu307. PMC 4204766. PMID 24957906.
- 1 2 Kiss S, Ahmed M, Letko E, Foster CS (2005). "Long-term follow-up of patients with birdshot retinochoroidopathy treated with corticosteroid-sparing systemic immunomodulatory therapy". Ophthalmology. 112 (6): 1066–1071. doi:10.1016/j.ophtha.2004.12.036. PMID 15936442.
- ↑ Becker MD, Wertheim MS, Smith JR, Rosenbaum JT (2005). "Long-term follow-up of patients with birdshot retinochoroidopathy treated with systemic immunosuppressants". Ocul Immuno Inflamm. 13 (4): 289–293. doi:10.1080/09273940490912407. PMID 16159719.
- ↑ Kuiper JJW, Missotten T, Baarsma SG, Rothova A (2013). "Vision-related quality of life in patients with birdshot chorioretinopathy". Acta Ophthalmol. 91 (1): 177–182. doi:10.1111/aos.12054. PMID 23289541.
- ↑ Sobrin L, Huang JJ, Christen W, Kafkala C, Choopong P, Foster CS (2008). "Daclizumab for treatment of birdshot chorioretinopathy". Arch Ophthalmol. 126 (2): 186–191. doi:10.1001/archophthalmol.2007.49. PMID 18268208.