Anterior interventricular branch of left coronary artery
| Anterior interventricular branch of left coronary artery | |
|---|---|
 Sternocostal surface of heart. Anterior descending branch labeled at upper right | |
| Details | |
| Source | left coronary artery |
| Branches | septals, diagonals |
| Supplies | anterolateral myocardium, apex, interventricular septum, 45-55% of the left ventricle (LV) |
| Identifiers | |
| Latin | ramus interventricularis anterior arteriae coronariae sinistrae |
| TA | A12.2.03.202 |
| FMA | 3862 |
The left anterior descending artery (also LAD, anterior interventricular branch of the left coronary artery, or anterior descending branch), of which infarction or stenosis is known as the "widow maker", is an artery of the heart.[1]
Structure
It passes at first behind the pulmonary artery and then comes forward between that vessel and the left auricula to reach the anterior interventricular sulcus, along which it descends to the incisura apicis cordis.
Although rare, multiple anomalous courses of the LAD have been described. These include the origin of the artery from the right sinus of valsalva.[2]
In 78% of cases, it reaches the apex of the heart.
Branches
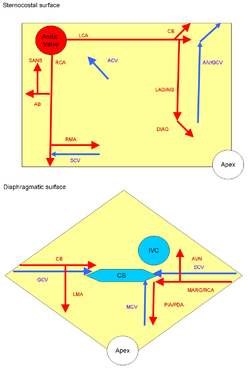
The LAD gives off two types of branches: septals and diagonals.
- Septals originate from the LAD at 90 degrees to the surface of the heart, perforating and supplying the anterior 2/3rds of the interventricular septum.
- Diagonals run along the surface of the heart and supply the lateral wall of the left ventricle and the anterolateral papillary muscle.
Function
The artery supplies the anterolateral myocardium, apex, and interventricular septum. The LAD typically supplies 45-55% of the left ventricle (LV) and is therefore considered the most critical vessel in terms of myocardial blood supply.
EKG changes associated with left anterior descending territory ischemia include ST segment changes in leads V1-V4, 1 and AVL.

Widow maker
The widow maker is an alternate name for the anterior interventricular branch of the left coronary artery.[3][1] The name widow maker may also apply to the left coronary artery[4] or severe occlusions to that artery.[5][6]
This term is used because the left main coronary, and/or the left anterior descending supply blood to large areas of the heart. This means that if these arteries are abruptly and completely occluded it will cause a massive heart attack that will likely lead to sudden death. The blockage that kills is made up of platelets streaming to the site of a ruptured cholesterol plaque. Even a small amount of plaque in this area can (for a variety of poorly understood reasons) rupture and cause death; bypassing chronic blockages or trying to open them up with angioplasty does not prevent heart attack but it can restore blood flow in case of a sudden blockage or heart attack and if performed within a rapid time period can minimize the damage done. An example of the devastating results of a complete occlusion of the LAD artery was the sudden death of former NBC News Washington Bureau Chief Tim Russert.[7]
From the minute a widow maker heart attack hits, survival time ranges from minutes to several hours. Rapidly progressing symptoms should signal the need for immediate attention. Symptoms of initial onset may include nausea, shortness of breath, pain in the head, jaw, arms or chest, numbness in fingers, often of a novel but imprecise sensation which builds with irregular heart beat. Early symptoms may be mistaken for food poisoning, flu or general malaise until they intensify. A widow maker cannot kill instantly but induces cardiac arrest which may do so within 10 to 20 minutes of no circulation. A victim with no pulse or breath is still alive, living off oxygen stored in the blood and may be able to be rescued if treatment is begun promptly within this window.[8]
Additional images
-
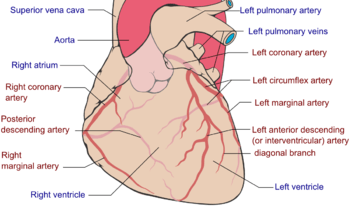
Coronary arteries (labeled in red text)
-
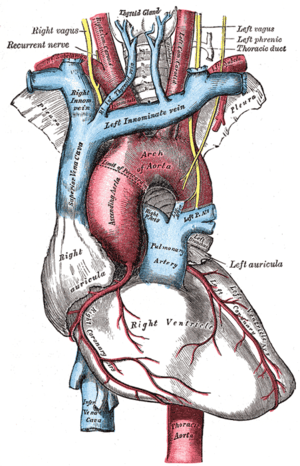
The arch of the aorta, and its branches.
-

Heart attack
-
Cardiac vessels
-

Human heart with coronary arteries
-

Heart coronary territories
References
This article incorporates text in the public domain from the 20th edition of Gray's Anatomy (1918)
- 1 2 Topol, Eric J.; Califf, Robert M. (2007). Textbook of Cardiovascular Medicine. Lippincott Williams & Wilkins. p. 283. ISBN 9780781770125. Retrieved 6 November 2014.
The most worrisome type is the proximal left anterior descending (LAD) MI, often referred to as the widow-maker infarction, which carries a high mortality and is attributed to an occlusion of the LAD before or at the first septal perforator.
- ↑ Ropers, D. (12 February 2002). "Anomalous Course of the Left Main or Left Anterior Descending Coronary Artery Originating From the Right Sinus of Valsalva: Identification of Four Common Variations by Electron Beam Tomography". Circulation. 105 (6): 42e–43. doi:10.1161/hc0602.102020.
- ↑ Lewis, Kathryn (1 December 2009). Multiple Lead ECGs: A Practical Analysis of Arrhythmias. Cengage Learning. p. 10. ISBN 9781435441248. Retrieved 6 November 2014.
The LAD is frequently implicated in sudden cardiac death, predominantly in adult males. Clinicians often refer to the LAD as the widow maker because obstruction here predisposes to a high incidence of sudden death.
- ↑ Barbara J. Aehlert; Robert Vroman (2011). "22". Paramedic Practice Today: Above and Beyond (1st ed.). Jones & Bartlett Publishers. p. 819. ISBN 978-0-323-08535-9. Retrieved 2 March 2015.
- ↑ Richard Beebe; Jeff Myers (11 December 2009). "34". Professional Paramedic, Volume I: Foundations of Paramedic Care. Cengage Learning. p. 764. ISBN 1-4283-2345-7. Retrieved 2 March 2015.
- ↑ Carlos S Restrepo; Dianna M. E. Bardo (1 January 2011). Cardiac Imaging. Thieme. p. 188. ISBN 978-1-60406-186-4. Retrieved 2 March 2015.
- ↑ Morgan, David (June 13, 2008). "TV newsman Tim Russert dies of heart attack". Reuters. Archived from the original on June 24, 2008. Retrieved June 13, 2008.
- ↑ Kearl, Mary (June 2009). "Surviving a Widow-Maker Heart Attack". AOL Health. Retrieved June 2009. Check date values in:
|access-date=(help)
External links
- Anatomy photo:20:09-0102 at the SUNY Downstate Medical Center - "Heart: The Left Coronary Artery and its Branches"
- Anatomy figure: 20:03-08 at Human Anatomy Online, SUNY Downstate Medical Center - "Anterior view of the heart."
- 168165435 at GPnotebook